


Abstract
This study evaluated a novel high-resolution breast-specific gamma camera (HRBGC) for the detection of suggestive breast lesions. Methods: Fifty patients (with 58 breast lesions) for whom a scintimammogram was clinically indicated were prospectively evaluated with a general-purpose gamma camera and a novel HRBGC prototype. The results of conventional and high-resolution nuclear studies were prospectively classified as negative (normal or benign) or positive (suggestive or malignant) by 2 radiologists who were unaware of the mammographic and histologic results. All of the included lesions were confirmed by pathology. Results: There were 30 benign and 28 malignant lesions. The sensitivity for detection of breast cancer was 64.3% (18/28) with the conventional camera and 78.6% (22/28) with the HRBGC. The specificity with both systems was 93.3% (28/30). For the 18 nonpalpable lesions, sensitivity was 55.5% (10/18) and 72.2% (13/18) with the general-purpose camera and the HRBGC, respectively. For lesions ≤ 1 cm, 7 of 15 were detected with the general-purpose camera and 10 of 15 with the HRBGC. Four lesions (median size, 8.5 mm) were detected only with the HRBGC and were missed by the conventional camera. Conclusion: Evaluation of indeterminate breast lesions with an HRBGC results in improved sensitivity for the detection of cancer, with greater improvement shown for nonpalpable and ≤1-cm lesions.
Mammography is currently the most widely used imaging method for breast cancer screening. The sensitivity of screening mammography for breast cancer detection is 85% (1). In radiodense breasts, the sensitivity of mammography decreases to 68% (1). In addition, only 15%–30% of breast biopsies yield a diagnosis of malignancy. Therefore, adjunct methods are needed to improve breast cancer detection and differentiation of benign from malignant lesions.
Recent studies of 99mTc-sestamibi scintimammography showed sensitivities ranging from 62% to 95.8% and promising specificities ranging from 69% to 100% (2–14). Although the presence of radiodense fibroglandular breast tissue does not decrease the sensitivity of scintimammography, the sensitivity is decreased for ≤1-cm lesions, especially those in the medial aspect of the breast (15–18). The sensitivity for detection of lesions ≤ 1 cm ranges from 35% to 64% with general-purpose gamma cameras (7,13,15–19). The design of a general-purpose gamma camera does not allow for optimal breast imaging and prohibits the acquisition of standard mammographic views that would allow better spatial registration between the modalities. It was for these reasons that we developed a high-resolution, small-field-of-view gamma camera to improve the resolution of scintimammography and optimize positioning for breast imaging (20).
The development of a high-resolution, small-field-of-view breast-specific gamma camera can improve the sensitivity of nuclear medicine imaging of the breast in several ways. Such a camera can increase intrinsic spatial resolution and accessibility to the posterior and medial areas of the breast, decrease the impact of scatter radiation from nearby organs (such as the myocardium and the liver) on imaging, minimize the distance between the breast and the detector to improve resolution, decrease the amount of breast tissue between the lesion and the detector through mild compression, and image using patient positions comparable to those of mammography. We report our preliminary results for a prototype high-resolution breast-specific gamma camera.
MATERIALS AND METHODS
Patients and Study Design
All nonpregnant patients who were 18 y or older and for whom additional evaluation with 99mTc-sestamibi scintimammography was recommended for clinical indications were prospectively evaluated with a conventional gamma camera and a novel high-resolution breast-specific gamma camera prototype. Clinical indications for scintimammography included a palpable lesion with no mammographic correlate; possible multicentricity shown on mammography or sonography; asymmetric breast tissue shown on mammography, with no corresponding sonographic or clinical findings; and patient anxiety. The Institutional Review Board approved the study, and all patients gave informed consent. A standard 925-MBq dose of 99mTc-sestamibi was administered into a pedal vein. All suggestive breast lesions underwent biopsy, and the results were proven pathologically. Patient age, lesion palpability, lesion size, time from scintimammography to biopsy, and biopsy type were documented.
Mammography
Craniocaudal and mediolateral oblique mammograms were obtained on dedicated film-screen mammography equipment (Siemens Medical Systems, Iselin, NJ, and MIV; Lorad, Danbury, CT) using 90-s processing (Kodak, Rochester, NY). Additional views (coned compression or magnification views) were obtained as deemed necessary by the radiologist. All patients with a palpable finding were examined sonographically using a 7.5-, 10-, or 13.5-MHz linear-array transducer (Elegra; Siemens, Issaquah, WA, and Acoustic Imaging, Mountain View, CA). Breast density, lesion type, and size were recorded. Lesions were characterized as microcalcifications or masses, with the latter including asymmetric densities and architectural distortion.
