


Abstract
For over 40 years, 18F-FDG has been the dominant PET tracer in neurology, cardiology, inflammatory diseases, and, most particularly, oncology. Combined with the ability to perform whole-body scanning, 18F-FDG has revolutionized the evaluation of cancer and has stifled the adoption of other tracers, except in situations where low avidity or high background activity limits diagnostic performance. The strength of 18F-FDG has generally been its ability to detect disease in the absence of structural abnormality, thereby enhancing diagnostic sensitivity, but its simultaneous weakness has been a lack of specificity due to diverse pathologies with enhanced glycolysis. Radiotracers that leverage other hallmarks of cancer or specific cell-surface targets are gradually finding a niche in the diagnostic armamentarium. However, none have had sufficient sensitivity to realistically compete with 18F-FDG for evaluation of the broad spectrum of malignancies. Perhaps, this situation is about to change with development of a class of tracers targeting fibroblast activation protein that have low uptake in almost all normal tissues but high uptake in most cancer types. In this review, the development and exciting preliminary clinical data relating to various fibroblast activation protein–specific small-molecule inhibitor tracers in oncology will be discussed along with potential nononcologic applications.
Inspired by Sokoloff’s autoradiographic assessment of cerebral glucose metabolism, David Kuhl approached the Brookhaven National Laboratory to develop a positron-emitting tracer of deoxyglucose for his new tomographic scanner. As a consequence, 18F-FDG, which Dr. Henry Wagner once described as being “the molecule of the 20th century,” was conceived. Roles in epilepsy (1), neurodegeneration (2), and ischemic heart disease (3) were initially described, but it was in oncology that 18F-FDG has most profoundly impacted the current practice of molecular imaging. This was accelerated by the development of whole-body scanning capability (4) and particularly PET/CT (5).
In the developed world, PET/CT is now widely used to diagnose, stage, and monitor treatment response with more accuracy, sparing inappropriate use of expensive and toxic therapies (6). 18F-FDG is by far the dominant tracer in oncology, despite increasing use of more specific tracers in certain malignancies, such as 68Ga-DOTA-octreotate in neuroendocrine neoplasia (7) and various prostate-specific membrane antigen tracers for prostate cancer evaluation (8,9). These two have become particularly important as part of theranostic paradigms including peptide receptor radionuclide therapy (10) and prostate-specific membrane antigen–based radioligand therapy (11), respectively. Similarly, high uptake of 18F-FDG in the brain has opened the way for amino acid analogs in the evaluation of brain tumors (12).
Despite the attraction of such tracers in advancing precision medicine and replacing standard nuclear medicine procedures (13), none have the broadly based appeal of 18F-FDG across the spectrum of malignancies in which it currently holds hegemony. For a tracer to compete, it would need to vie with 18F-FDG for sensitivity and surpass it with respect to specificity or, alternatively, offer the opportunity for theranostic application. Although data are preliminary, emerging evidence suggests that small-molecule fibroblast activation protein inhibitor (FAPI) tracers may be candidates for widespread oncologic application. In this review, the development and performance of FAPI PET/CT will be discussed along with possible therapeutic use. As with 18F-FDG, FAPI agents may also find an important diagnostic niche in nononcologic conditions.
THE ROLE OF CAFs IN CANCER
Although neoplastic cells have traditionally been thought to be primary determinants of cancer behavior, nonmalignant cells within the tumor microenvironment are increasingly recognized as modulators of both tumor progression and therapeutic response. Accordingly, the stromal compartment, including immune cells, vascular elements, and cancer-associated fibroblasts (CAFs), has been a focus of investigation. Key functions of CAFs are deposition and remodeling of extracellular matrix as part of a fibrotic reaction, which, when prominent in tumors such as pancreatic adenocarcinoma (14), is termed desmoplasia. However, CAFs are commonly found in solid tumor types without desmoplasia and therefore represent an attractive diagnostic and therapeutic target (15). Indeed, there is a concerted international effort to develop therapeutic agents targeting CAFs (16). Recently, it has become clear that the complex interplay of CAFs and immune cells can both suppress and accelerate tumor growth. This is likely to be driven by the significant biologic heterogeneity that has been identified in CAF subtypes both within and between cancers (17,18). The origins of CAFs are postulated to include activation of quiescent tissue fibroblasts, transdifferentiation of other stromal or epithelial cells, recruitment of circulating mesenchymal stem cells, or differentiation from tissue-resident stem cells (19). Any or all of these mechanisms may coexist, but how this ontogeny influences their biologic behavior remains to be fully elucidated. Epigenetic processes are thought to be involved in the development of protumorigenic CAFs (20).
