


Abstract
The standard treatment of meningiomas is surgery or radiotherapy. Complex, especially recurrent or progressive cases, may exhibit tumor growth involving critical neurovascular structures or diffuse growth, resulting in limited efficacy and higher risk of standard treatment. We evaluated whether somatostatin receptor–targeted radionuclide therapy with 90Y-DOTATOC may be a therapeutic option. Methods: Fifteen patients with recurrent or progressive meningiomas after multimodal pretreatment or unfavorable medical risk profile were treated with systemic 90Y-DOTATOC. Endpoints were progression-free survival and toxicity. Results: Usually applied doses were 7,400 MBq/m2 of 90Y-DOTATOC in 2 fractions. Mean observation time was 49.7 mo (range, 12–137 mo). Overall median progression-free survival was at least 24 mo. Toxicity was moderate, mostly hematologic (n = 8) and transient. Conclusion: 90Y-DOTATOC therapy is feasible and may represent a promising second- or third-line option for complex meningiomas, which are progressive or otherwise not treatable with a reasonable risk–benefit ratio.
Meningiomas are benign (World Health Organization I [WHO I], 80%–90%), atypical (WHO II, 5%–15%), or malignant neoplasms (WHO III, 1%–3%). Depending on age, tumor size, and treatment, 5-y survival was 70% for benign and 55% for malignant meningiomas (1). A subgroup exhibits a diffuse en plaque growth pattern, and attachment of tumor segments to critical neural or vascular structures obviates complete resection. Attempts to resect meningiomas involving these critical structures may cause devastating vascular injury or disabling cranial neuropathies (2,3). Tumor remnants are treated radiotherapeutically, which leads to 5-y progression-free survival rates in 89% of benign and 48% of malignant cases (4). However, fractionated external-beam radiotherapy may also cause serious neurologic complications (5) and secondary tumors (6). Stereotactic radiotherapy represents an option for selected cases (7), leading to 5-y tumor control rates of 93% (8). Stereotactic GammaKnife (Elekta) radiosurgery led to control rates of 92.5% in small meningiomas, with permanent morbidity rates of 6.6% (9).
Regarding complex or recurrent meningiomas, especially those close to critical vascular respective neural structures or meningiomas with diffuse, meningiosislike growth, there is so far no sufficient therapeutic option.
Seventy to one hundred percent of meningiomas express somatostatin receptors (10), mainly subtype 2a (SSTR2a). Somatostatin analogs have been shown to affect progression-free survival (PFS) in 44% of patients in a 6-mo follow-up in recurrent meningiomas (11).
The aim of this prospective study was to investigate feasibility, toxicity, and efficacy of targeted β radiotherapy for stabilization of complex meningiomas using the somatostatin analog 90Y-DOTATOC, a metabolically stable cyclic octapeptide (12).
MATERIALS AND METHODS
Study Design
This was a clinical phase II single-center open-label study investigating response, survival, and safety. Approval was obtained from the Ethics Committee of Swiss Cantons Basel-Landschaft and Basel-Stadt and Swiss Federal authorities (Swissmedic). We evaluated PFS as a primary endpoint and toxicity as a secondary endpoint.
Patients
Inclusion criteria were SSTR2a positivity, recurrent or progressive meningiomas in functionally critical areas, or unfavorable medical risk profile or refusal of surgery. SSTR2a status was assessed by 111In-DOTATOC scintigraphy/SPECT or 111In-OctreoScan (Mallinckrodt Medical) (112.5 MBq of 111In). Tumor uptake was graded in the following manner (13): lower than (grade 1), equal to (grade 2), or greater than (grade 3) normal liver tissue, or higher than normal spleen/kidney uptake (grade 4). Preexisting grade II–IV hematologic/renal toxicities, also of Karnofsky performance status less than 50, were excluded.
Treatment Protocol
Twenty milligrams of intravenous dexamethasone was administered before therapy. After initial dose modification according to the study of Waldherr et al. (12), the 90Y-DOTATOC dose was fixed at 3,700 MBq/m2 twice, with an 8-wk interval. 111In-DOTATOC (112.5 MBq) was injected simultaneously to verify biodistribution and receptor binding. Imaging was performed 6, 24, and 48 h after injection by γ camera. Dexamethasone was tapered after therapy. Therapeutic effects and adverse events were monitored by clinical examinations, blood sampling, and MR imaging.
