


Abstract
The purpose of this investigation was to evaluate the use of a commercially available lactose-free fatty-meal food supplement, as an alternative to sincalide cholescintigraphy, to develop a standard methodology, and to determine normal gallbladder ejection fractions (GBEFs) for this supplement. Methods: Twenty healthy volunteers all had negative medical histories for hepatobiliary and gallbladder disease, had no personal or family history of hepatobiliary disease, and were not taking any medication known to affect gallbladder emptying. All were prescreened with a complete blood cell count, comprehensive metabolic profile, gallbladder and liver ultrasonography, and conventional cholescintigraphy. Three of the 20 subjects were eliminated from the final analysis because of an abnormality in one of the above studies. Results: After gallbladder filling on conventional cholescintigraphy, the subjects ingested the supplement and an additional 60-min study was acquired. GBEFs were calculated and ranged from 33% to 95% (mean ± SD, 62.6% ± 21.3%). Statistical analysis determined the lower range of normal to be 32.6%. Maximal gallbladder emptying occurred between 55 and 60 min. Conclusion: A standard methodology and normal GBEFs (≥33%) were established for supplement-stimulated cholescintigraphy.
Sincalide (Kinevac; Bracco Diagnostics) is routinely used for various indications in conjunction with cholescintigraphy (1). One common indication is to evaluate the adequacy of gallbladder contraction and to calculate a gallbladder ejection fraction (GBEF) in order to confirm or exclude the preoperative diagnosis of chronic acalculous cholecystitis (2,3). However, sincalide was not in production or available between November 2001 and December 2002. Alternative methods for evaluating gallbladder contraction became necessary.
Fatty meals have been used by investigators and clinicians over the years to evaluate gallbladder contraction in conjunction with oral cholecystography, ultrasonography, and cholescintigraphy. Proponents assert that fatty meals are physiologic and low in cost. Numerous different fatty meals have been used. Many are institution specific. Methodologies have differed, and few investigations have studied a sufficient number of subjects to establish valid normal GBEFs for the specific meal. Whole milk and half-and-half have the advantage of being simple to prepare and administer (4–7). Milk has been particularly well investigated. Large numbers of healthy subjects have been studied, a clear methodology described, and normal values determined (6–7). However, lactose intolerance is common and is associated with quite disagreeable symptoms. A commercially available standardized, prepackaged lactose-free meal would have advantages for clinical practice.
The purpose of this study was to investigate a commercially available lactose-free fatty-meal food supplement (Ensure Plus; Abbott Laboratories) containing sufficient fat to cause gallbladder contraction, to develop a standard methodology, and to determine normal GBEFs for this supplement.
MATERIALS AND METHODS
Twenty healthy paid volunteers (7 men, 13 women) were studied. They ranged in age from 21 to 47 y (mean ± SD, 33.2 ± 7.7 y) and weighed 59.8–94.5 kg (133–210 lb) (mean ± SD, 73.4 ± 13.5 kg [163 ± 30 lb]). All had negative medical histories for hepatobiliary and gallbladder disease, had no personal or family history of hepatobiliary disease, and were not taking any medication known to affect gallbladder emptying. Before the study, all underwent gallbladder/hepatobiliary ultrasonography, screening blood tests including complete blood cell count, comprehensive metabolic profile, and urinalysis. The investigational protocol was approved by the Georgetown University Hospital Institutional Review Board.
The subjects fasted for 4–12 h before cholescintigraphy. 99mTc-Mebrofenin (Choletec; Bracco Diagnostics) was injected intravenously with the patient supine. Conventional cholescintigraphy was performed (60 s/frame, 128 × 128) for 1 h using a large-field-of-view single-head gamma camera and a low-energy, all-purpose, parallel-hole collimator. Gallbladder filling occurred by 60 min in 19 of 20 subjects.
After voiding, the 19 subjects ingested a 240-mL (8 oz) can of the supplement (11.4 g of fat, 1,485 kJ [355 kcal], 50 g of carbohydrate) while sitting. Meal composition was identical regardless of nonnutritional flavoring (i.e., vanilla, chocolate, strawberry, etc.) Patients again lay supine, and images were acquired for 60 min (60 s/frame, 128 × 128) on a computer.