One of the major impacts of CAFs is the development of an immunosuppressive tumor microenvironment (21) by processes including desmoplastic stroma excluding T cells from tumor deposits and secretion of various chemokines that recruit myeloid-derived suppressor cells and regulatory T cells. Chief among these is transforming growth factor β (22). The desmoplasia initiated by transforming growth factor β has recently been shown to be mediated through downregulation of signaling through the type I interferon receptor (23). CAFs also interact to alter the behavior of epithelial cancer cells through cell–cell interactions mediated by cadherins, cytokine signaling, and secretion of exosomes (24). Further, by modifying the extracellular matrix, CAFs are permissive for cancer invasion and tumor cell survival (25,26).
The biology and nomenclature of subsets of CAFs in different cancer types are still evolving (18), but recent advances, including single-cell technologies, have helped to define specialized subsets of CAFs (21). In pancreatic cancer, for instance, CAFs can be classified as myofibroblastic, inflammatory, and antigen-presenting (27).
FIBROBLAST ACTIVATION PROTEIN (FAP) AND CANCER BIOLOGY
FAP is a type II transmembrane glycoprotein belonging to the dipeptidyl peptidase IV–like family of postprolyl cleaving serine proteases that are expressed in dimeric form on the surface of CAFs (28); as such, FAP is an attractive diagnostic and therapeutic target. It plays a complex role in modulating the extracellular matrix (29). FAP differs from other members of the dipeptidyl peptidase family in acting as a gelatinase on denatured collagen, especially when cleaved by matrix metallopeptidases (30). Although the role of specific subtypes of CAFs in promoting or suppressing tumorigenesis remains controversial, it is becoming increasing clear that CAFs with high FAP expression are associated with an adverse prognosis by promoting invasion, angiogenesis, microenvironmental immune suppression, and metastasis (15). At least in part, this may reflect production of an immunosuppressive tumor microenvironment (31). Interestingly, in addition to expression on CAFs, FAP is also expressed on tumor-associated macrophages, which are important mediators of immune suppression (32). FAP has been shown to be important in recruitment of immunosuppressive myeloid-derived suppressor cells in cholangiocarcinoma (33). One of the potential effector molecules secreted by FAP-expressing CAFs is chemokine (C-X-C motif) ligand 12, which leads to polarization of macrophages to the immunosuppressive M2 phenotype (34) and also promotes angiogenesis in both breast (35) and colorectal carcinoma (36).
There is still much to learn about the biologic and clinical significance of FAP expression in different tumor types. For example, in the brain, where CAFs do not exist in the microenvironment, FAP overexpression has been found both in nonmalignant mesenchymal cells in the stroma and in transformed cells but had no association with prognosis (37). FAP expression was particularly associated with dysplastic blood vessels and highest in the mesenchymal subtype of glioblastoma. In a subsequent study of 13 patients with glioblastoma (38), no correlation was found with the apparent diffusion coefficient, which is generally associated with variation in prognosis. There was, however, significant intratumoral heterogeneity, with a relationship to better-perfused regions, possibly reflecting FAP expression in the neovasculature (39). Additionally, FAP expression is also seen in certain sarcomas and some benign mesenchymal tumors, including desmoid, giant cell tumors, and chondroblastoma (40), suggesting that FAP expression is not limited to CAFs.
Besides the opportunity that FAP provides as a diagnostic target, its high expression in several cancers with a poor response to current therapeutic approaches, including pancreatic (41) and ovarian carcinoma (42,43), makes it also an attractive therapeutic target. Even in more common and generally chemoresponsive tumors such as colorectal cancer, high FAP expression has also been found to be associated with poor prognosis (36,44). At least in preclinical models, use of chimeric antigen receptor T cells directed against FAP-expressing CAFs has been a successful therapeutic strategy (45). FAP is also being investigated as a target for antibody–drug conjugates (46). Accordingly, companion diagnostics would be valuable for selecting patients for such treatments or even for selecting patients for radioligand therapy. Importantly, FAP appears to be overexpressed across a diverse range of cancers (Fig. 1).

Cancer FAP expression results based on data generated by Cancer Genome Atlas Research Network (99). mRNA = messenger RNA; SCC = squamous cell carcinoma.