Kidney Protection
Renal reuptake and retention were inhibited by the infusion of physiologic saline–containing arginine (20.7 mg/mL) and lysine (20.0 mg/mL).
Radiotracers
The development of DOTATOC, a tetraazocyclo-dodecanetetraacetic acid–modified somatostatin analog (14), followed good manufacturing practices. 111In- and 90Y-DOTA-d-Phe1-Tyr3-octreotide were synthesized according to Waldherr et al. (12). The preparation and affinity and stability calculations of 111In- and 90Y-labeled DOTATOC were according to Merlo et al. (15). The radiolabeling yield determined by a Sep-Pak C18 cartridge (Waters GmbH) and high-performance liquid chromatography was 99% or higher without peptidic radiolysis products, revealing radioligands with preserved receptor binding (the dissociation constant [Kd]) = 2.2 ± 0.5 nM). The affinity of 90Y-labeled DOTATOC was determined by competition assay (1.8 ± 0.5 nM 123In-labeled octreotide), and stability was determined according to Ruser et al. (14).
Toxicity
The scoring of toxicity was according to National Cancer Institute grading criteria (NCI-CTC V4.0). Hematology, liver, and kidney parameters were examined before therapy and biweekly for at least 2 mo after therapy.
Tumor Response
MR imaging was performed 4 wk before and 6–8 wk after treatment. Follow-up of clinical and radiologic examinations was performed at 6- to 12-mo intervals, depending on neurologic status. Response was evaluated according to Response Evaluation Criteria In Solid Tumors 1.1 to determine PFS (i.e., stable disease). Additional treatments were not allowed for at least 12 mo.
RESULTS
Patients
Fifteen patients (median age, 56 y; age range, 41–78 y) were included (Table 1). All patients gave written informed consent. The median Karnofsky performance status at inclusion was 90 (50–100). The sex distribution (female, n = 12; male, n = 3) was as reflected by epidemiologic studies (16). WHO grading was I (n = 9), II (n = 2), and III (n = 1). Biopsy or surgery was not been performed because of a high American Society of Anesthesiologists score in 3 patients; the high diagnostic probability of meningioma was based on typical radiologic patterns in CT/MR imaging and positive 111In-octreotide or 111In-DOTATOC uptake. Fourteen tumors were SSTR2a-positive in 111In-OctreoScan or 111In-DOTATOC; uptake grades were 1 (n = 2), 2 (n = 5), and 3 (n = 7). Overall, 12 patients (80%) were included with progressive tumors, 3 patients (20%) after subtotal resection. Ten patients had been treated by surgery (6 patients), surgery and radiotherapy (3 patients), or surgery and radiotherapy and chemotherapy (1 patient) before 90Y-DOTATOC. These tumors were progressive (patients 1, 3, 4, 6, 7, 8, and 15) or had been subtotally resected (patients 2, 5, and 9). Four patients died from non–tumor-related disease (patients 8, 13, 14, and 15). Mean follow-up was 49.7 mo (range, 12–137 mo).
Patient Characteristics and Treatment
Tumor Response
Stable disease was observed in 13 patients (86.7%) and progressive disease in 2 patients (13.3%). Eight of 15 patients were ongoing stable and did not reach the endpoint PFS. With this statistical limitation, the overall median PFS was at least 24 mo (range, 0–137 mo).
The evaluation of response was limited in 2 patients (patients 13 and 14) because of non–tumor-related death before tumor progression (pneumonia, cardiac failure). Two patients (patients 8 and 15) were radiologically stable for 19 and 14 mo, respectively, but died after 32 and 16 mo (non–tumor-related: pneumonia, hemolytic anemia), respectively.
Five of the 6 remaining patients (83%) with confirmed WHO I tumors (patients 2, 4, 6, 7, and 9) exhibited ongoing PFA (range, 14–137 mo); patient 5 experienced progression after 17 mo.
