


Abstract
Ventilation and perfusion (V/Q) lung scintigraphy has been used in the assessment of patients with suspected pulmonary embolism for more than 50 y. Advances in imaging technology make SPECT and SPECT/CT feasible. This article will examine the application and technical considerations associated with performing 3-dimensional V/Q SPECT and the contribution of a coacquired CT scan. The literature tends to be mixed and contradictory in terms of appropriate investigation algorithms for pulmonary embolism. V/Q SPECT and SPECT/CT offer significant advantages over planar V/Q, with or without the advantages of Technegas ventilation, and if available should be the preferred option in the evaluation of patients with suspected pulmonary embolism.
Although ventilation and perfusion (V/Q) lung scintigraphy has been used in the assessment of patients with suspected pulmonary embolism for more than 50 y, there have been advances in imaging technology to provide superior resolution and sensitivity, SPECT techniques, and SPECT/CT hybrid imaging. Advances in ventilation agents, Technegas (Cyclomedica) in particular, have contributed to assimilation to SPECT and SPECT/CT protocols. Technegas was developed in Australia in 1984 (1), and Chris McLaren, an Australian pioneer nuclear medicine technologist, was part of the team evaluating its original clinical application. Unlike radioaerosols, Technegas does not redistribute after administration, a requirement for any prolonged tomographic acquisition (such as SPECT). McLaren appears to be the first (in 1987) to recognize the potential not only for performing SPECT V/Q lung scanning but also for computerized subtraction of SPECT data to map and quantify potential perfusion defects (2). His approach highlighted the major issue associated with the fact that both phases use 99mTc in a single-day protocol and provided a solution: “A useful spin-off from the subtraction technique is that ‘true’ perfusion images are obtainable” (2).
This discussion will not examine the broader debate on the role and application of V/Q imaging or the merits of Technegas; these have been detailed widely elsewhere. The discussion will explore the application and technical considerations associated with performing the entire V/Q protocol as 3-dimensional SPECT imaging and the addition of a coacquired CT scan.
This article aims to both challenge and inform readers on the role of SPECT and SPECT/CT. The original perspective for the article focused on the added value of technologic innovation that not only makes planar imaging redundant but also makes SPECT a requisite. Drawing a comparison to the omission of SPECT from the armamentarium of myocardial perfusion, skeletal or cerebral perfusion imaging was thought to highlight the importance of SPECT in lung scanning. Challenging readers to consider the appropriateness of a clinical department that performs planar cerebral perfusion imaging, myocardial perfusion or spine imaging was initially thought analogous to a department performing only planar lung scanning. Although provocative, the challenge was not intended to be critical or insulting. Nonetheless, the optics changed with the realization that there are additional factors that might influence the decision to use SPECT or SPECT/CT in lung scanning. Not the least of these factors is the excellent positive and negative predictive value for planar V/Q. This feature of V/Q is challenged when single-day, 99mTc-based ventilation and perfusion imaging is undertaken, especially when the ratio of count rate differences is not met. To further clarify, an informal poll was posted for 24 h by 2 separate nuclear medicine technologist groups: one comprising predominantly members from the United States and another comprising predominantly Australian members (Table 1). Although not expected to be quantitatively representative of either population, the insights did provide a snapshot with generalizability of findings. The stark contrast in results, with 67% of respondents from the United States indicating they performed planar-only studies, compared with just 3% of Australian sites, is thought to reflect, in part, the greater suitability of Technegas for SPECT than 81mKr, 133Xe, or 99mTc aerosol ventilation studies. As previously outlined (3), Technegas is considered the preferred ventilation method in more than 60 countries, including Australia, yet has limited adoption in the United States. Indeed, several additional comments by U.S. respondents indicated that poor ventilation SPECT is a barrier whereas omission of the ventilation scan in favor of CT for patients during the COVID era is a driver for SPECT/CT. Conversely, the principal discussion among the Australian respondents was related to advanced SPECT/CT techniques using breath-hold approaches and justification of base to apex against radiographer-preferred apex to base protocols. The impending approval of Technegas by the Food and Drug Administration in the United States may change that landscape and, therefore, demands a detailed discussion of the advances that allow the entire V/Q protocol to move to 3-dimensional SPECT or SPECT/CT imaging.
Summary of Results of 24-Hour Social Media Poll Conducted August 22, 2022
THE V/Q TEST
Although pulmonary embolism is the principal pathology of interest in V/Q lung scanning, it is not the only application investigated with the V/Q scan. The basic premise in pulmonary embolism is the mismatch scan, in which a perfusion deficit is accompanied by normal ventilation. The V/Q mismatch, however, can be caused by pathology other than pulmonary embolism, and not all pulmonary emboli produce a mismatch (4). Acute pulmonary embolism may partially resolve (diminishing the perfusion defect) or may progress to infarction, which produces a matching V/Q defect (4). Traditionally, the chest radiograph was used to improve the accuracy of the V/Q scan and to identify those patients more suited to CT pulmonary angiography (CTPA). The use of SPECT V/Q independently improves V/Q accuracy and, when combined with CT, produces coregistration with anatomic detail superior to that of chest radiographs. The possibility of combining SPECT with CTPA creates an additional layer of insight that demands attention. The potential redundancy of the chest radiograph and the ventilation scan warrant consideration with the emergence of lung V/Q SPECT/CT and V/Q SPECT/CTPA.
Planar V/Q has several challenges. First, perfusion defects are segmental or subsegmental, often with overlap of segments using 2-dimensional planar imaging. As a result, identification of specific defect localization or segments is difficult (5). Second, the overlap of tissues using 2-dimensional images means that a perfusion defect may have events superimposed from over- or underlying normally perfused lung tissue. This shine-through can confound perfusion defect detection and interpretation (5). For example, a small subsegmental defect may have sufficient superimposed counts to go undetected or the perfusion deficit may be underestimated for a larger defect. Third, the shine-through of ventilation data in the perfusion data can also confound perfusion defect detection and interpretation. The count rate difference between 99mTc-based ventilation and the subsequent 99mTc-based perfusion study is ideally a minimum of 7 times higher perfusion counts, with 4 times being an absolute minimum. This is seldom actually confirmed before imaging or reporting and has the same implications as anatomic shine-through either globally or, particularly for aerosol studies that can produce airway deposition at the branching of the airways, focally. Next, there are variable approaches to ventilation that directly impact the interpretability of the studies and the proportion of indeterminate studies. Availability of Technegas as the preferred method is not universal, which also influences the lack of universality of interpretation criteria. Adoption of Technegas could use a same-day protocol with ventilation followed by perfusion and this protocol comes with the potential “shine-through” (Fig. 1) issues discussed above. Alternatively, a two-day protocol with perfusion first and the ventilation only performed on abnormal perfusion studies could be adopted. The latter approach has been revisited during the 2019 coronavirus disease pandemic because of concerns about aerosols and disease transmission. It may also reduce the radiation dose for some patients (normal perfusion) and eliminate ventilation shine-through on the perfusion study but delays confirmatory diagnosis by 24 h in an emergency. Finally, the interpretation criteria generally used are not fit for the purpose and have largely migrated from probabilistic approaches to categoric classification.