FAP AS A TARGET FOR IMAGING CANCER
Early attempts to develop FAP imaging probes involved radiolabeled antibodies. The 19F probe that had been used for immunohistochemical identification of FAP expression (47) was labeled with 131I and evaluated in patients with metastatic colorectal cancer (48). However, the long circulation time of intact antibodies poses logistic challenges and stimulated investigation of smaller molecules that may be suitable for imaging. It had long been known that novel dipeptides containing the boronic acid analog of proline could form potent yet nonselective inhibitors of the dipeptidyl peptidase family of peptidases (49). It was the introduction of the structurally similar 2-cyanopyrollidine that led to the discovery of FAPIs with increased selectivity and nanomolar affinity (50,51). By building on this work, the Heidelberg group based its first FAP-targeted tracers, FAPI-01 and FAPI-02, radiolabeled with 131I, and 68Ga, respectively, through chelation to DOTA (52).
Initial reports primarily involved preclinical validation (52,53). Compared with FAPI-01, FAPI-02 was found to specifically bind to FAP-expressing cells and have greater cellular retention. Internalization was confirmed using a fluorescent FAPI-02 with colocalization with endosomes. Small-animal PET demonstrated high and specific tumor uptake. Encouraged by these results, a preliminary human evaluation was performed on 3 patients, 1 each with metastatic breast, lung, and pancreatic cancer. All 3 patients had visualization of primary and metastatic disease but declining tumor uptake over 3 h. The primary route of excretion was renal, with little parenchymal retention. A series of variants based on FAPI-02 was designed to increase cellular retention. The most promising agent in preclinical models, FAPI-04, was tested in 2 women with metastatic breast cancer, demonstrating encouraging tumor visualization and a favorable biodistribution (54).