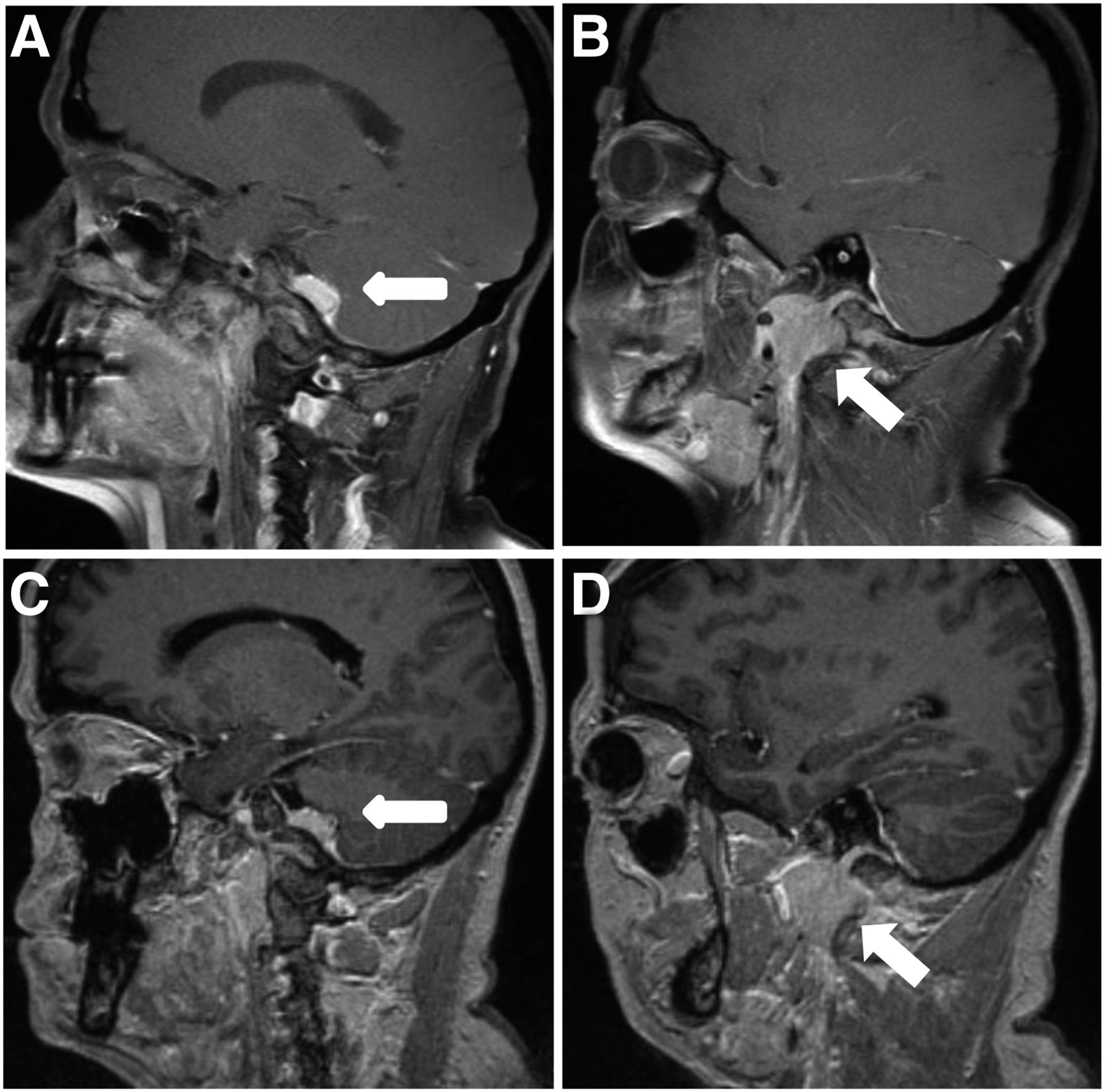
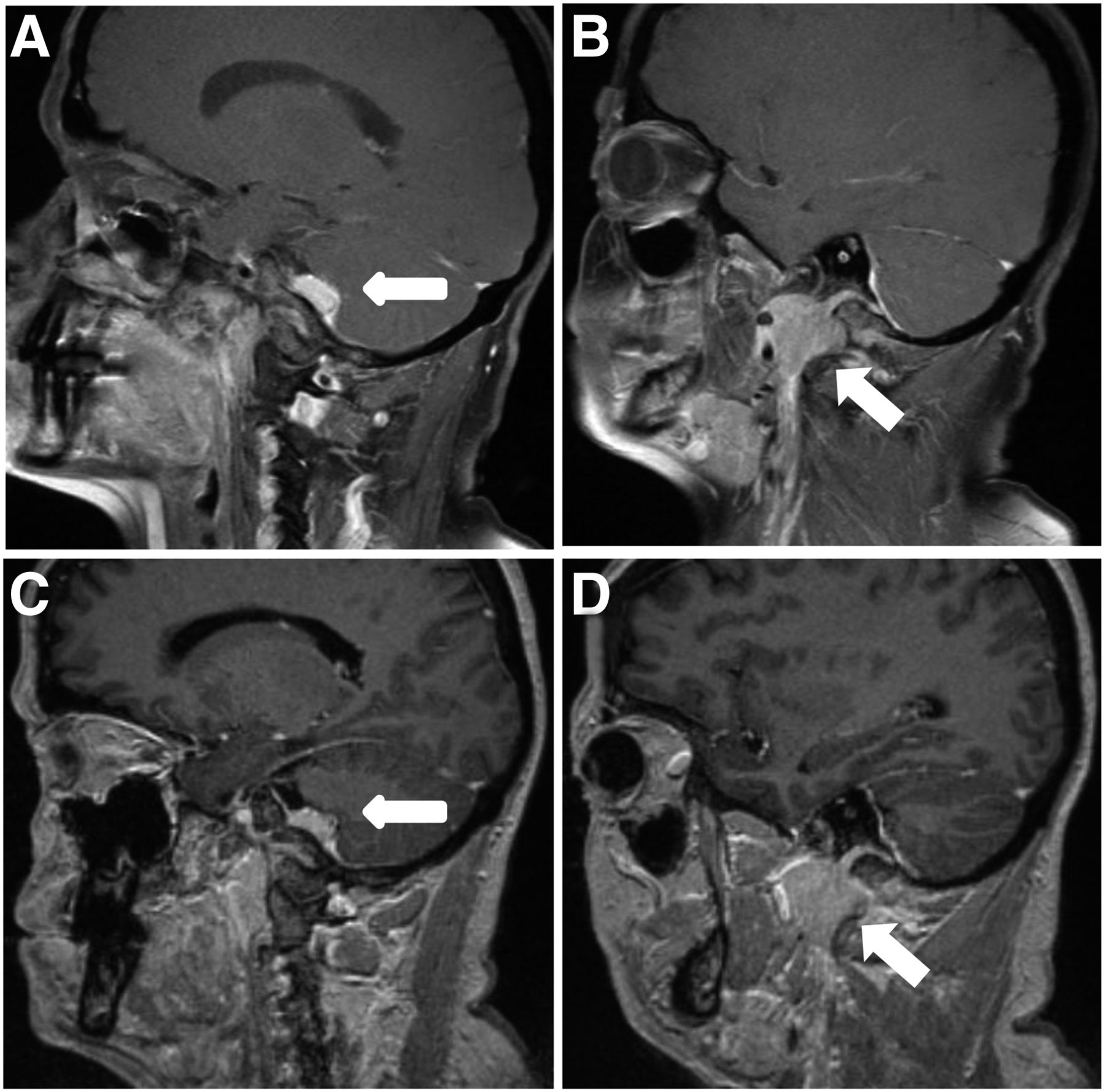
Figure 1 illustrates a progressive skull base meningioma (patient 4) with brain stem compression, infiltration of cavernous sinus, and involvement of the optic chiasm. Surgical decompression was followed by 2 cycles of 90Y-DOTATOC, resulting in ongoing stable disease for now 87 mo.

WHO I meningioma, patient 4. (A) Scintigraphy 24 h after 111In-DOTATOC displaying SSTR2a expression. (B) Contrast T1 MR imaging at initiation of 90Y-DOTATOC therapy. MR imaging 60 mo (C) and 87 mo (D) after 90Y-DOTATOC treatment. Arrow indicates tumor localization.
One WHO II tumor (patient 1) did not respond, whereas the WHO II tumor (patient 10, with craniocervical skull base meningioma) responded to treatment (Fig. 2): after bioptic diagnosis of meningioma WHO II, the patient declined surgery to avoid further risk to the lower cranial nerves. 90Y-DOTATOC (13,320 MBq) led to ongoing clinical stabilization and radiologically stable disease (patient 10, now 83 mo).
WHO II meningioma, patient 10. Meningioma from cerebello-pontine angle to upper cervical spine. (A and B) Contrast T1 MR imaging at initiation of 90Y-DOTATOC therapy: intracranial (A) and vertebral (B) tumor (arrows). (C and D) MR imaging 72 mo after 90Y-DOTATOC treatment. Arrows indicate tumor localization.