Conventional Scintimammography
Lateral and anterior nuclear images were obtained with the patient prone, using a conventional gamma camera with a high-resolution or ultra-high-resolution collimator, as previously described (2). Patients received an intravenous injection of 925 MBq 99mTc-sestamibi (Miraluma; DuPont Pharma, Billerica, MA) injected into the pedal vein. Planar images were obtained for 10 min per image, beginning 5–10 min after radiotracer administration. Images of each breast were obtained with the patient in the lateral prone position, lying on a table overlay designed for breast imaging; a single anterior view with the patient supine followed.
Prototype High-Resolution Breast-Specific Gamma Camera
After completion of the scintimammographic study with the general-purpose gamma camera and approximately 1–1.5 h after injection, the patients were imaged in a seated position with a high-resolution breast-specific gamma camera (technology developed and licensed to Dilon Technologies, Inc., Newport News, VA, by Thomas Jefferson National Accelerator Facility, Newport News, VA). Craniocaudal and mediolateral views of the breast of interest were obtained, at 10 min per view (Fig. 1).
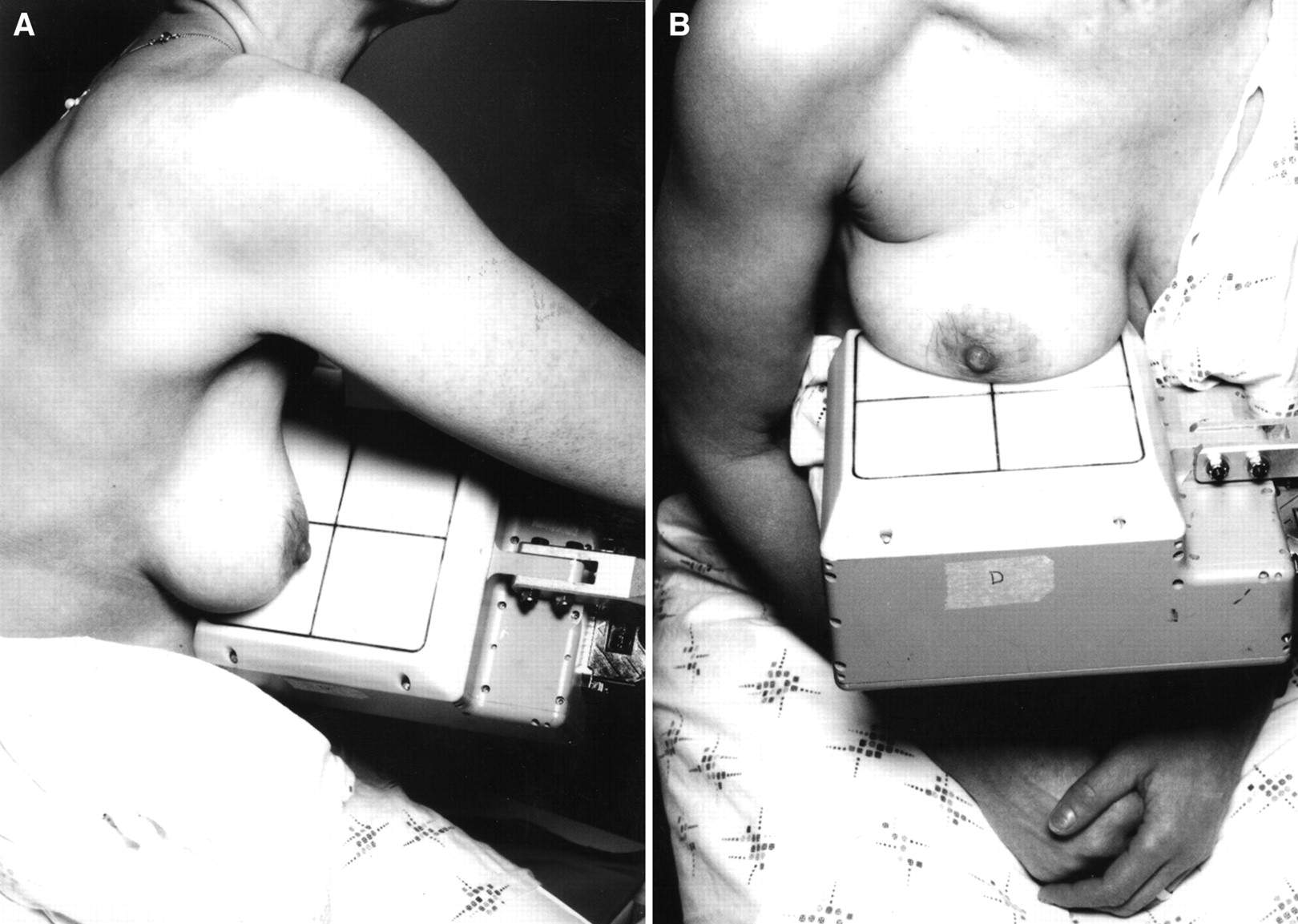
Imaging using high-resolution breast-specific gamma camera in mediolateral projection (A), comparable with projection obtained with mammography, and craniocaudal projection (B).