Computer processing was performed in a manner similar to that described previously by us for sincalide cholescintigraphy (8). On the computer display, regions of interest were drawn for the gallbladder and adjacent liver. Background- and decay-corrected time–activity curves were generated. GBEFs were calculated using the maximum counts minus the minimum counts divided by the maximum counts.
The GBEF data had a nongaussian distribution. Because of this and the number of subjects studied, an ad hoc method of statistical analysis was created. The smallest of GBEF observations is an estimate of the 5.6% point of the distribution; however, the lowest data value observed in the tail of the distribution may be unstable. To obtain a better estimate of the lower 5th percentile (5% point), the data were compared with a normal distribution and with an empiric model that fit a cubic polynomial to the cumulative distribution of GBEF (i.e., GBEF vs. percentage of subjects with an equal or smaller value). The normal distribution was systematically biased, whereas the cubic polynomial provided a nearly perfect fit over the limited data range. The estimated percentile that we report is the model-based, predicted GBEF value when the cumulative distribution is at 5%.
RESULTS
Not included in the final analysis were 3 of the 20 subjects. One had no gallbladder filling on 60-min cholescintigraphy and thus did not receive the supplement. A second subject had cholelithiasis on sonography. A third had a calculated GBEF calculation of 25% and on further review was found to have had a low GBEF on a past research study and thus was not believed to represent a truly healthy subject. All subjects found the supplement very palatable and ingested it within 5 min. No subject had adverse symptoms.