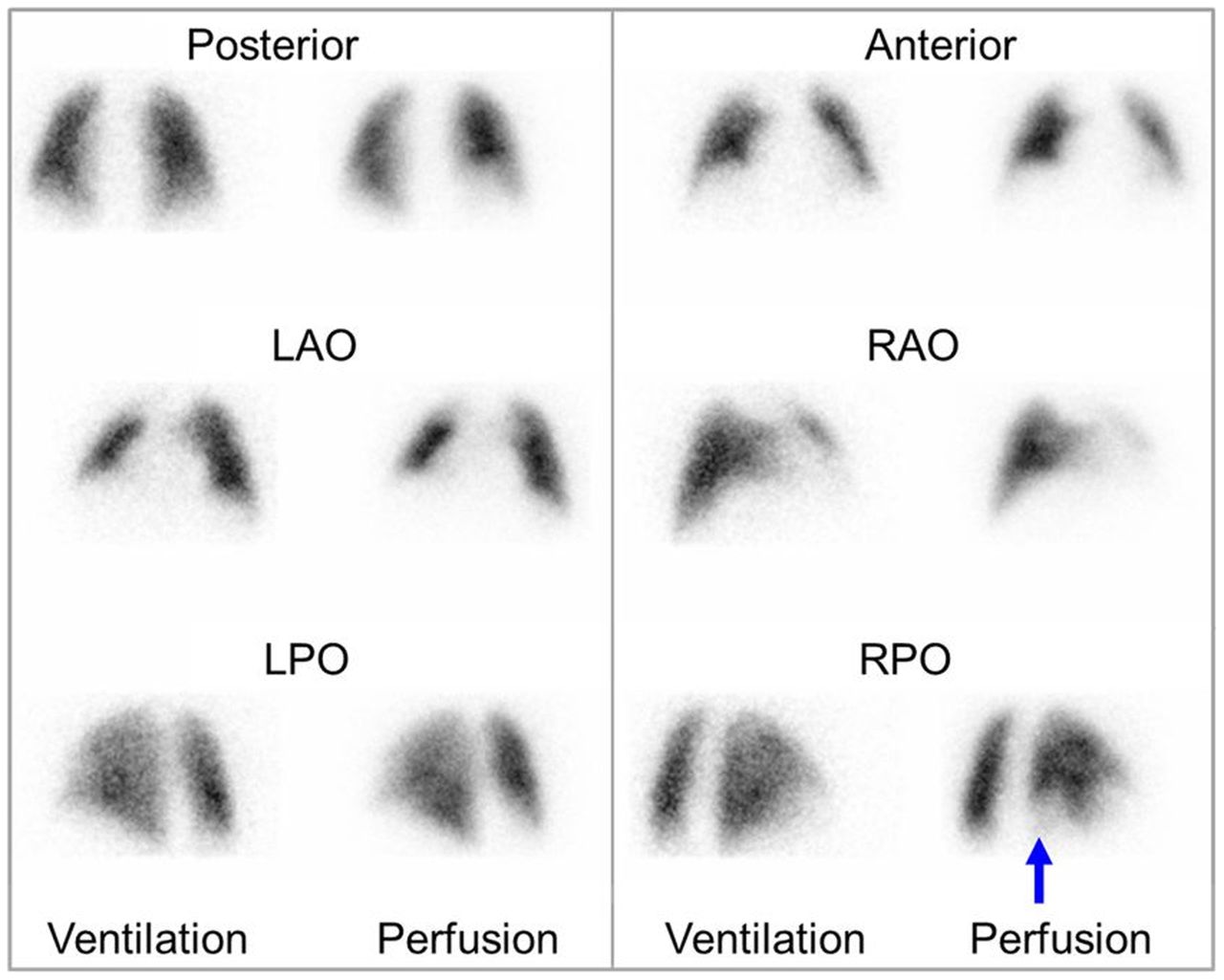
Planar V/Q scan with single mismatched perfusion defect (arrow) suggestive of intermediate probability of pulmonary embolism. LAO = left anterior oblique; LPO = left posterior oblique; RAP = right anterior oblique; RPO = right posterior oblique. (Reprinted from (5).)
Despite significant advances in the technology associated with nuclear medicine imaging, planar V/Q imaging has not evolved since the mid-1980s despite the application of advanced technology and associated protocol modifications to most other long-standing procedures. The arguments against SPECT V/Q adoption are largely the same confronting the transition to SPECT and gated SPECT myocardial perfusion. Transitioning to Technegas might be analogous to displacement of 201Tl by 99mTc-based agents for myocardial perfusion. The additional time required for acquisition of both planar and SPECT acquisitions during the learning phase of SPECT adoption is shared between V/Q and myocardial perfusion, although several authors have shown how to produce adequate pseudoplanar images from the SPECT data. The invested experience in planar interpretation and associated new learning are common reasons to avoid the transition to SPECT previously cited for the myocardial perfusion SPECT transition. Although transition to Technegas confronts regulatory hurdles in the United States, perhaps the only barrier elsewhere to the adoption of SPECT V/Q is the net benefit given that planar V/Q has high accuracy and that the incremental benefit of SPECT is much smaller than that of myocardial perfusion imaging.
Regardless of the 99mTc ventilation method adopted (radioaerosol or Technegas) or the imaging approach used (planar or SPECT), both the ventilation and the administration of the perfusion radiopharmaceutical should be performed with the patient supine to minimize the effects of gravitational gradients. The ventilation count rate should not exceed 1,000–1,500 per second; otherwise, the residual ventilation counts may reduce the detectability of perfusion defects. The Rose model associated with image contrast and object detection determined, mathematically, that human perception requires a signal-to-noise ratio of at least 5–7 (6). This conflicts with advice from the Society of Nuclear Medicine and Molecular Imaging guidelines (7) suggesting that a count rate of 3–4 times is adequate and that decreased contrast may lead to increased false-negative studies. With 100 MBq of 99mTc-macroaggregated albumin producing count rates of 2.3–5.0 per second (decreasing with increasing body mass index), a patient dose of 200–250 MBq of 99mTc-macroaggregated albumin is generally required. When ventilation has been efficient and produced higher count rates, a delay before the perfusion administration and acquisition should be used until count rates reduce to 1,000–1,500 per second. Increasing the administered dose beyond 250 MBq imposes not only a higher radiation dose to the patient but also a greater risk due to increased capillary blockade.