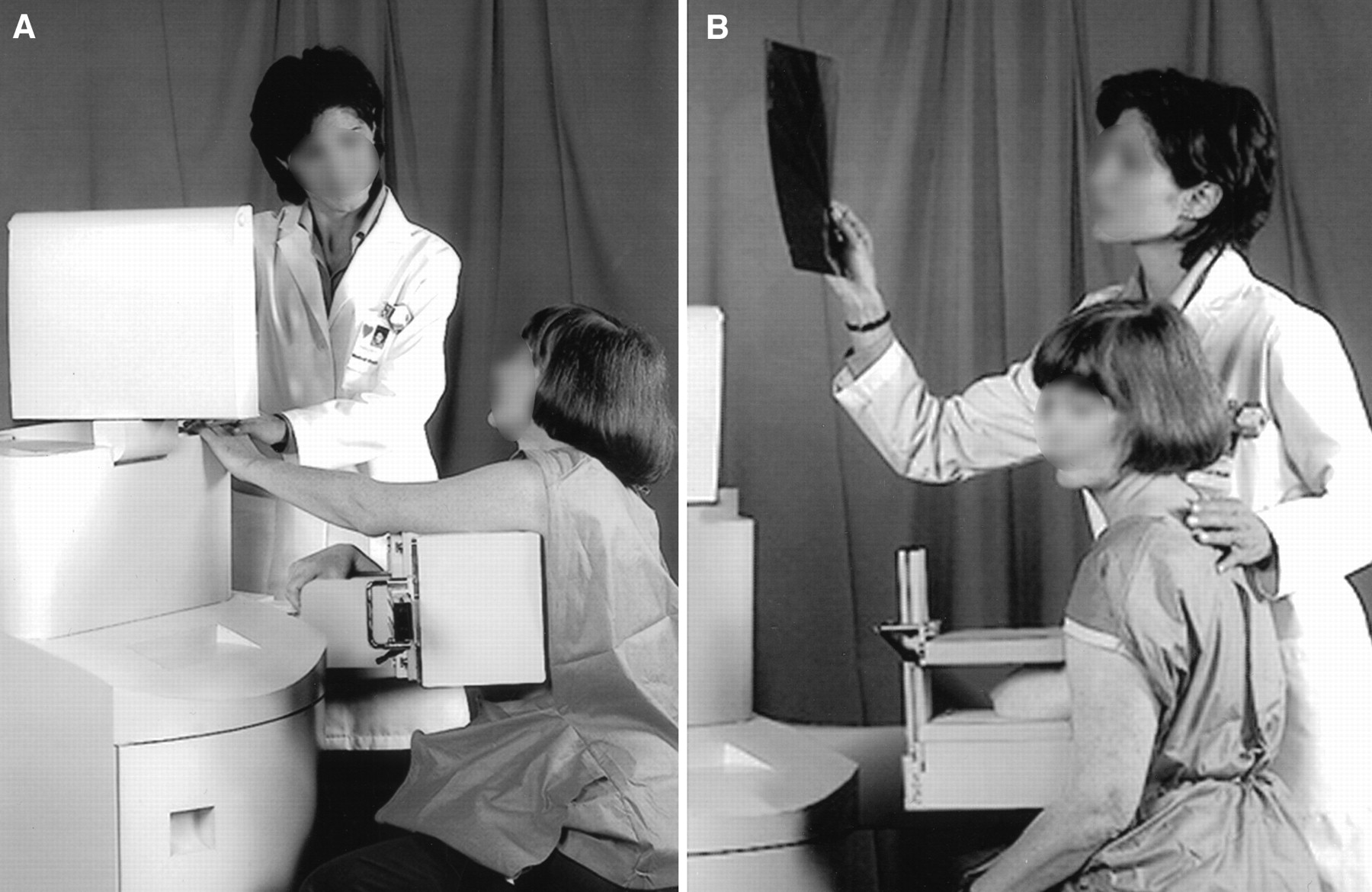
The high-resolution, breast-specific gamma camera differs from general-purpose gamma cameras in the following ways. An array of 3 × 3 × 10 mm NaI (Tl) crystals separated by a 0.3-mm-wide reflective septum is used in place of the single crystal typical of conventional, general-purpose gamma cameras. This pixel-based scintillator does not suffer from the edge effects of the single-crystal systems and therefore allows the entire field of view to be useful. The sensitive area of the detector begins <10 mm from the outside edge of the detector housing. An assembly of square position-sensitive photomultiplier tubes is optically coupled to the crystal array. The breast can be imaged in the craniocaudal and medial lateral views (Fig. 1) while in contact with the detector head and under mild compression, resulting in greater lesion contrast and resolution. Mild compression is provided by a graded shielding plate termed the γ-isolation shield (Fig. 2). Although this device was developed to reduce image contamination from extramammary radiotracer uptake, we found the application of mild compression decreased patient motion and improved lesion contrast. The gantry design of the high-resolution breast-specific gamma camera uses an articulating arm for support of the detector head and the γ-isolation shield. A further technical description is beyond the scope of this article, but details and performance characteristics have been published, and the comparative resolution of the general-purpose and high-resolution gamma cameras is shown in Figure 3 (20). In addition, several technical reports have been published on other independently developed high-resolution gamma cameras (21–25).