A further report expanded these preliminary clinical results in 50 patients equally split between 68Ga-FAPI-02 or 68Ga-FAPI-04 PET/CT (55). As suggested by the earlier reports, there was significantly greater washout of 68Ga-FAPI-02 than of 68Ga-FAPI-04 from tumor deposits at 1–3 h, but both performed comparably at 1 h, with clinically acceptable dosimetry. In 6 patients with contemporaneous 18F-FDG PET/CT available for direct correlation, comparable tumor SUV results were observed, except for 1 patient with iodine-negative thyroid cancer in whom 18F-FDG visualized several sites of disease not identified on FAPI PET/CT.
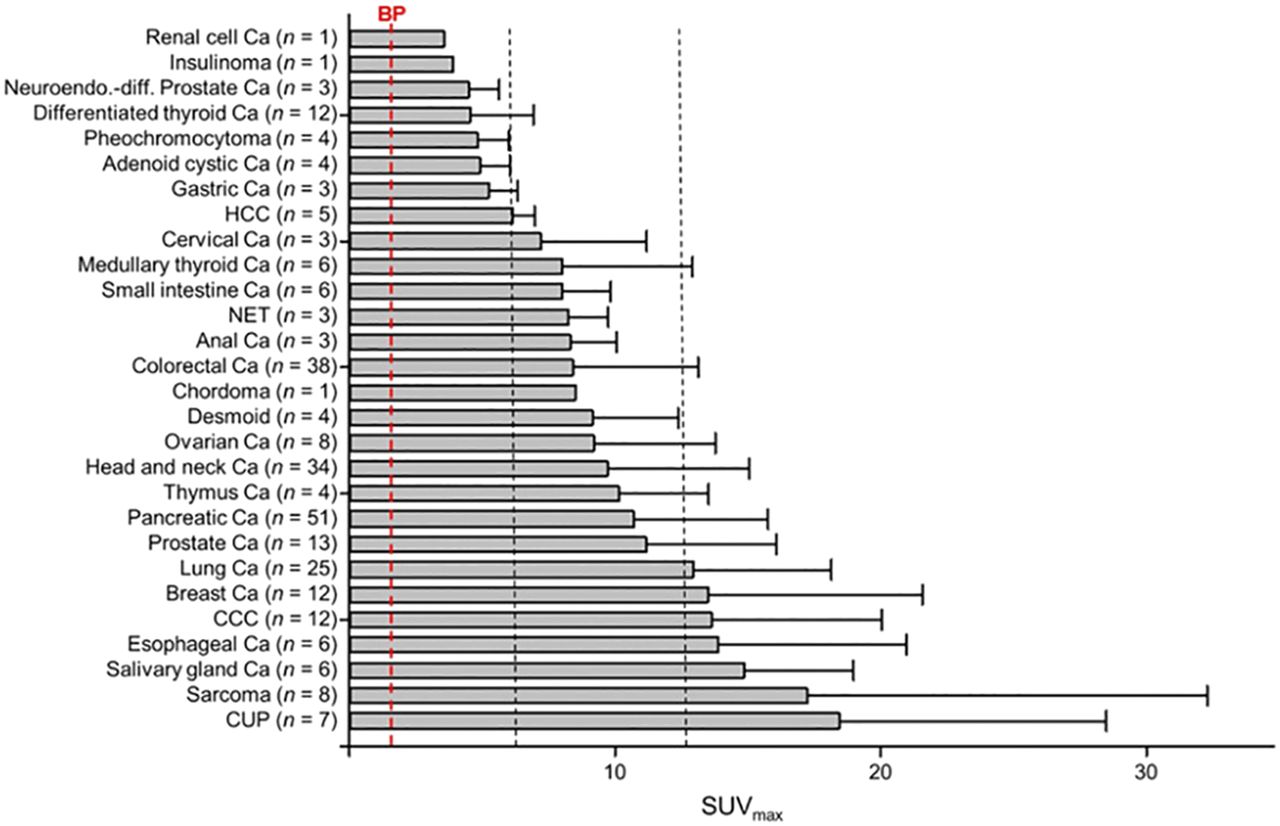
The Heidelberg experience with 68Ga-FAPI-04 was subsequently expanded to 80 patients with a range of cancers (56). Of 28 cancer types evaluated, the highest uptake (average SUVmax > 12) was observed in carcinoma of unknown primary, sarcoma, cholangiocarcinoma, and cancers of the esophagus, breast, and lung, but most had uptake significantly higher than that in the blood pool (Fig. 2). However, a case report from another group suggested that inflammatory conditions, such as IgG4-related disease, can also be positive (57). Similarly, another group evaluating 68Ga-FAPI-04 in 68 patients with equivocal 18F-FDG PET/CT findings found a small number of false-positive results related to inflammatory conditions despite clarifying the extent of disease in most patients (58). Another study evaluated 75 patients with FAPI-04, including 54 with 18F-FDG PET/CT correlation (59). Across 12 different cancer groupings, FAPI PET/CT identified more primary, nodal, and distant metastatic sites than did 18F-FDG PET/CT, with a significantly higher SUV in lung, pancreatic, and gastric cancer. The high tumor-to-background ratios provided by 68Ga-FAPI have been leveraged to guide radiotherapy planning in 14 patients with head and neck cancer (60), a site of complex anatomy and where muscular and brown fat activity can make 18F-FDG PET/CT difficult to interpret. Given that FAP seems to invoke an immune-excluded tumor microenvironment, FAPI imaging may potentially play a role in identifying patients who are less likely to respond to immune checkpoint inhibitor therapy (61).

Average SUVmax of 68Ga-FAPI PET/CT in various tumor entities in comparison to blood pool. Ca = cancer; CCC = cholangiocellular carcinoma; CUP = carcinoma of unknown primary; HCC = hepatocellular carcinoma; NET = neuroendocrine tumor; neuroendo.-diff. = neuroendocrine differentiation. (Reprinted with permission of (56).)