GBEFs ranged from 33% to 95% (mean ± SD, 62.6% ± 21.3%) (Table 1). Maximal emptying occurred at 60 min in 15 of 17 subjects and at 55 min in the other 2. The pattern of gallbladder-emptying time–activity curves varied considerably, that is, exponential, biexponential, linear, slow, rapid (Fig. 1). The time from the start of the second computer acquisition until the beginning of gallbladder emptying (lag phase) varied from 1 to 35 min (mean ± SD, 5.6 ± 8.2 min). The variability of ingestion time (maximum, 5 min) and of time required to lie down again on the imaging table and start the computer was not included in the lag phase. Only 2 subjects (subjects 4 and 16) (Table 1) had a lag phase greater than 7 min (15 and 35 min, respectively).
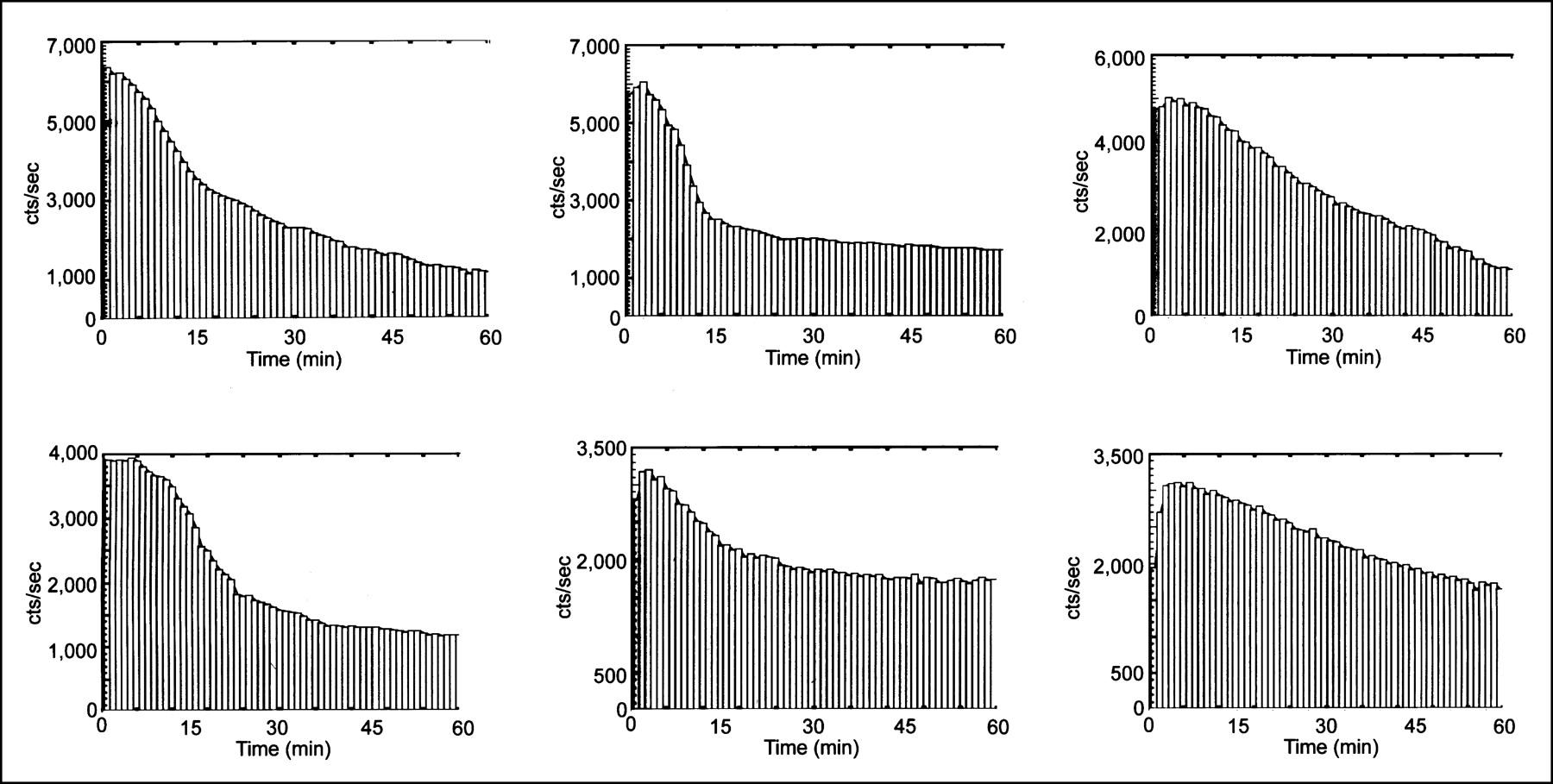
Supplement-stimulated gallbladder time–activity curves are shown for subjects 5, 7, 6, 4, 13, and 12 (from left to right and top to bottom). Curves for gallbladder emptying varied considerably, both in delay before emptying began and, most markedly, in pattern of emptying (linear, exponential, or biexponential).
Age, Sex, Weight, Lag Phase, and GBEF Values for All Subjects Who Ingested Supplement
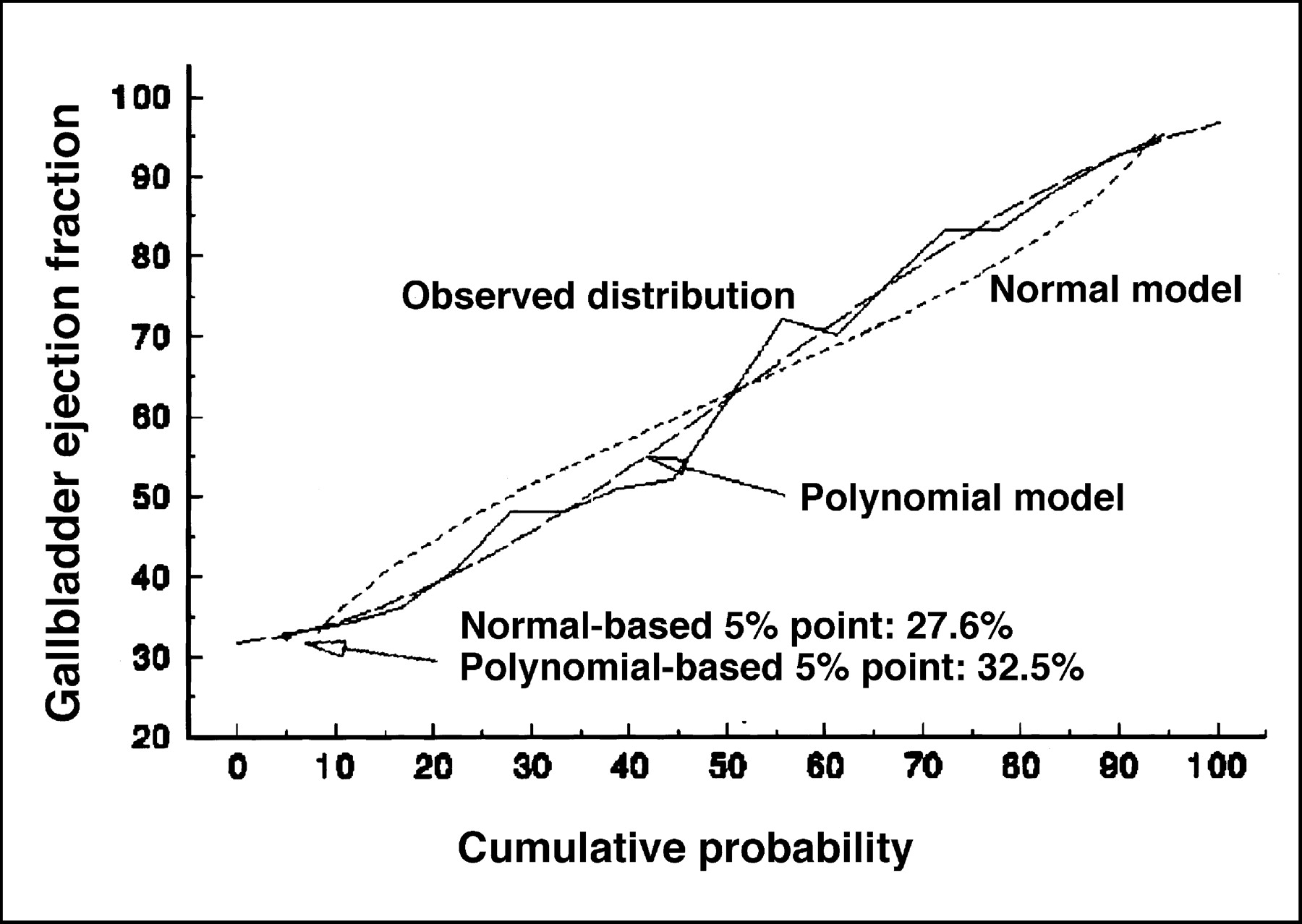
The lowest GBEF of the 17 healthy subjects was 33% (Table 1). This is an estimate of the 5.6% point of the distribution, close to the desired lower 5% point. However, observed values in the tail of the distribution may be quite unstable, and thus, a model-based analysis was used. The usual normal model yields an estimated lower 5% point of 27.6% for the distribution of GBEFs; this is the mean of 62.65% minus 