


Abstract
A 65-y-old woman with multiple cardiovascular risk factors presented with atypical chest pain, prompting a 1-d pharmacologic stress myocardial perfusion test using 99mTc sestamibi. Initial interpretation suggested ischemia, but closer inspection revealed increased right ventricular uptake and increased left ventricular chamber size at stress, indicative of significant 3-vessel coronary artery disease (CAD). These findings were confirmed by cardiac catheterization, showing 3-vessel disease, including significant left main CAD. The patient underwent coronary artery bypass graft surgery. This case highlights the importance of meticulous SPECT image interpretation, particularly focusing on right ventricular uptake and transient ischemic dilation, to accurately diagnose severe CAD and improve cardiovascular outcomes.
- myocardial perfusion imaging
- right ventricular uptake
- transient ischemic dilation
- SPECT
- coronary artery disease
SPECT myocardial perfusion imaging is an essential tool in the cardiologists’ arsenal for detecting coronary artery disease (CAD). Detailed inspection of images in the context of the patient’s presentation and other findings is crucial for correct interpretation, directly influencing further steps and treatment that aim to improve cardiovascular outcomes.
CASE REPORT
A 65-y-old woman with a past medical history of diabetes complicated by neuropathy, retinopathy and glaucoma, heartburn, hypertension, hyperlipidemia, and asthma presented with nonradiating chest pressure while eating. She denied dyspnea or exercise limitation. The more likely diagnosis was gastroesophageal reflux disorder instead of acute coronary syndrome, given atypical chest pain and a history of heartburn. However, she was admitted for closer observation because of her risk factors. Echocardiography showed a left ventricular (LV) ejection fraction of 60% with no regional abnormalities and moderate aortic stenosis.
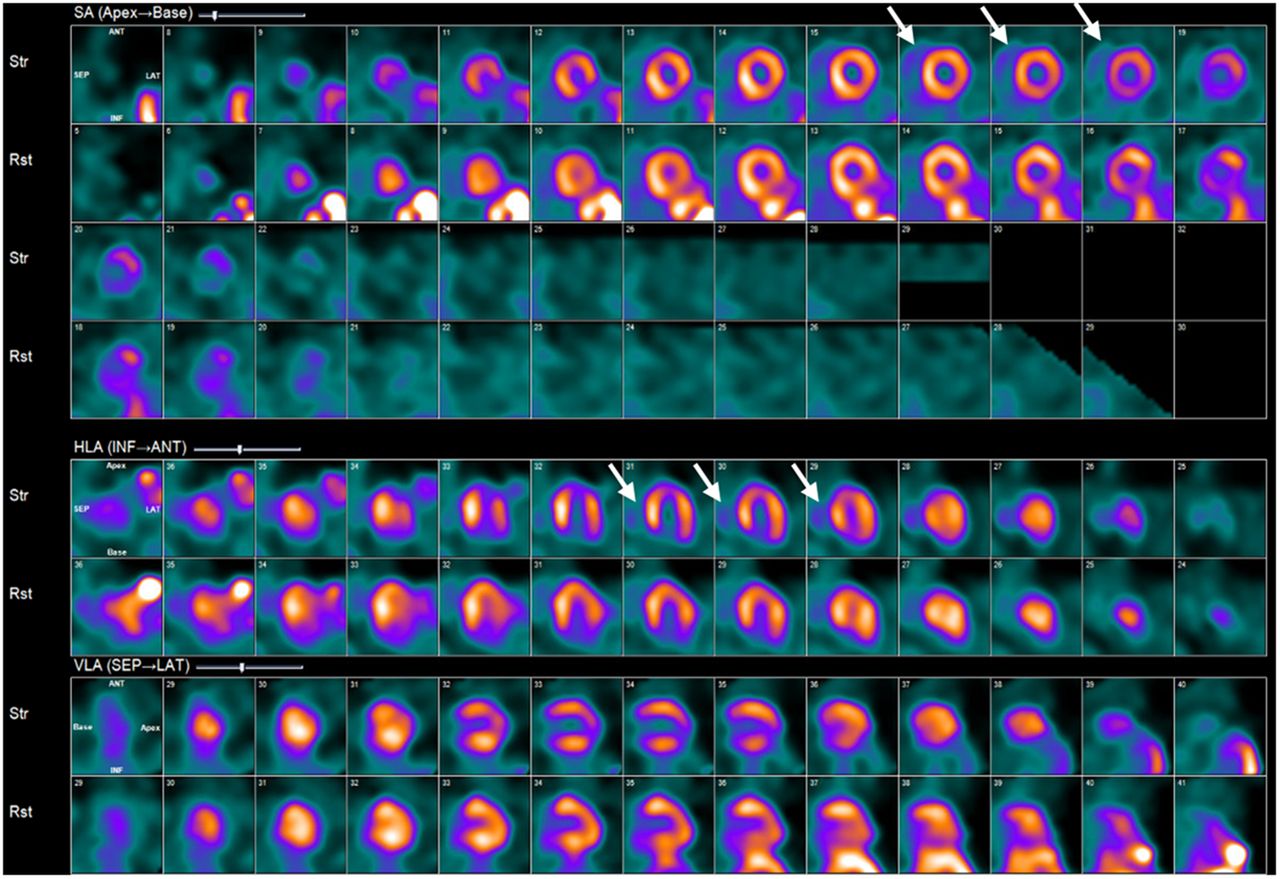
A 1-d pharmacologic stress myocardial perfusion test was performed the following day using 99mTc sestamibi, with the findings shown in Figure 1. Imaging was notable for increased gut uptake and Compton scatter at rest, which was absent at stress. Despite this artifact, additional pertinent findings were noted, including a small, severe stress-induced perfusion abnormality at the apex that completely reversed on the rest images. This finding would otherwise indicate a prognostically low-risk study necessitating intensification of medical therapy for underlying CAD.