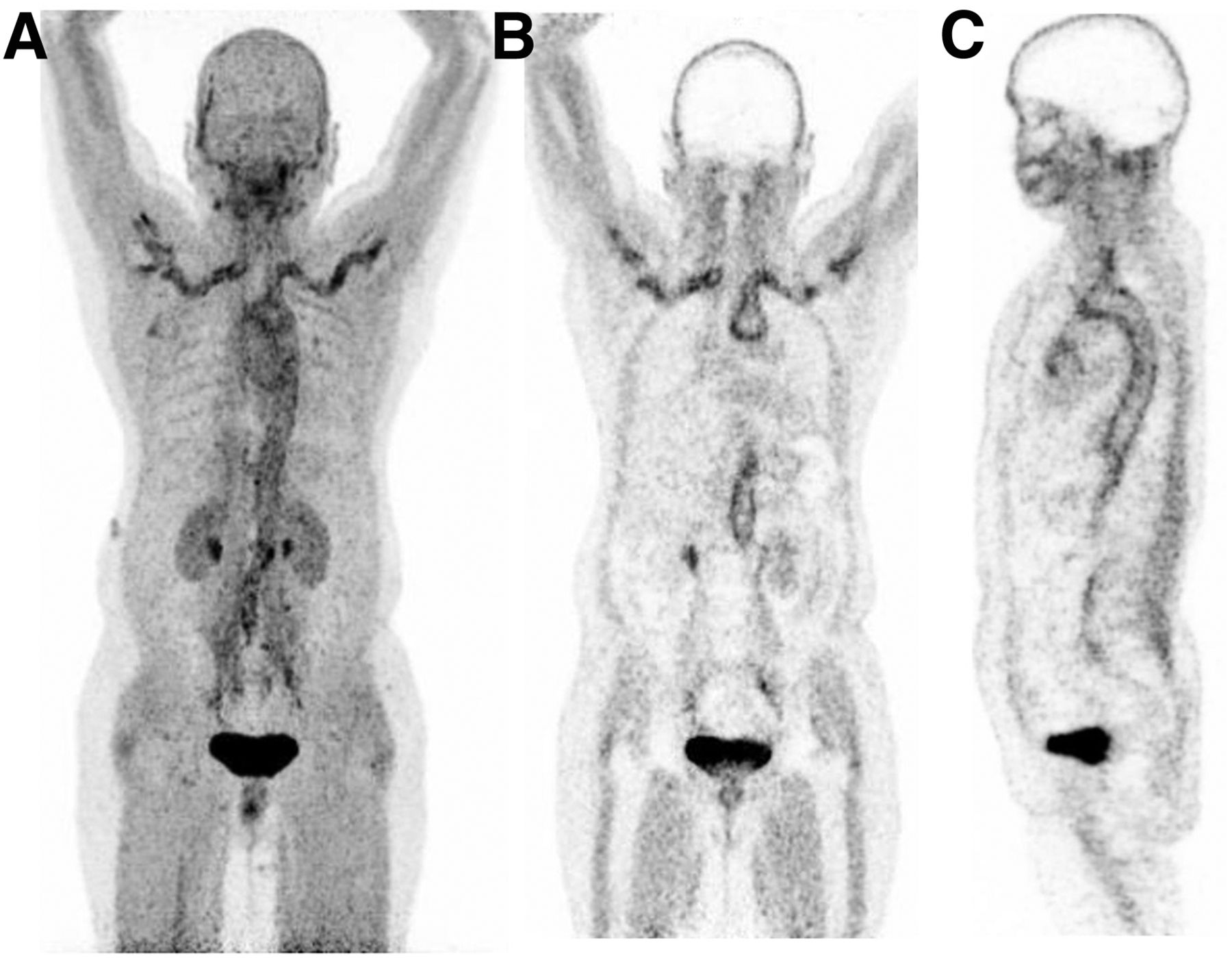
The Heidelberg group continued to experiment with variations on FAPI-04 using chemical adaptations, including alteration of lipophilicity and modification of the DOTA/linker attachment at the quinoline moiety to improve tumor retention (53). On the basis of cell culture and preclinical imaging, 2 lead compounds entered clinical evaluation in 8 patients. These were designated FAPI-21 and FAPI-46. Although both had high tumor uptake, FAPI-21 inexplicably had higher uptake in the major salivary glands, mouth, and thyroid, rendering 68Ga-FAPI-46 the leading candidate for clinical evaluation. Formal dosimetry studies performed on 6 patients were favorable (62). The main off-target organs to receive radiation were, as expected, the urinary bladder and kidneys. This suggests that adequate hydration and frequent voiding would be protective in the therapeutic setting. From a combination of scans with 68Ga-FAPI-04 (n = 16) and 68Ga-FAPI-46 (n = 6), promising results were reported in tumors of the lower gastrointestinal tract (63). Stage was changed in 50% of patients without prior treatment, with significantly more metastases being identified in those with already known metastasis, and management was changed in 17 of 21 evaluable patients. However, relatively few of these patients had been staged with 18F-FDG PET/CT. The study included 6 patients with anal cancer, which can be difficult to assess because of physiologic 18F-FDG uptake in sphincteric muscle. Low bowel activity is a potential advantage of FAPI in delineating peritoneal disease (Fig. 3).