Imaging using γ-isolation shield in craniocaudal (A) and mediolateral oblique (B) projections to reduce image contamination from extramammary radiotracer uptake and to apply mild compression.
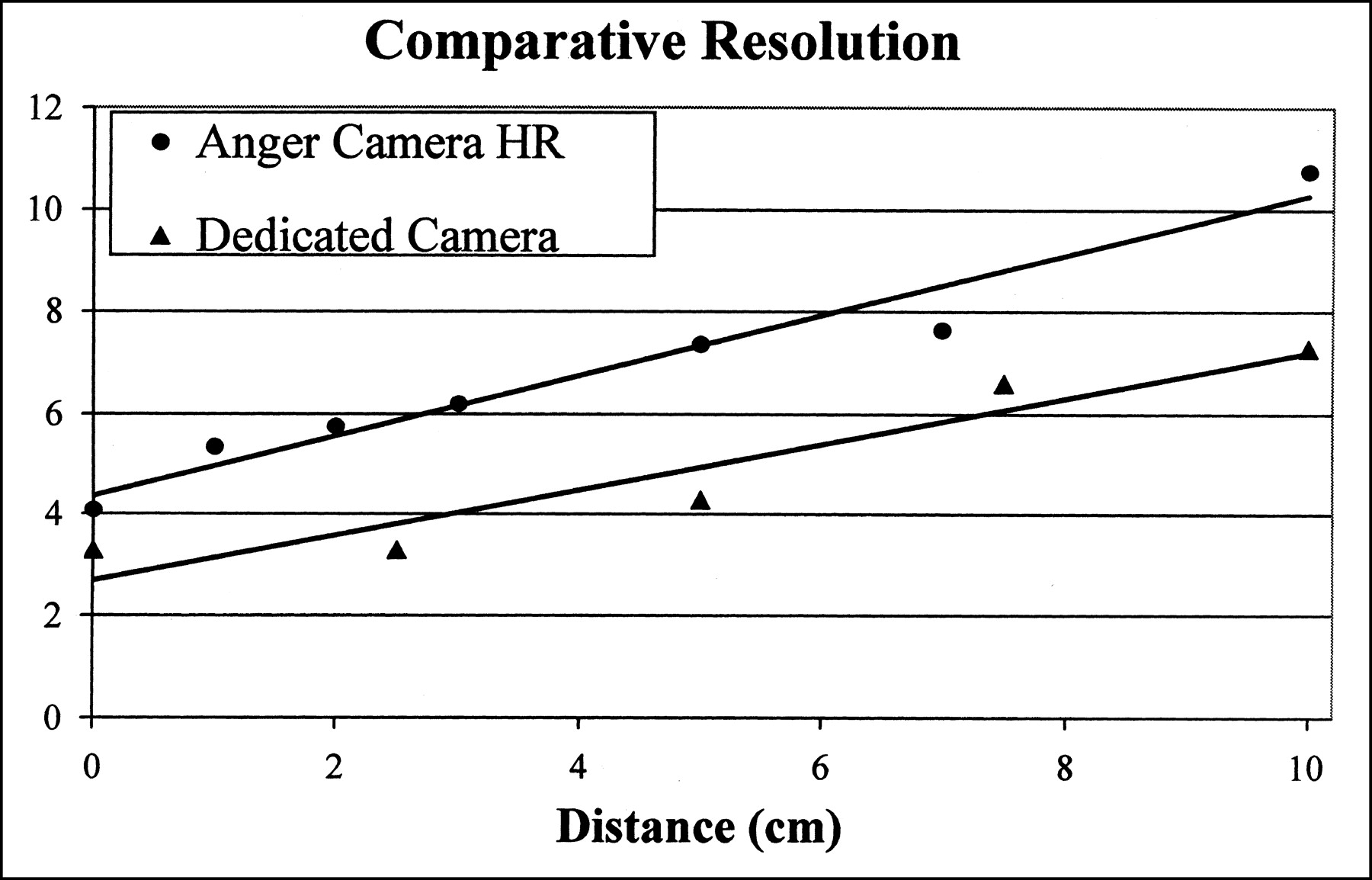
Comparative resolution of traditional gamma camera using high-resolution (HR), high-efficiency collimators and breast-specific gamma camera. y-axis = resolution (mm).