SPECT V/Q
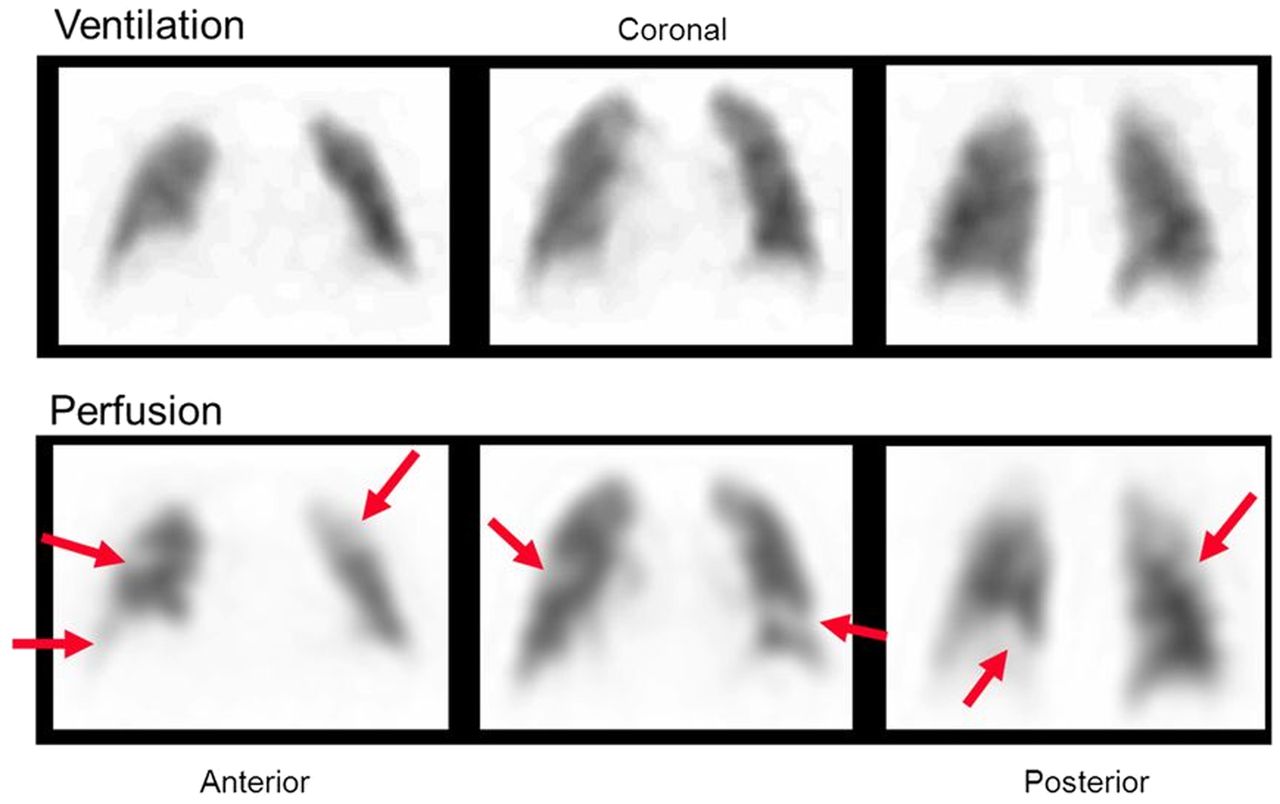
SPECT and the associated 3-dimensional imaging overcomes many of the challenges of planar imaging. First, SPECT allows more accurate localization of segmental and subsegmental perfusion defects. Second, SPECT eliminates over- and underlying tissues and the associated shine-through, which enhances defect detection and interpretation. Third, the ventilation study shine-through can be normalized and subtracted, and parametric approaches can be used (e.g., the V/Q ratio). All 3 of these factors enhance V/Q contrast and the ability to detect perfusion defects. Importantly, SPECT can improve the sensitivity, specificity, accuracy, and reproducibility of the V/Q study compared with planar imaging and can reduce the proportion of indeterminate studies (Table 2) (5). SPECT has been reported to increase detection of segmental perfusion defects by more than 10% and subsegmental perfusion defects by as much as 80% (Fig. 2) (8). Indeed, the advantages of SPECT V/Q over planar V/Q are so well established in the literature that SPECT V/Q is standard practice in many European and Latin American countries, Canada, and Australia. SPECT V/Q is also the preferred approach of the European Association of Nuclear Medicine (9), whereas the Society of Nuclear Medicine and Molecular Imaging guidelines indicate that, except in patients with complex comorbidities, planar V/Q remains preferred in the United States (10). This view reflects lack of access to a suitable ventilation agent at present and may change in the future. One should keep in mind, however, that simultaneous V/Q imaging with continuous tidal breathing using 81mKr for ventilation has been widely reported as providing high-quality V/Q SPECT studies.
Characteristics Enhanced by SPECT over Planar Imaging for V/Q Scan

SPECT acquisition protocols should include 120–128 projections using a dual-detector γ-camera over 360° with a 128 × 128 matrix and high-resolution collimation. The ventilation study is typically 10–12 s per projection (but can be 15–20 s), whereas the higher-count perfusion study is typically 8–10 s per projection (but can be 12–15 s). For a single-day V/Q scan, the patient should be positioned supine with arms hyperextended above the head and an injection line in place in either arm. On completion of the ventilation SPECT, without the patient moving, the 99mTc-macroaggregated albumin should be administered and perfusion SPECT commenced. For convenience, protocols can be established to perform dual SPECT studies using the same orbit parameters, with the ventilation rotating clockwise and then the perfusion simply rotating back counterclockwise. The SPECT images should be reconstructed using an iterative algorithm, typically ordered-subset expectation maximization. The images can be used to produce planar imaging–equivalent images from the dataset. One approach is to sum several projections from either side of the required view (anterior, for example, would be projection 1 summed with projections 2, 3, 119, and 120) (11). A better approach is to reproject the SPECT data with an associated attenuation map (12). More commonly, however, the SPECT data provides the insights required and the extracted planar data are not required or produced. The ordered-subset expectation maximization parameters depend on the acquisition parameters and total counts per pixel; however, 8 subsets and 4 iterations with a low-pass filter are typical, with a 3- to 4-mm slice thickness. SPECT V/Q data should be displayed after simultaneous reconstruction as V/Q pairs sequentially for each projection (Fig. 3). Representative slices can be extracted to correlate with parametric images (Fig. 4).