Peritoneal carcinomatosis. (A) 18F-FDG PET maximum-intensity-projection image demonstrates focal uptake in region of cecum and transverse colon but impression of diffuse peritoneal disease. (B) Corresponding FAPI-04 PET maximum-intensity projection clearly demonstrates diffuse peritoneal disease including involvement of subphrenic spaces.
In a further advance, an 18F-labeled agent, FAPI-74, was recently described that uses an aluminum-fluoride labeling method on a precursor that can also be labeled as a cold kit using 68Ga (64). Evaluation in 10 patients with lung cancer revealed somewhat higher vascular visualization than that obtained with FAPI-02 or FAPI-04 but high tumor uptake enabling radiotherapy planning. Radiosynthesis and preclinical evaluation of another fluorinated FAPI tracer, 18FGlc‐FAPI, has also been recently described (65). This agent had higher hepatobiliary clearance than 68Ga-FAPI-04. There is currently limited information on the clinical performance of this tracer.
Low uptake of FAPI agents in the brain is a potential advantage over 18F-FDG for evaluation of both primary and secondary malignancies (Fig. 4). Recognition of cerebral metastasis (66) and leptomeningeal disease (67) has been reported in individual patients with adenocarcinoma of the lung. However, uptake may not necessarily be specific for malignancy, with infectious etiologies such as tuberculosis also demonstrating increased activity (68). In a series of patients with various primary brain tumors, uptake of 68Ga-FAPI-02 or 68Ga-FAPI-04 was observed in all isocitrate dehydrogenase wild-type glioblastomas and in higher-grade isocitrate dehydrogenase mutant gliomas (38). In a preliminary evaluation, the potential application of FAPI PET/CT or PET/MRI for radiotherapy planning has been described (69).
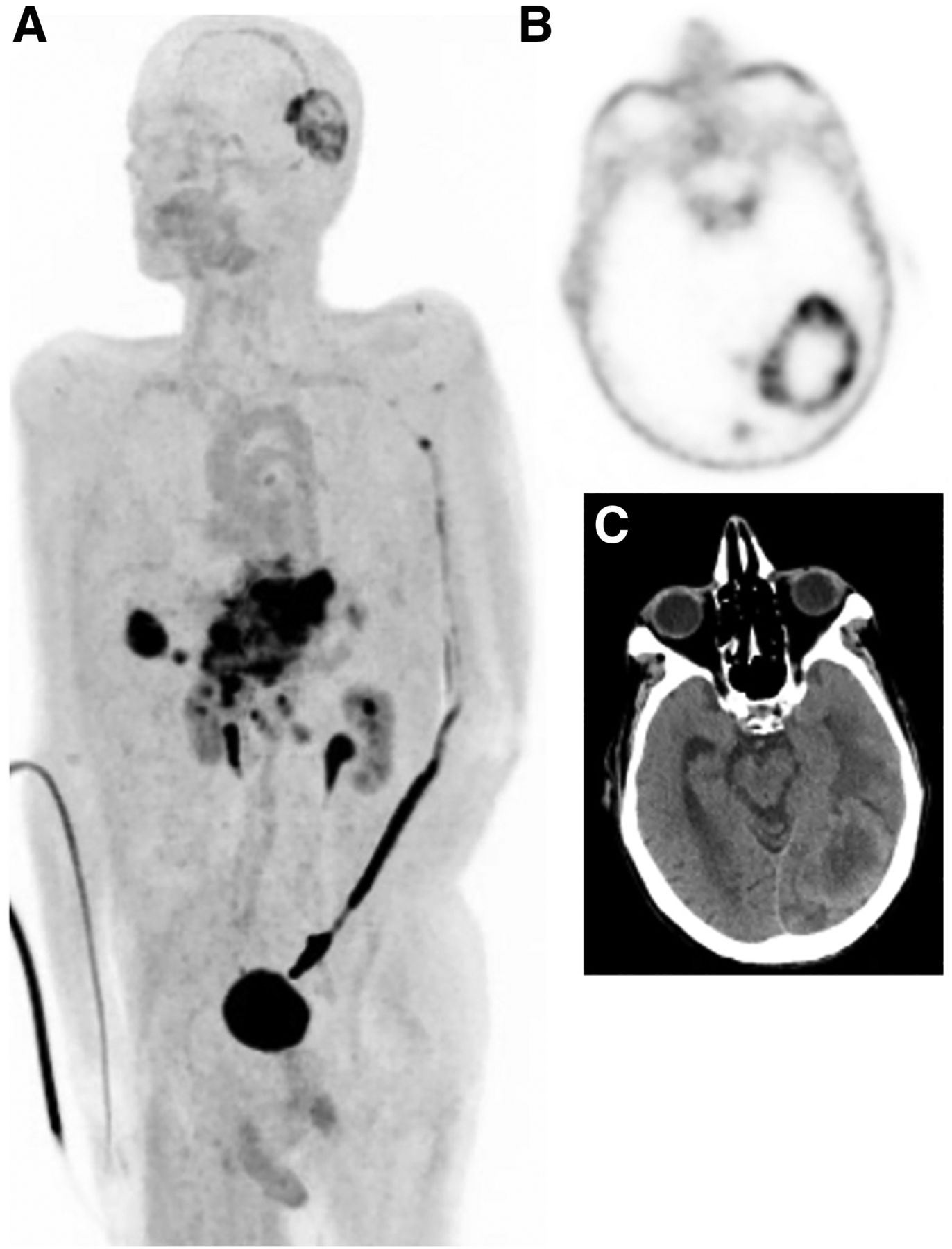
Gastric cancer with node, liver, and brain metastases. (A) FAPI PET maximum-intensity projection. (B) Necrotic left occipital metastasis on transaxial FAPI PET. (C) Correlative CT.
Beside the diagnostic utility of FAPI agents, the potential ability to select patients for radionuclide therapy is an attractive prospect. Preclinical studies of 177Lu-labeled internalizing antibodies directed against FAP have been tested in preclinical models and demonstrated to have efficacy (70). For agents with very high uptake but a short biologic half-life, a radionuclide with a short physical half-life may be more appropriate than a long-lived radionuclide. With these factors in mind, FAPI analogs were evaluated preclinically using 64Cu (71). The pairing of 64Cu and 67Cu represents an exciting theranostic combination. 