Rest and stress regadenoson 99mTc SPECT myocardial perfusion imaging imaging shows increased RV uptake, which is more pronounced at stress (white arrows) than at rest. Images also show transient ischemic dilatation on stress.
However, on closer inspection, one can note several additional important details that would dramatically influence the interpretation and subsequent patient management. On the stress images, the right ventricle (RV) appears prominent with significantly increased tracer uptake, most notably in the short- and horizontal long-axis orientations (Fig. 1). Additionally, although easily overlooked, there was an increase in LV chamber size at stress compared with at rest (transient ischemic dilatation).
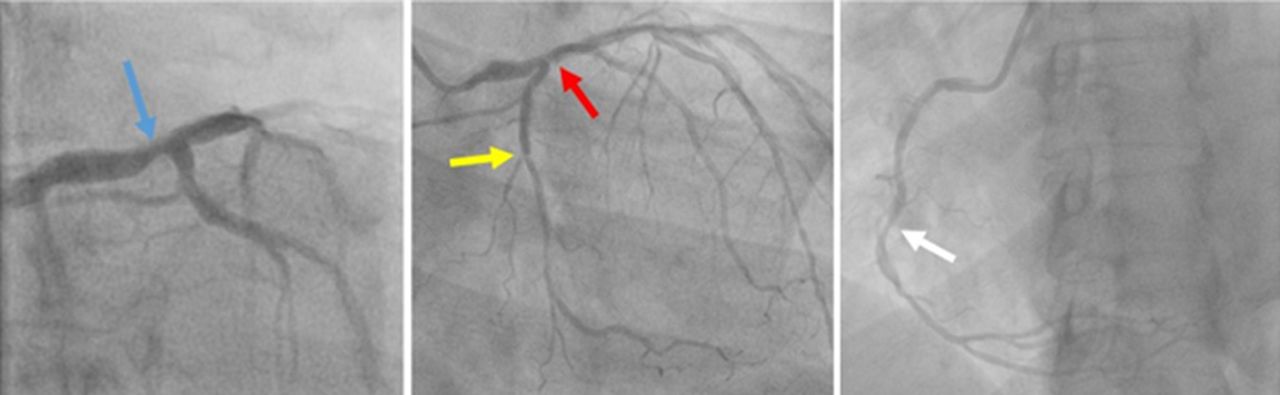
Consequently, left heart cardiac catheterization was performed, and 3-vessel disease, including significant left main CAD, was found (Fig. 2). The patient was referred for coronary artery bypass graft surgery with successful recovery.

Coronary angiogram. Significant multivessel stenosis was identified in left main coronary artery (blue arrow), proximal left anterior descending coronary artery (red arrow), left circumflex coronary artery (yellow arrow), and right coronary artery (white arrow).
DISCUSSION
Increased RV uptake and increased LV chamber size on the stress images, taken together, suggest significant 3-vessel CAD (1–5). RV uptake may indeed be increased in the setting of RV hypertrophy due to increased pressures. A prominent RV contour would typically be noted on the rest and stress images. However, when the RV uptake is more pronounced at stress than at rest, it can indicate significant multivessel disease. This finding occurs because the entire LV myocardium has less radiotracer uptake at stress compared with the unchanged tracer uptake in the RV, which is not ischemic (2–4).
Increased LV chamber size or transient ischemic dilation on myocardial perfusion imaging refers to an apparent enlargement of the LV cavity on poststress images compared with rest images. It is thought to be caused by severe global subendocardial ischemia, making the cavity appear larger on stress images. Transient ischemic dilation is a marker of severe, extensive CAD (1,5).
CONCLUSION
Careful inspection of SPECT myocardial perfusion images is crucial for accurately diagnosing CAD. Special attention must be given to the RV uptake as well as LV chamber size, which, in the appropriate context and patient history, may correctly identify significant 3-vessel CAD. Prompt intervention in these patients with multiple risk factors, including diabetes, may significantly improve mortality and other cardiovascular outcomes, further stressing the value of careful SPECT interpretation (6).
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 22, 2025.
REFERENCES
- Received for publication March 24, 2025.
- Accepted for publication March 31, 2025.
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.