Data Analysis
The results of conventional and high-resolution nuclear studies were prospectively classified as negative (normal: no uptake; benign: mild ill-defined area of radiotracer uptake, probably physiologic) or positive (suggestive: focal mildly increased radiotracer uptake; malignant: focal highly increased radiotracer uptake) by 2 radiologists who were unaware of the mammographic and pathologic results. Any discrepancies in interpretation were resolved by consensus. The quality of images obtained with the high-resolution breast-specific gamma camera was graded according to a 3-point scale (0 = uninterpretable; 1 = good; 2 = excellent). Grade 0 images from the high-resolution breast-specific gamma camera were excluded from this study because they were uninterpretable. Paired statistical analysis of the sensitivity of both conventional gamma cameras and high-resolution breast-specific gamma cameras for the detection of breast carcinoma was performed using the McNemar test.
RESULTS
The high-resolution breast-specific gamma camera images of 5 patients were excluded because of poor quality (grade 0). All of these images were obtained during the initial part of the study and during camera modifications. Image quality improved during the course of the study as clinical and instrumental improvements were made.
Fifty patients (58 lesions) were included (age range, 30–80 y; mean age, 53 y). Of the 58 lesions, 41 (71%) were not palpable and 17 (29%) were palpable. Lesion size at mammography or sonography ranged from 3 to 60 mm (median size, 11 mm; mean size, 14 mm). The mean time between the scintimammographic examination and subsequent biopsy was 5.7 d, and the range was 0–56 d. Four lesions underwent surgical biopsy, and 54 underwent percutaneous biopsy with either sonographic guidance (n = 20) using a 14-gauge spring-loaded needle (Achieve; Allegiance Health Care Corp., McGraw Park, IL) or stereotactic guidance (n = 34) using an 8-gauge vacuum-assisted biopsy needle (MIBB; United States Surgical/Tyco Corp., Danbury, CT). All malignant lesions were subsequently excised surgically.
Of the 58 lesions, 30 (52%) were benign and 28 (48%) were malignant. Benign lesions ranged in size from 3 to 40 mm (median size, 11.5 mm; mean size, 13.4 mm) as determined mammographically or sonographically and included benign breast tissue (n = 9), fibrocystic changes (n = 8), fibrosis (n = 6), fibroadenomas (n = 2), intraductal papillomas (n = 2), mastitis (n = 2), and fat necrosis (n = 1). Malignant lesions, ranging in size from 4 to 60 mm (median size, 9.5 mm; mean size, 14 mm), as determined by mammography or sonography, included ductal carcinoma in situ (n = 5), invasive ductal carcinoma (n = 12), invasive lobular carcinoma (n = 5), invasive mammary carcinoma (i.e., with ductal and lobular features) (n = 5), and invasive tubular carcinoma (n = 1). Pathologically, lesions ranged in size from 3 to 60 mm (median size, 10 mm; mean size, 14.7 mm). Ten (36%) of 28 lesions were palpable.
Mammography and Sonography
Thirty-one masses and 19 microcalcifications, which ranged in size from 3 to 60 mm (median size, 12 mm), were detected with mammography. Of these, 35 were prospectively classified as suggestive (Breast Imaging Reporting and Data System [BI-RADS] 4) and 15 were prospectively classified as highly suggestive (BI-RADS 5).
Eight masses (14%) (median sonographic size, 8 mm; size range, 5–13 mm) were not detected with mammography. These lesions were clinically (n = 2) or sonographically (n = 6) detected in women with heterogeneously (n = 1) or moderately (n = 6) dense breasts and in 1 woman with scattered dense breast tissue. Four (50%) of the lesions not visible with mammography were found to be malignant at percutaneous biopsy (1 ductal carcinoma in situ and 3 cases of invasive carcinoma). The sensitivity of mammography for breast cancer detection was 85.7% (24/28).