64Cu is a positron-emitting radioisotope with a 12.7-h half-life, allowing centralized manufacturing and distribution of diagnostic tracers as well as the ability to perform prospective dosimetry (72), whereas 67Cu is a β-emitting radiometal with physical characteristics similar to 177Lu but a shorter half-life. Compared with 68Ga-FAPI-04, 64Cu-FAPI-04 showed higher liver and intestinal activity. Although it is known that the radiometal component of otherwise identical targeting agents can alter biodistribution (73), for copper, there is a possibility that relatively poor chelation by DOTA may increase free-64Cu uptake in the liver. For radiopeptides, alternative chelating agents can significantly reduce liver activity (74). However, unless related to free copper, altering clearance from rapid renal clearance to slower hepatobiliary excretion may benefit therapeutic applications by increasing the bioavailability of the radioligand.
THERAPEUTIC TARGETING OF FAP IN CANCER
One of the first attempts to leverage high FAP expression as a therapeutic target was a trial in 26 patients, primarily with metastatic colorectal cancer, using an antibody called sibrotuzumab (75). Unfortunately, no objective responses were observed. Further antibodies developed against FAP identified by phage display have been labeled with 177Lu and tested in preclinical models (70). These agents demonstrated encouraging efficacy. Other approaches have included development of FAP-targeting prodrugs, vaccines, and nanoparticles (76), although these have largely been limited to preclinical evaluation as yet.
The therapeutic application of FAPI agents has thus far been relatively limited. The original FAPI-04 report included a single patient treated with 2.9 GBq of 90Y-FAPI-04 for metastatic breast cancer (54). Bremsstrahlung imaging after treatment demonstrated significant tumor retention, and the patient experienced a symptomatic improvement in bone pain, thereby demonstrating the theranostic potential of these agents.
FAP IMAGING IN OTHER PATHOLOGIES
There is a wide range of conditions that involve deposition of collagen. In normal-tissue homeostasis, wound healing is the obvious example (77,78). However, an excessive fibrotic reaction characterizes many pathologic states, including keloid formation in the skin, pulmonary fibrosis, asbestosis in the lungs, postmyocardial healing, restrictive pericarditis in the heart, interstitial nephritis in the kidney, and sclerosing cholangitis and cirrhosis in the liver, to name but a few. Additionally, increased FAP expression has be reported in synoviocytes in refractory rheumatoid arthritis (79). In preclinical models, an antibody targeting FAP, 111In-28H1, had impressive uptake but the 89Zn version for PET was less impressive because of higher bone uptake (80).