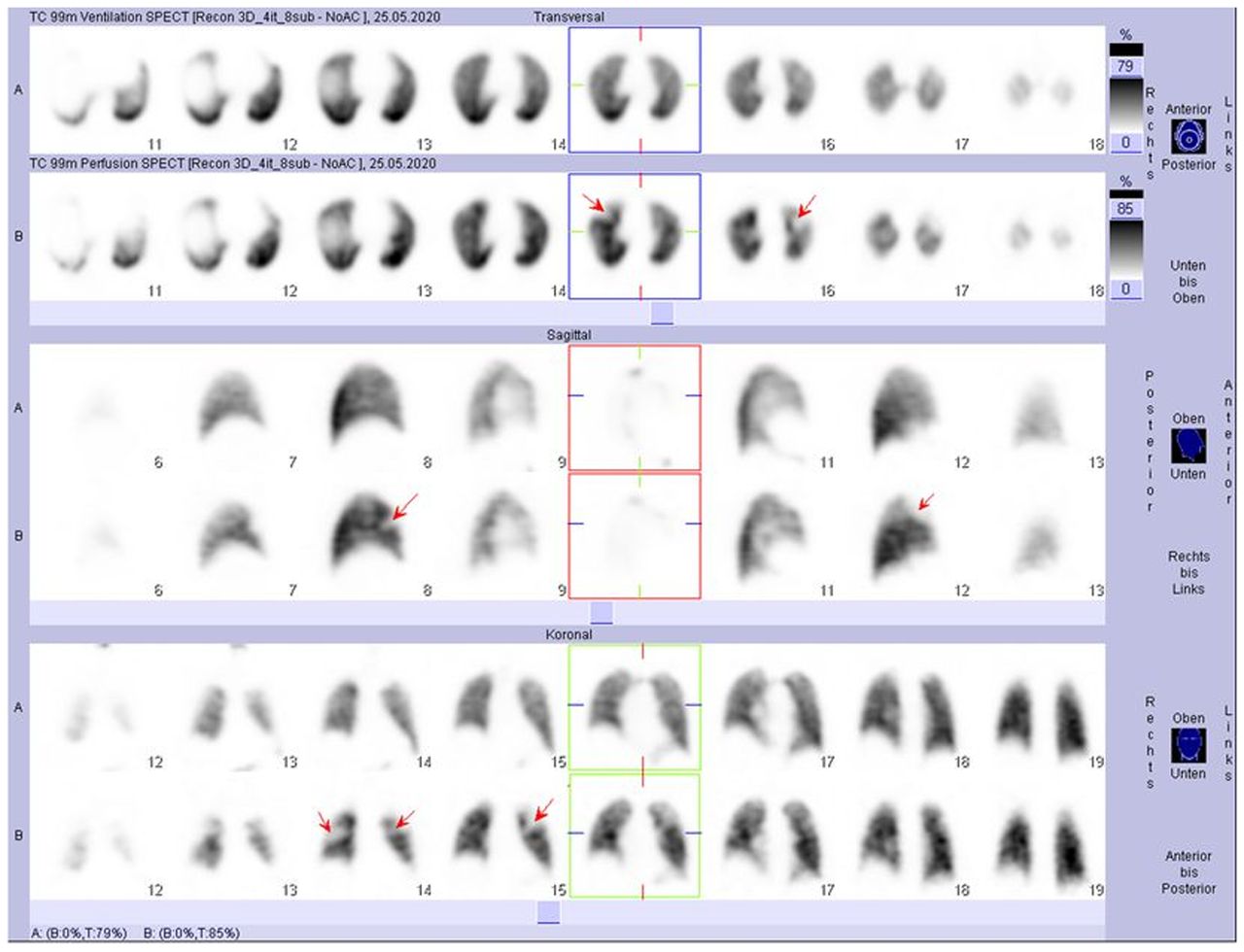
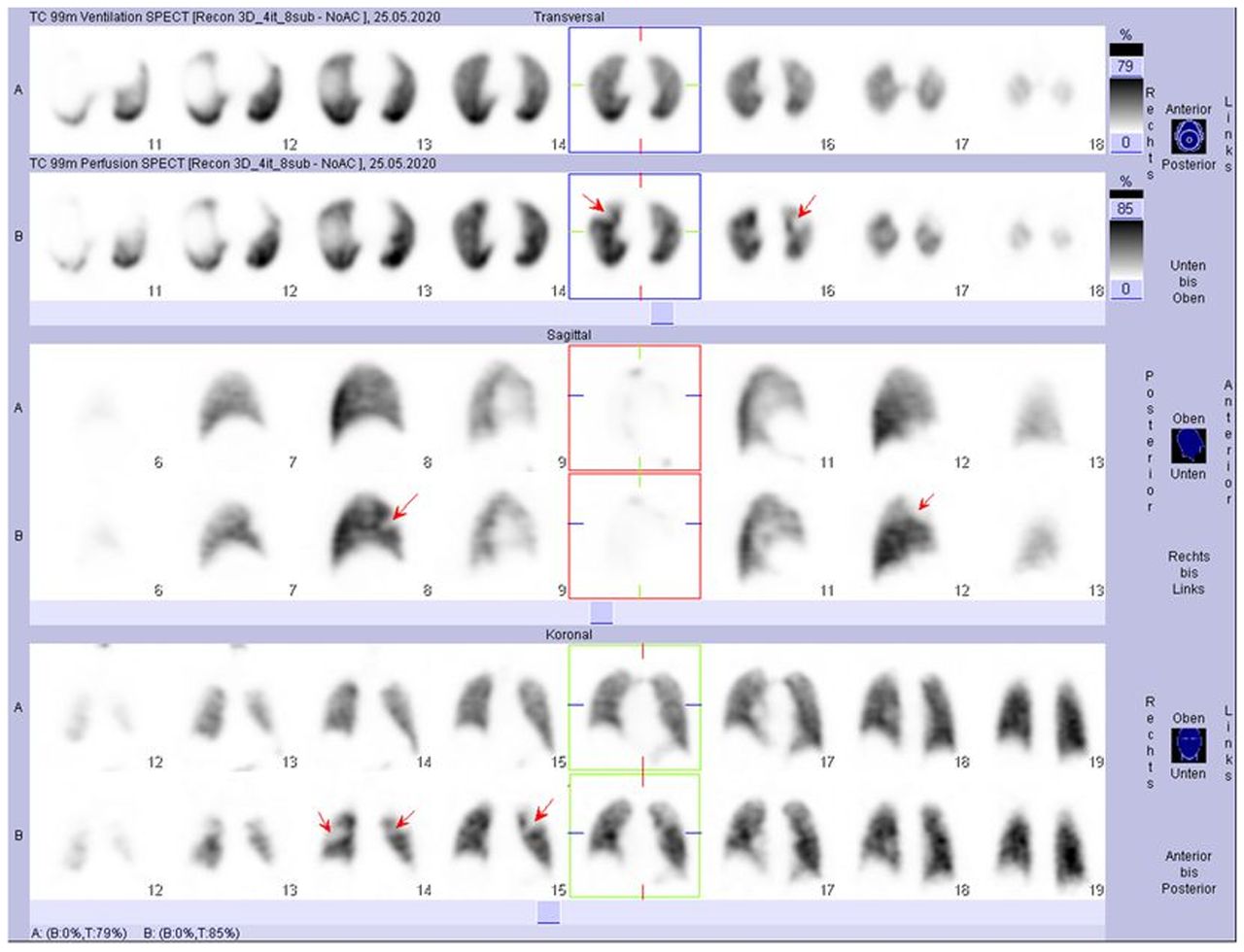
Slice-by-slice V/Q pairs for SPECT data with arrows highlighting mismatch defect typical of pulmonary embolism. (Reprinted from (26).)