Scintimammography
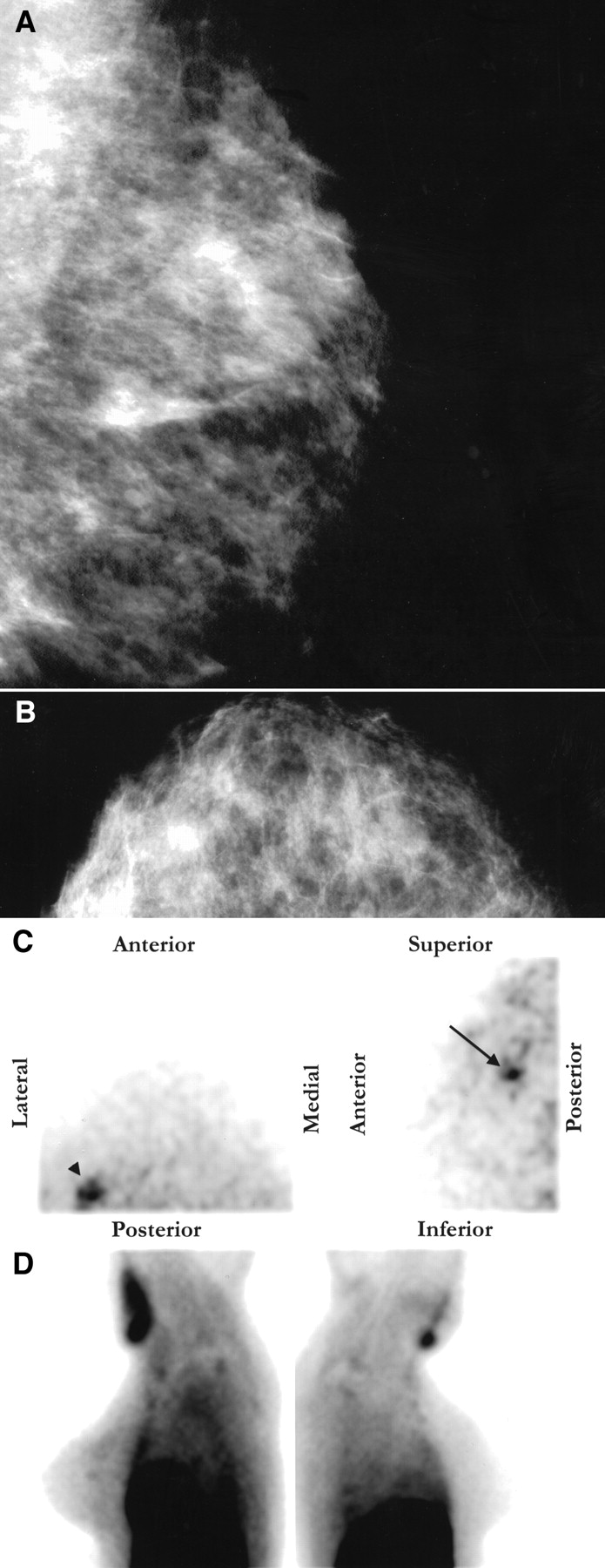
Eighteen (64.3%) of the 28 malignant lesions were detected with the general-purpose gamma camera. Twenty-two (78.6%) of the 28 malignant lesions were detected with the high-resolution breast-specific gamma camera (Table 1). The high-resolution breast-specific gamma camera detected 4 lesions (1 was ductal carcinoma in situ, and 3 were invasive carcinoma) that were not detected with the general-purpose gamma camera (1 palpable and 3 nonpalpable) (Table 2). Of the 4 lesions (3, 8, 9, and 12 mm) detected only with the high-resolution breast-specific gamma camera, 1 consisted of clustered microcalcifications and 3 were masses; 2 were in the medial aspect of the breast and 2 were in the upper outer quadrant of the breast (Fig. 4).
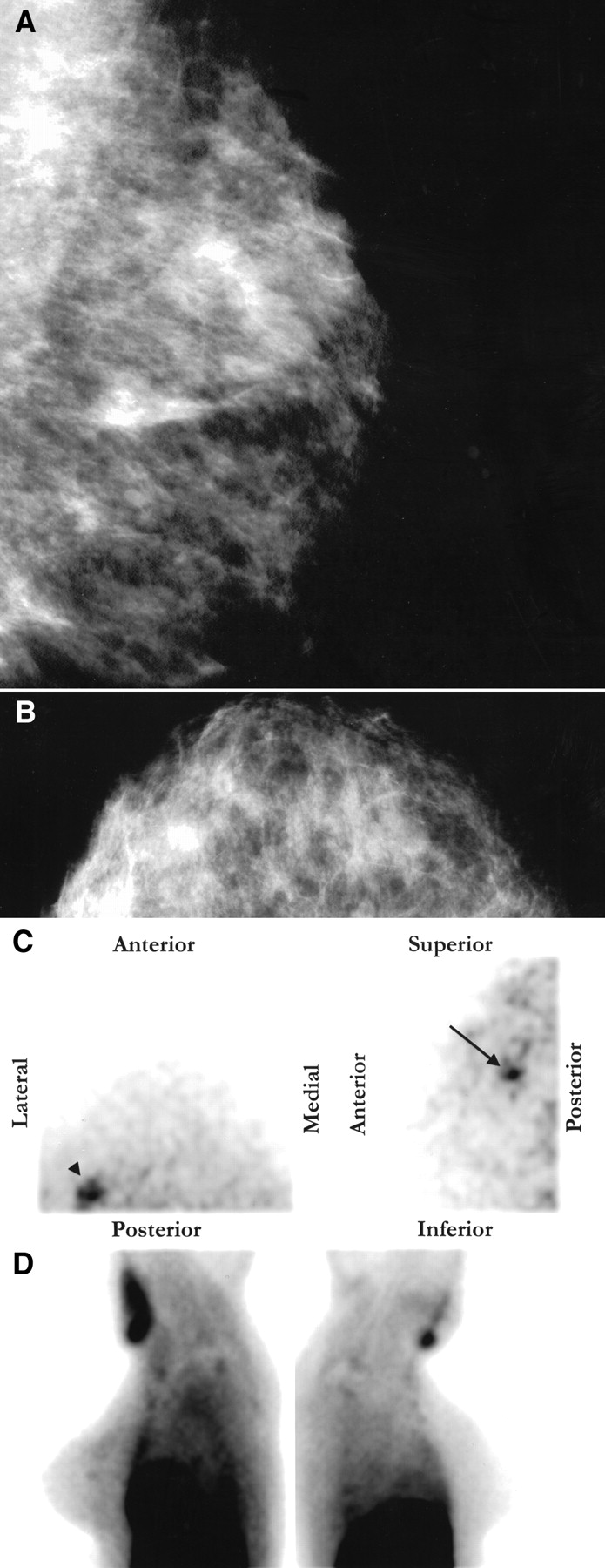
Detection of unsuspected cancer with high-resolution breast-specific gamma camera in 33-y-old woman 2 y after lumpectomy and radiation therapy for infiltrating ductal carcinoma of right breast. Area of architectural distortion appeared in right breast, for which scintimammography was performed. Mediolateral oblique (A) and craniocaudal (B) mammograms of left breast showed normal findings. Scintimammogram with high-resolution breast-specific gamma camera showed normal findings in right breast. However, images of left breast (C) showed focal area of radiotracer uptake in upper (arrow) outer (arrowhead) quadrant of left breast. (D) Images with conventional gamma camera showed possible minimal radiotracer uptake in superior left breast. Biopsy showed 4-mm infiltrating ductal carcinoma.
Comparison of General-Purpose Gamma Camera and High-Resolution, Breast-Specific Gamma Camera: Number of Lesions Detected
Comparison of General-Purpose Gamma Camera and High-Resolution, Breast-Specific Gamma Camera: Sensitivity in Detecting Lesions of Various Sizes and Palpabilities
Six lesions (3 masses and 3 microcalcifications), ranging in size from 3 to 12 mm (median, 6.5 mm; mean, 7 mm), were not detected by either camera. Of these, a 12-mm invasive mammary carcinoma was palpable, and the other 5 were not.
The high-resolution breast-specific gamma camera detected 3 lesions (5–9 mm; median, 8 mm) that were not visible with mammography; the general-purpose gamma camera detected 2. All 3 of these lesions were in areas of dense breast tissue. The lesion that was visible only with the high-resolution breast-specific gamma camera, not with mammography, was a 5-mm, nonpalpable invasive ductal carcinoma, which was detected sonographically.