Patient 3, with a WHO III meningioma, was radiologically stable for 4 mo after 90Y-DOTATOC therapy (8,438 MBq).
Toxicity
A summary of toxicity is provided in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org). The median follow-up was 6 mo (range, 2–45 mo).
An overall hematologic toxicity greater than grade II was found in 5 patients (33.3%). A reduction of red blood cells from preexisting grade I to III (1 patient, 6.7%) was found, and the patient subsequently recovered. Three (20%) patients had transient thrombocytopenia (grade I), 4 patients (26.6%) transient grade I or II leukopenia, and 8 patients transient lymphocytopenia (4 patients grade II, 26.6%; 4 patients grade III, 26.6%).
Transient neurologic toxicity was found in 2 patients (13.3%): radiogenic edema with gait disturbance (patient 15) and 1 seizure (patient 13).
A creatinine increase to grade II toxicity over 14 mo was found in 1 patient (7.1%) (clearance, 15.8 mL/min).
For 5 patients (33.3%), there was a slight transient elevation of hepatic enzymes, with an unclear relationship to 90Y-DOTATOC due to accompanying morbidity.
DISCUSSION
In most cases, surgical removal of meningiomas is an effective and definitive therapeutic approach. However, meningiomas involving cranial nerves, vascular structures, or the brain stem can render surgery hazardous, with considerable morbidity (3). Consequently, a subgroup of meningiomas was treated by standard external-beam radiotherapy, fractionated stereotactic radiotherapy, or stereotactic radiosurgery. These modalities have been shown to control tumor growth (4), especially in smaller meningiomas (17), but with complications (5,6).
In complex meningiomas involving critical neurovascular structures, exhibiting diffuse growth or recurrence despite multimodal therapy or high perioperative risks, the aims of treatment need to be questioned and should be adapted from complete resection without loss of neurologic function to rather prevention of further tumor growth with preserved quality of life.
With a median PFS of at least 24 mo and ongoing PFS in 83% of confirmed WHO I meningiomas (observation time range, 14–137 mo) in our study, 90Y-DOTATOC may represent a promising option for complex cases. PFS in the WHO I patients in our cohort is somewhat longer than in the study cohort of Bartolomei et al. (18), which may potentially be attributable to higher total doses applied in our study (median dose, 13 vs. 10 GBq). However, the potential dose–effect relationship is interesting, because long-term tumor control can be achieved with relatively low doses by radiosurgery (19,20).
Because of the small number of confirmed WHO II–III patients in our study, it remains unclear whether malignant meningiomas may potentially require higher doses than the applied doses. In the study of Bartolomei et al. (18), this group of patients was treated analogous to WHO I meningiomas with a median dose of 10 GBq. The outcome of the WHO II and III patients was significantly inferior to those patients with WHO I meningiomas, which might indicate the need for higher doses.
With regard to additive toxicity, the potential combination of radiotherapy and radiolabeled somatostatin analogs has raised concerns and has been addressed by Kreissl et al. (21). According to their results, a combination of 177Lu-labeled somatostatin analogs with fractionated external-beam radiotherapy is feasible and well tolerated. Consequently, 90Y-DOTATOC treatment may supplement surgery and the existing radiotherapeutic options with a promising second- or third-line option for patients with otherwise poor alternatives. However, patients with impaired renal function have to be evaluated thoroughly before considering therapy with radiolabeled somatostatin analogs. Alternatively, according to the results of Minutoli et al. (22), 111In-labeled somatostatin analogs might be used instead of β-emitting radionuclides in cases with a higher risk of renal toxicity.
CONCLUSION
This study demonstrates the feasibility and efficacy of 90Y-DOTATOC treatment in patients with complex meningiomas. Hematologic, neurologic, and renal toxicities were transient and moderate. 90Y-DOTATOC may represent a promising second- or third-line therapeutic option for complex meningiomas, which are progressive or otherwise not treatable with reasonable risk–benefit ratio.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by the Swiss National Science Foundation (Tandem 3238-056368.99) and by the Regional Cancer League of Basel. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 20, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 26, 2015.
- Accepted for publication August 10, 2015.





{kind=link}
{kind=link}