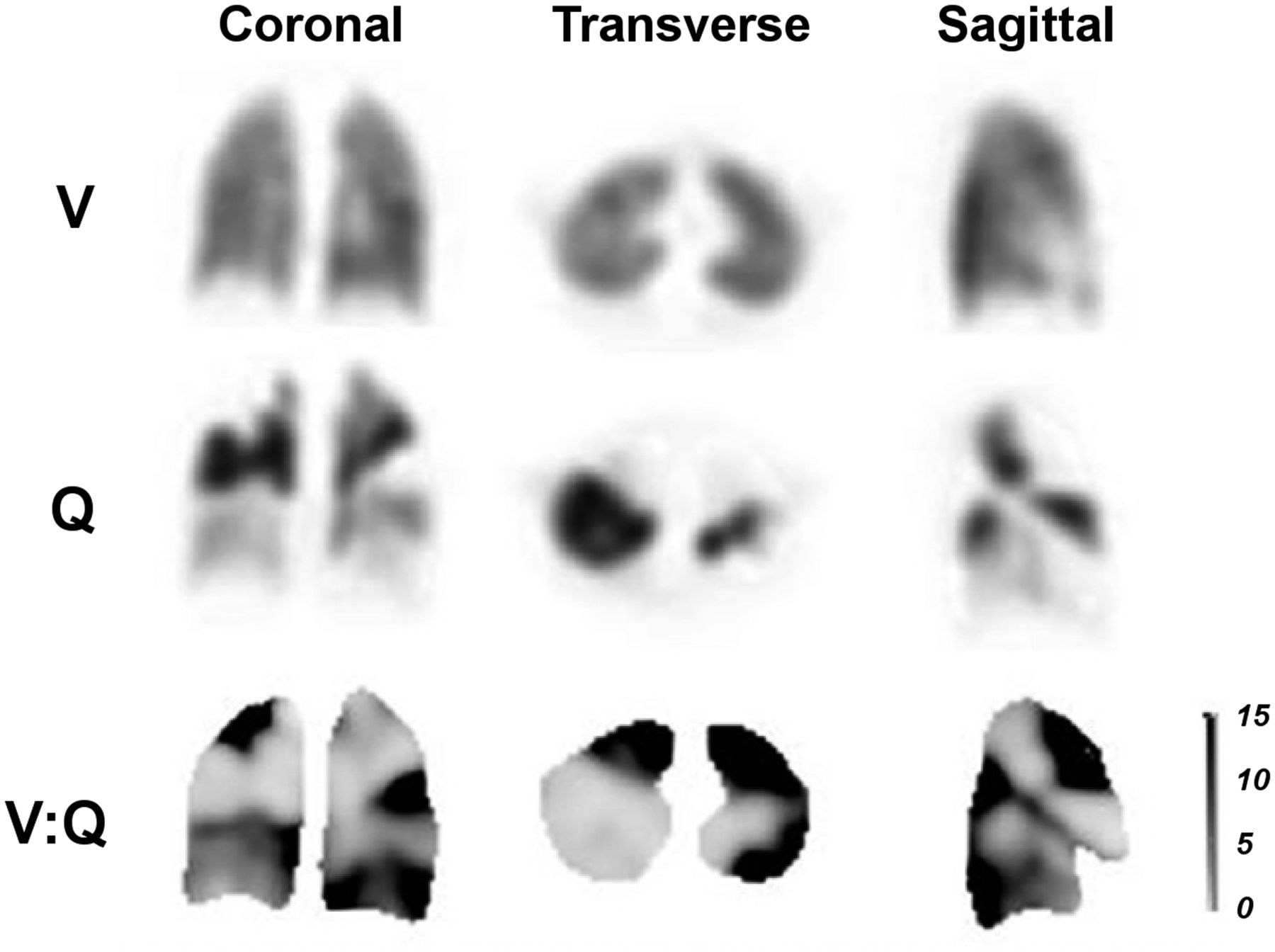
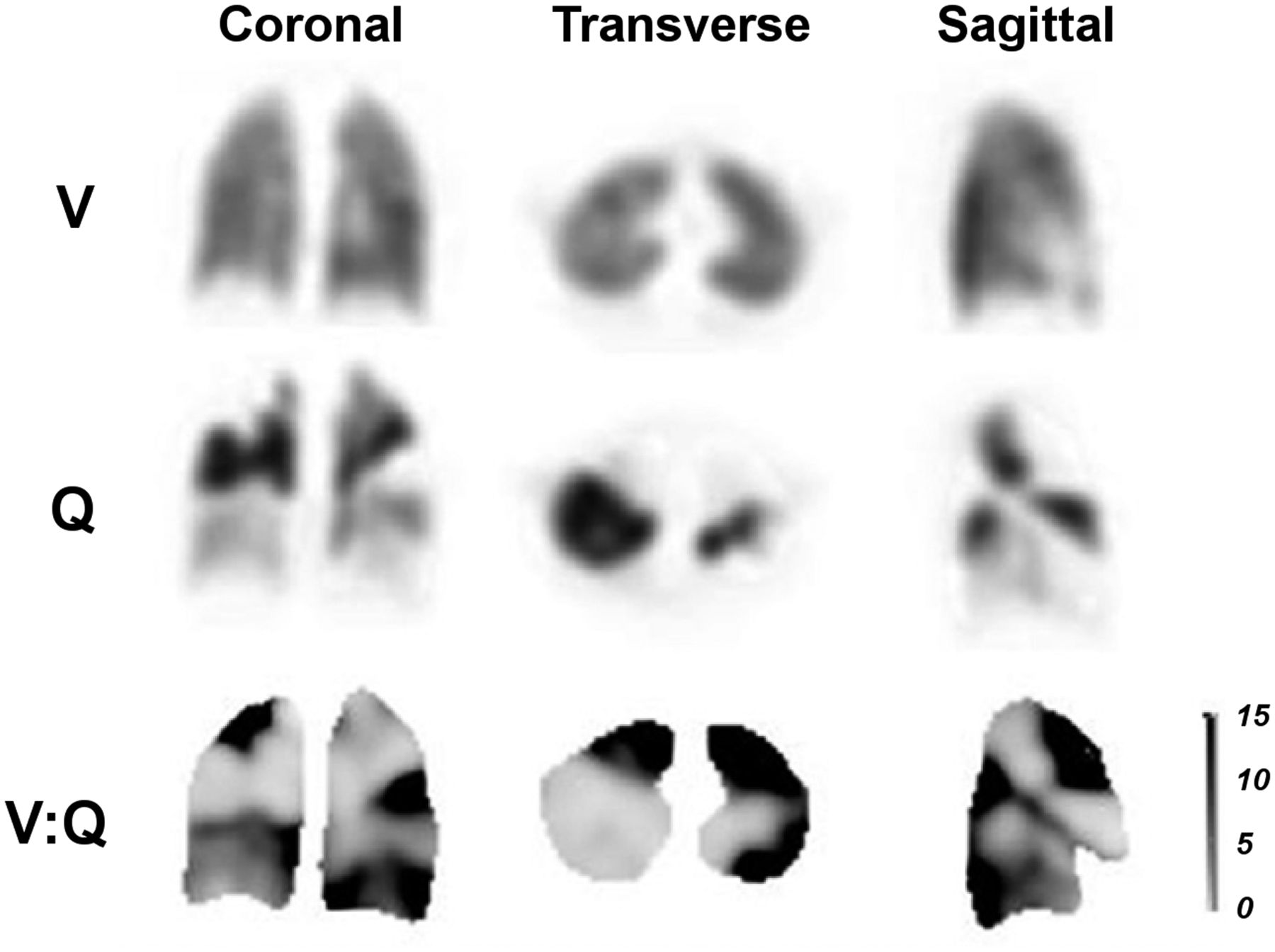
Representative slices for ventilation (top), perfusion (middle), and parametric V:Q ratio images (bottom), with positive segments for pulmonary embolism denoted by darker shading on parametric images. (Reprinted with permission of (27).)
SPECT/CT V/Q
The low-dose CT scan acquired with SPECT reduces the radiation dose to the patient compared with a diagnostic CT scan. When used in conjunction with V/Q, SPECT provides attenuation correction, localization, and additional insight into vascular, parenchymal, and pleural abnormalities (4). For example, low-dose