1.645 times the SD of 21.34%. This is not the 95% lower confidence bound for the mean; that value would be 62.65% − 1.746 × 21.34%/√17 = 53.61%. The normal model is systematically biased (Fig. 2), since it predicts GBEFs that are too large below the median and too small above the median. A nearly perfect fit is obtained with a cubic polynomial (GBEF as a function of percentage cumulative distribution). The model has an adjusted R2 of 0.985, F3,13 = 360.8, P < 0.0001, for a test of fit. Although the cubic polynomial can be valid only within a limited range, it clearly fits well at the lower (and upper) tail of the distribution, where it implies that the lower 5th percentile of the GBEF distribution is 32.6%. The empiric 5.6% point of 33% GBEF and the model-based 5% point of 32.6% are in good agreement.

Cumulative distribution of GBEF observations for study subjects. Normal model is systematically biased, predicting GBEFs too large below median and too small above median. Nearly perfect fit is obtained with cubic polynomial.
DISCUSSION
Sincalide is commonly administered before or after cholescintigraphy for various indications (1). Before cholescintigraphy is performed, sincalide is infused to empty the gallbladder for patients who have been fasting more than 24 h or who are on total parenteral nutrition and, less commonly, for patients being evaluated for sphincter of Oddi dysfunction (9). After routine cholescintigraphy, sincalide can help differentiate biliary obstruction from other causes of delayed biliary-to-bowel transit and is probably most commonly used to evaluate gallbladder contraction and confirm or exclude the clinical diagnosis of chronic acalculous cholecystitis (2,3).