A patient with mastitis had positive scintimammography findings with both the general-purpose gamma camera and the high-resolution breast-specific gamma camera. In addition, a patient with florid benign duct hyperplasia had positive findings with the general-purpose gamma camera, and a patient with fibrocystic changes had positive findings with the high-resolution breast-specific gamma camera.
In this series, the overall sensitivity of scintimammography for the detection of breast cancer improved from 64.3% (18/28) to 78.6% (22/28) with use of the high-resolution breast-specific gamma camera, as opposed to the general-purpose gamma camera, without a change in specificity (93.3% [28/30]) (Table 2).
The overall sensitivity of scintimammography with the conventional and high-resolution breast-specific gamma camera was compared with the McNemar test (proportions on paired samples), which showed a probability value of 0.12. The sensitivity of breast cancer detection with the general-purpose gamma camera and the high-resolution breast-specific gamma camera for ≤1-cm, nonpalpable lesions could not be compared statistically because of the small sample size in this pilot study.
DISCUSSION
The recent introduction of nuclear medicine imaging of the breast has shown that this physiologic approach to breast cancer imaging offers incremental information and is a useful adjunct in breast cancer diagnosis (2–20). Compared with mammography, scintimammography has been useful in improving the sensitivity of breast cancer detection, especially in women with dense breasts, as well as in improving sensitivity. However, smaller and nonpalpable lesions have not been reliably imaged with conventional, general-purpose gamma cameras because of their intrinsic limitations (7,13,15–19). These include decreased study resolution because of excessive detector-to-organ distance and the inability to image in multiple views, as well as poor spatial registration with mammography. A study has shown that the sensitivity of scintimammography for breast cancer detection in lesions > 1 cm is 97%, compared with <50% in lesions ≤ 1 cm (18). Therefore, a high-resolution, small-field-of-view breast-specific gamma camera was developed to optimize nuclear medicine imaging of the breast.