CT provides richer detail than chest radiography in identifying hypoperfused lung (Westermark sign), pulmonary artery enlargement (Palla sign and Fleishner sign), or pulmonary artery tapering (knuckle sign) that may support a diagnosis of pulmonary embolism (Fig. 5). Conversely, opacities more consistent with pathologies that cause a matched V/Q defect (Fig. 6) and, thus, less likely to represent pulmonary embolism can also be identified on low-dose CT (e.g., consolidation, bullae, atelectasis, interstitial disease, or space-occupying lesions). The combination of SPECT/CT in the evaluation of pulmonary emboli may reduce the false-positive rate, improving specificity (4). Although it seems intuitive that CT may make the ventilation study redundant, evidence suggests that the ventilation study substantially improves test specificity over perfusion SPECT/CT alone (13).
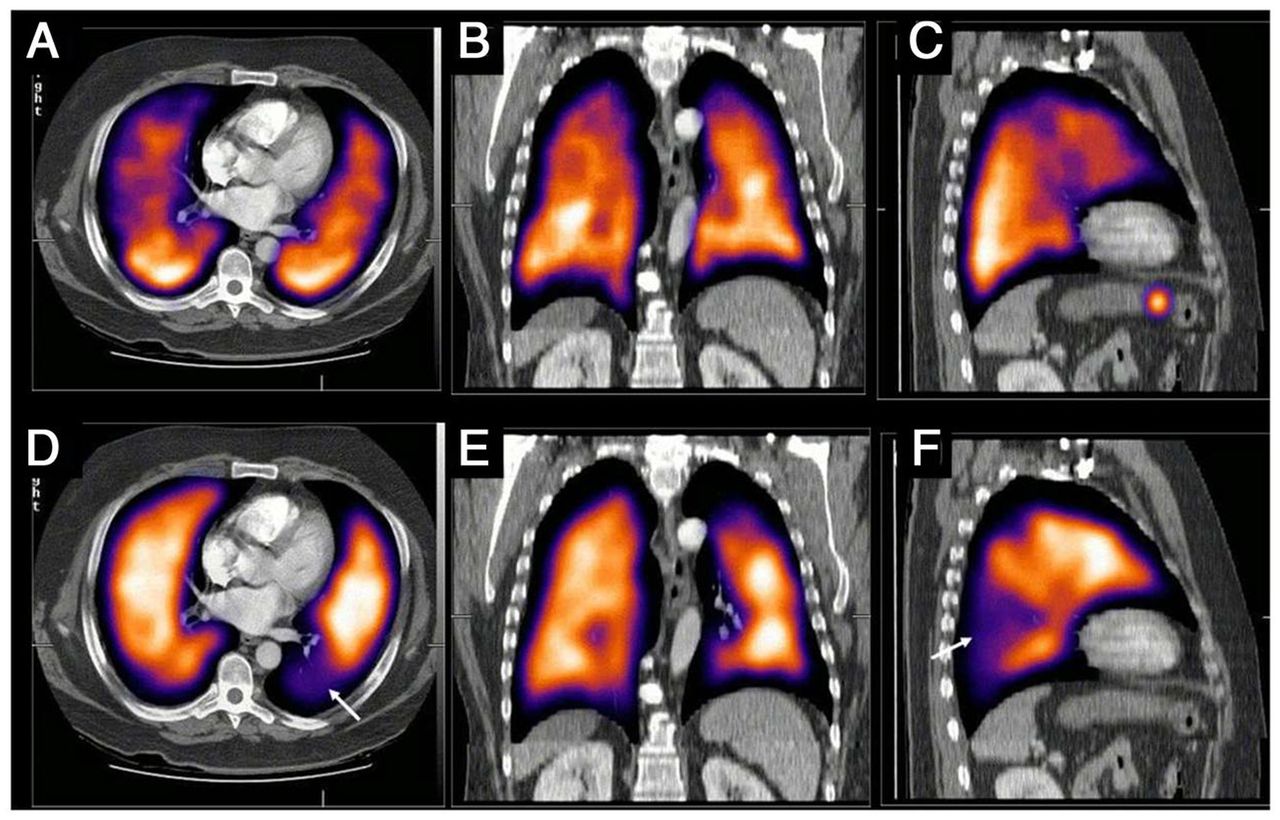
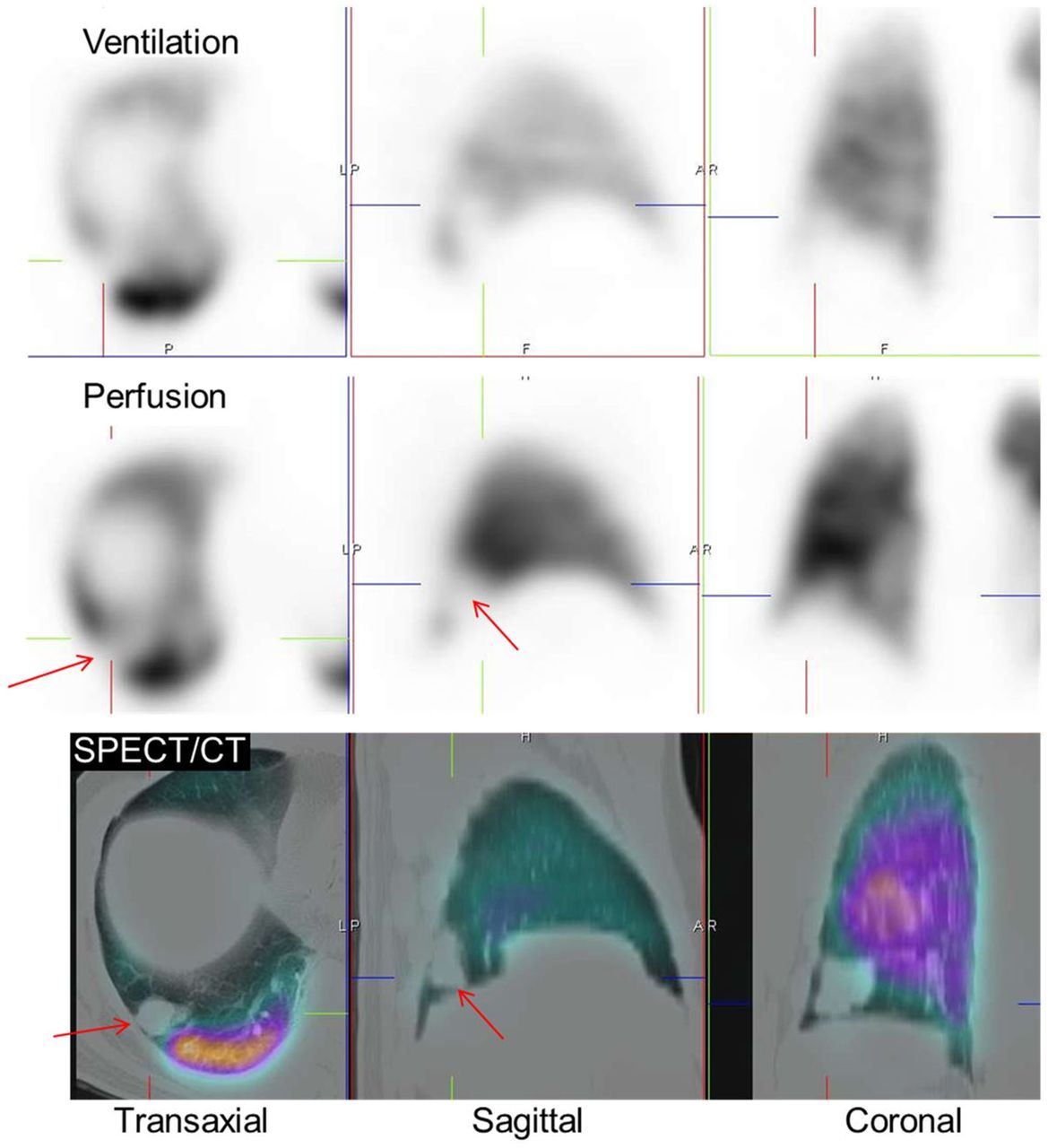
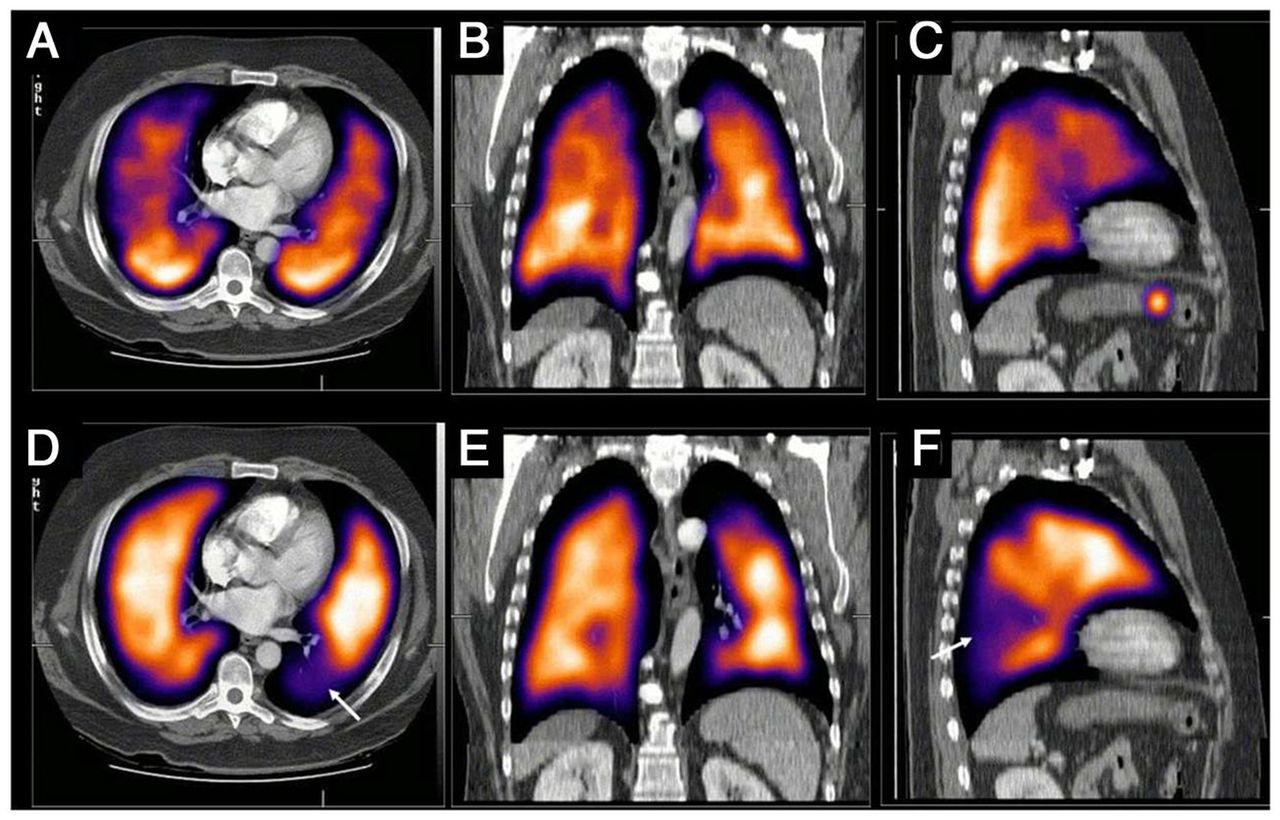
Representative SPECT/CT images of lung ventilation (top) and perfusion (bottom) demonstrating segmental perfusion defect (arrow in D and F) in left lower lobe with no CT opacity or matched ventilation defect consistent with pulmonary embolism. (Reprinted from (3).)