Sincalide is the only commercial analog of cholecystokinin (CCK) approved by the Food and Drug Administration (FDA) for clinical use. Pharmacy-compounded sincalide has been advocated as an alternative (10). Pharmacists can compound the raw chemical materials into a human product as part of the practice of pharmacy. Questions have been raised about quality control, sterility and toxicity testing, and liability issues (11). Quality control at regional pharmacies for sincalide does not meet U.S. Pharmacopoeia and FDA standards (12).
An alternative intravenous method of inducing gallbladder contraction is desirable and necessary for some indications. However, no other intravenous cholecystokinetic drug has been approved by the FDA. Intravenous erythromycin has an inotropic effect on gallbladder emptying (13). Although promising, early data suggest an inconsistent effect and a high incidence of adverse symptoms (14). Limited data suggest that subcutaneously injected bethanechol produces gallbladder contraction (15). Rectal distention has some cholecystokinetic effect (16); however, this is not likely to gain patient or physician acceptance.
Oral drugs or fatty meals can serve as an alternative to sincalide when a patient is able or permitted to ingest food. Magnesium sulfate has cholecystokinetic properties but is less effective than sincalide or fatty meals (17). A wide variety of fatty meals has been used, including dried egg yokes (18), a corned beef and cheese sandwich with milk (19), and even a Mars bar (20). Hospital-based nutritionists have devised fatty meals that vary from institution to institution. Cafeteria French fries are recommended by many of our technologists and residents. These methods are often not standardized and do not have established normal values. Milk products are readily available and require no preparation. Half-and-half has been investigated; however, the number of subjects studied is limited and normal values were assumed but not established (4,5). Two published reports have investigated the use of milk in a large number of healthy subjects (30 subjects in one study and 34 in the other), have described a clear methodology, and have established normal values (6,7).
However, lactose intolerance is common; thus, we sought a lactose-free fatty meal. Furthermore, a prepackaged commercial meal or food supplement would be convenient to prepare and administer in the clinic setting. Lipomul (Mead Johnson Laboratories), a corn-oil liquid meal, has been investigated and used clinically but is no longer manufactured by the company (21). The supplement that we chose for this study is widely available. It contains sufficient fat (11.4 g) to produce gallbladder contraction. Ten grams of fat are needed to produce good gallbladder emptying (22). The supplement is sold in 240-mL (8 oz) cans and comes in a variety of flavors. In our study, all subjects found the meal to be quite palatable and ingested it within 5 min without adverse symptoms.
We acquired and quantified images in a manner similar to our most recently reported sincalide methodology (8). In prior investigations, we reported that the dose and infusion length of sincalide directly affect the GBEF normal range (8,23). Normal values for fatty-meal cholescintigraphy also likely depend on the content of the meal and the methodology used. For example, if we had acquired the study for longer than 60 min further emptying would likely have occurred, because most patients had maximal emptying at 60 min (Fig. 1). The amount of fat in a meal likely affects GBEF normal values. Data are limited, however. One report found that 4 g of fat did not result in gallbladder contraction but that 10 and 20 g produced maximal gallbladder contraction (22). The gastric-emptying rate may also affect GBEF normal values. Delayed gastric emptying may delay endogenous production of CCK from the proximal small bowel. The more rapid gastric emptying that occurs in the upright position than in the supine position (24) may stimulate earlier production of endogenous CCK and greater gallbladder emptying during the study acquisition time (6,7).
CONCLUSION
We have described a standardized method for performing fatty-meal CCK cholescintigraphy using a commercially packaged low-lactose liquid food supplement and have established normal values with a lower limit of normal of 33% for that meal.
Footnotes
Received Dec. 12, 2002; revision accepted Mar. 24, 2003.
For correspondence or reprints contact: Harvey A. Ziessman, MD, Department of Radiology, Georgetown University Hospital, 3800 Reservoir Rd., NW, Washington, DC 20007.
E-mail: Ziessmah@gunet.georgetown.edu




{kind=link}
{kind=link}