Benign processes characterized by fibrosis can, of course, coexist with cancer or be caused by cancer treatments, particularly radiotherapy and bleomycin chemotherapy. For example, radiotherapy can induce radiation pneumonitis that can be identified by a geographic increase in uptake of 18F-FDG (81), which often precedes the visualization of abnormality on CT (82). In a preclinical model of bleomycin lung injury, FAP levels were increased and fibrosis correspondingly reduced by use of a FAPI (83). Nonmalignant fibrosis of the mesentery and cardiac valves is a characteristic feature of carcinoid syndrome. Serotonin and bradykinins secreted by enterochromaffinlike cells have been implicated in this process through stimulating fibroblasts (84). In the heart, transforming growth factor β, which is also a key cytokine in cancer-associated desmoplasia, has been shown to be involved in the development of cardiac valvular thickening that characterizes carcinoid heart disease (85). Under the influence of transforming growth factor β, FAP is also instrumental in remodeling in the periinfarct zone after ischemic injury to the myocardium (86,87). The potential for FAPI PET to image this process has been demonstrated clinically (88,89).
Thus far, only limited clinical studies have been performed in benign fibrotic conditions using newer FAPI agents. Diffusely increased uptake in a cirrhotic liver but not in associated nodules, one of which was a hepatic adenoma on biopsy, has been reported (90). High uptake in hepatic cirrhosis could potentially impair the detection of hepatocellular carcinoma arising in this setting. However, in a recent series of 17 patients, who included 11 patients with intrahepatic hepatocellular carcinoma, all 15 identified lesions were positive on FAPI-04 PET/CT despite the fact that the liver-parenchyma SUVmean was significantly higher in patients with cirrhosis than in patients without cirrhosis (91).
IgG4-related disease seems to have high FAPI avidity, which may be focal or diffuse in the pancreas and involve other organs, particularly the lungs, salivary glands, and biliary tract (57,92,93). In the largest series published as yet, 26 patients were evaluated with both 18F-FDG and FAPI-04, with the latter demonstrating active disease in all cases and additional sites of involvement in 50% of cases (93). Activation of myofibroblasts by polarized CD4-positive T lymphocytes is the likely explanation for this finding (94). Large-vessel vasculitis is another potential application because of the rapid blood clearance and high uptake in vasculitis lesions (Fig. 5). The ability to differentiate vasculitis from active atherosclerotic plaques may, however, be limited, with an autoradiographic using an 125I-labeled FAPI agent demonstrating high binding to plaques in an animal model (95).

Giant cell arteritis. (A) FAPI PET maximum-intensity projection. (B) Coronal slice through aortic arch and subclavian arteries. (C) Sagittal slice through thoracic aorta.
FUTURE DIRECTIONS
There are a large number of ongoing or planned clinical trials using various FAPI tracers suitable for PET imaging, primarily in cancer (96). The need for agents suitable for use in parts of the world where PET is not routinely available is potentially addressed by the development of FAPI agents labeled with 99mTc (97). 99mTc-FAPI-34 has been tested in preclinical models and evaluated in one patient with ovarian cancer and another with pancreatic cancer, with the biodistribution in each case being similar to that for prior 68Ga-FAPI PET/CT and also posttreatment 90Y-FAPI bremsstrahlung imaging. A further attraction of this agent is the potential for therapeutic use with 188Re. This generator-produced β-emitting radionuclide has a relatively short half-life (16.9 h), which may be advantageous given the clearance kinetics of FAPI-34, and an imageable γ-emission (155 keV), allowing posttreatment dosimetry (98).
CONCLUSION
Although preliminary, there are several reasons to be hopeful that FAPI agents will play an important role in the molecular imaging armamentarium. These include high expression across a wide range of cancer types (including several with typically low 18F-FDG avidity), low uptake in almost all normal tissues (including the brain and bowel, where high physiologic uptake can obscure primary or metastatic disease), and the ability to provide prognostic information that might guide therapeutic options. Although it remains unclear whether targeting FAP will be an effective therapeutic strategy, the possibility of theranostics remains intriguing. As with 18F-FDG, the causes of false-positive cancer diagnoses open possibilities for a broader use of these agents, particularly in a range of fibrotic diseases that are difficult to monitor noninvasively.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 4, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- Received for publication October 12, 2020.
- Accepted for publication November 12, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}