Using this novel high-resolution breast-specific gamma camera, our study showed an increase in sensitivity for breast cancer detection with scintimammography from 64.3% to 78.6%. In addition, in lesions ≤ 1 cm, the sensitivity for breast cancer detection increased from 46.7% to 66.6%. Statistical evaluation of all lesions included in this study did not show a statistically significant difference in lesion detection. However, additional studies with a larger sample size are needed to more accurately evaluate scintimammography performed with the high-resolution breast-specific gamma camera. Furthermore, lesions ≤ 1 cm and nonpalpable lesions could not be evaluated statistically in this pilot study because of the small sample size. It is on these smaller, nonpalpable lesions that the high-resolution breast-specific gamma camera should have a greater impact. These studies are currently under way.
Imaging with the high-resolution breast-specific gamma camera was always performed after the standard camera series, 1–1.5 h after injection, and therefore outside the optimal imaging time indicated for the radiotracer. Proper dose-to-scan time with the high-resolution breast-specific gamma camera may result in improved diagnostic capabilities.
In this study, the high-resolution breast-specific gamma camera did improve the sensitivity of small-breast-lesion detection to a level comparable with that of all lesions detected with the general-purpose camera. Additional developments and improvements of the high-resolution breast-specific gamma camera are ongoing, and further clinical studies are in progress. In addition, clinical use of the system underwent several advances during the course of this study. Further studies may show improved results from better clinical implementation.
Imaging using patient positions comparable with those used during mammography (craniocaudal and true lateral) is possible with the high-resolution breast-specific gamma camera and should result in improved images of the breast, particularly in the medial portion, where imaging with general-purpose gamma cameras is limited. In addition, the versatility of positioning reduces image contamination from other organs, such as the heart and liver, by limiting the field of view to only the breast. Furthermore, the high-resolution breast-specific gamma camera allows for imaging of seated patients. The seated position has several advantages over the standard prone position used for general-purpose gamma cameras. First, the patient’s arm can be positioned comfortably and need not be extended over the head. Second, the detector can be placed directly against the chest wall, providing better visualization of nearby tissue and allowing a full range of views—craniocaudal, mediolateral, lateromedial, and oblique—without interference from a table (20). Finally, the γ-shield can be placed opposite the detector, and the distance between the detector and the breast lesion can be minimized by mild compression. This mild compression improves lesion contrast and background uniformity by minimizing breast thickness and providing a constant column height of tissue over the collimator. The increased versatility of positioning with the high-resolution breast-specific gamma camera should allow for improved localization of focal areas of radiotracer uptake before needle biopsy, in a manner similar to that of mammography.
The overall sensitivity of breast cancer detection with the general-purpose gamma camera reported in this study was lower than that shown in prior reports evaluating scintimammography (3). However, this study included consecutive patients on whom scintimammography was performed. Therefore, there was no specific patient or lesion size selection. The 1.0-cm mean lesion size included in this study was smaller than the 2.8-cm mean lesion size previously reported (3). We therefore expected that the sensitivity of cancer detection using the general-purpose gamma camera would be lower in our series, which included smaller lesions. The 84.6% (11/13) sensitivity for breast lesions > 1 cm detected with the general-purpose gamma camera shown in our study was comparable with that found for similarly sized lesions in prior scintimammography reports (3).
CONCLUSION
This study showed improved detection of breast cancer, including smaller and nonpalpable lesions, with the high-resolution breast-specific gamma camera. Although statistically significant differences in detection rates were not shown in this limited study, detailed statistical analysis could not be performed because of the small sample size. Nevertheless, these preliminary findings are promising and suggest that the limited ability to image smaller, nonpalpable lesions—an intrinsic limitation of general-purpose gamma cameras—may no longer be an obstacle to incorporation of scintimammography in clinical practice when used as an adjunct to mammography for breast cancer diagnosis.
Acknowledgments
The authors thank Barbara Levit for helping with this study and Joyce Raub, MS, for helping to prepare the manuscript. This study was supported by a grant from Dilon Technologies, Inc., and by DuPont Pharma, Inc. Dr. Brem is a consultant to and has stock options in Dilon Technologies, Inc.
Footnotes
Received Jun. 1, 2001; revision accepted Oct. 22, 2001.
For correspondence or reprints contact: Rachel F. Brem, MD, Breast Imaging and Intervention Center, George Washington University Medical Center, 2150 Pennsylvania Ave., Washington, DC 20037.
E-mail: rbrem{at}mfa.gwu.edu
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Factors Influencing the Uptake of 99mTc-Sestamibi in Breast Tissue on Molecular Breast Imaging
- Update on Emerging Technologies in Breast Imaging
- Breast-specific gamma imaging as an adjunct modality for the diagnosis of invasive breast cancer with correlation to tumour size and grade
- Is There a Clinical Role for Scintimammography in Breast Cancer Diagnosis?
- Scintimammography with Dedicated Breast Camera Detects and Localizes Occult Carcinoma
- Evaluation of a Small Cadmium Zinc Telluride Detector for Scintimammography
- Invited Commentary: One Step Forward