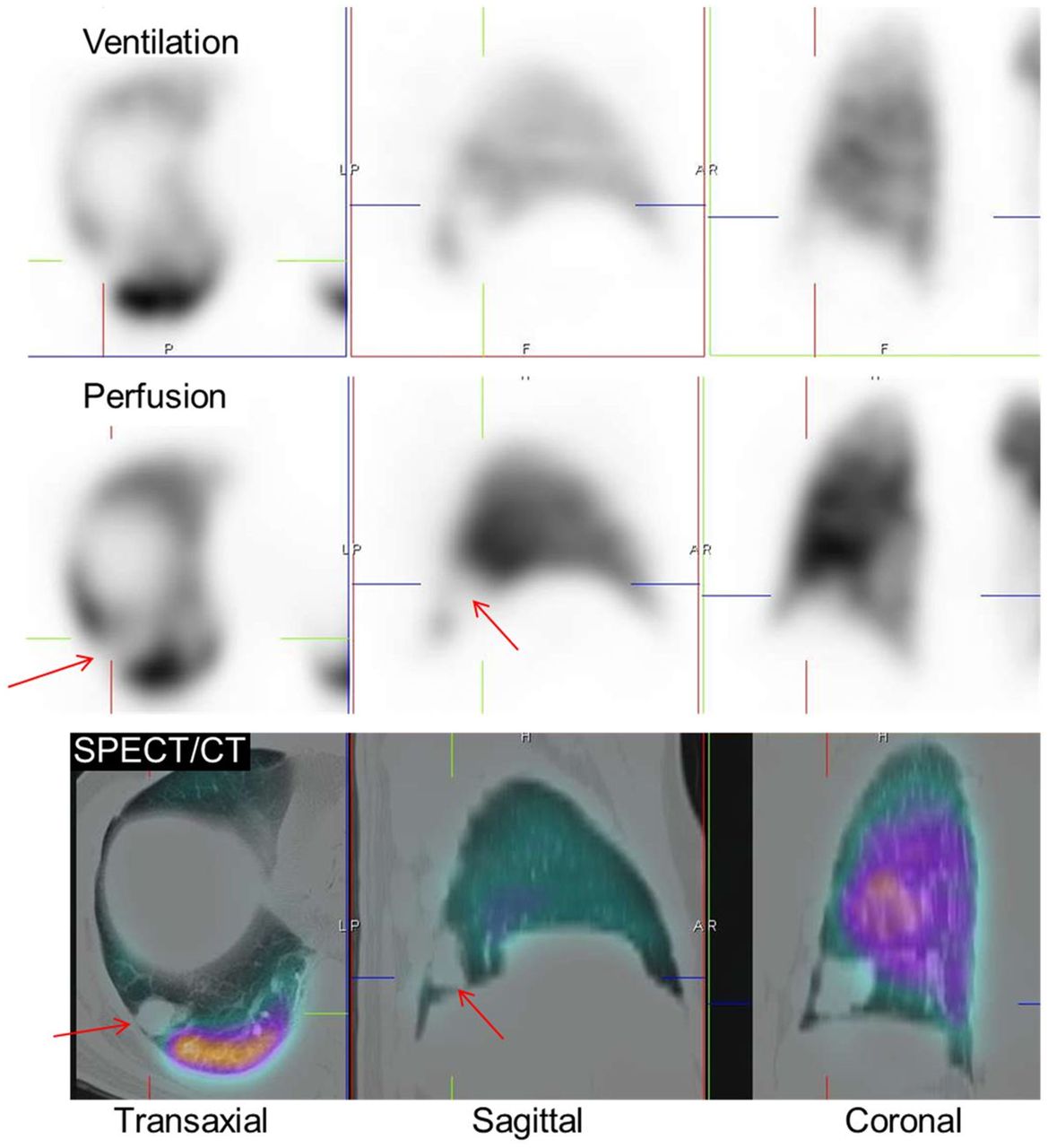
Fusion of SPECT and low-dose CT showing opacity (arrows) on CT corresponding to perfusion defect producing matching defect consistent with lung metastases. (Reprinted from (5).)
For simple attenuation correction, low-dose CT parameters might include 120 kVp, 10 mAs per slice, and a pitch of 1.0–1.5 to produce an additional radiation dose of less than 1 mSv. More typically and of greater value is a low-dose CT scan for coregistration and mapping of anatomic information. This low-dose CT scan produces a higher dose of 2–3 mSv using 80–120 kVp, 20 mAs per slice, a 512 × 512 matrix, and a pitch of 0.8 (14). Specific parameters and doses will vary depending on the CT system used. The V/Q SPECT scan alone is typically 2 mSv (4). A full diagnostic CT scan without contrast medium may also be performed using 100–140 kVp, 130–200 mAs per slice, a 512 × 512 matrix, and a pitch of 0.9, producing a dose of 3–8 mSv (15). Although not feasible for the SPECT phases, a mid-inspiration breath-hold should be used for the CT, with imaging adjusted to base to apex rather than the traditional apex to base to minimize coregistration artifacts. In the absence of a mid-inspiration breath-hold for the CT scan, shallow, continuous breathing can be used (4).
SPECT/CT V/Q AND CTPA
It is possible to combine SPECT and CTPA studies using software fusion, and although this adds insight, it also adds radiation exposure and confronts registration errors. Hybrid technology allows SPECT/CT and SPECT/CTPA to be performed with hardware fusion that overcomes the registration errors of software fusion (Fig. 7). The value of SPECT/CTPA is the combination of the highly sensitive perfusion map with the highly specific angiographic map to enhance diagnostic efficacy. In most patients, despite the feasibility of SPECT/CTPA in a single session, both procedures are usually neither required nor justified.
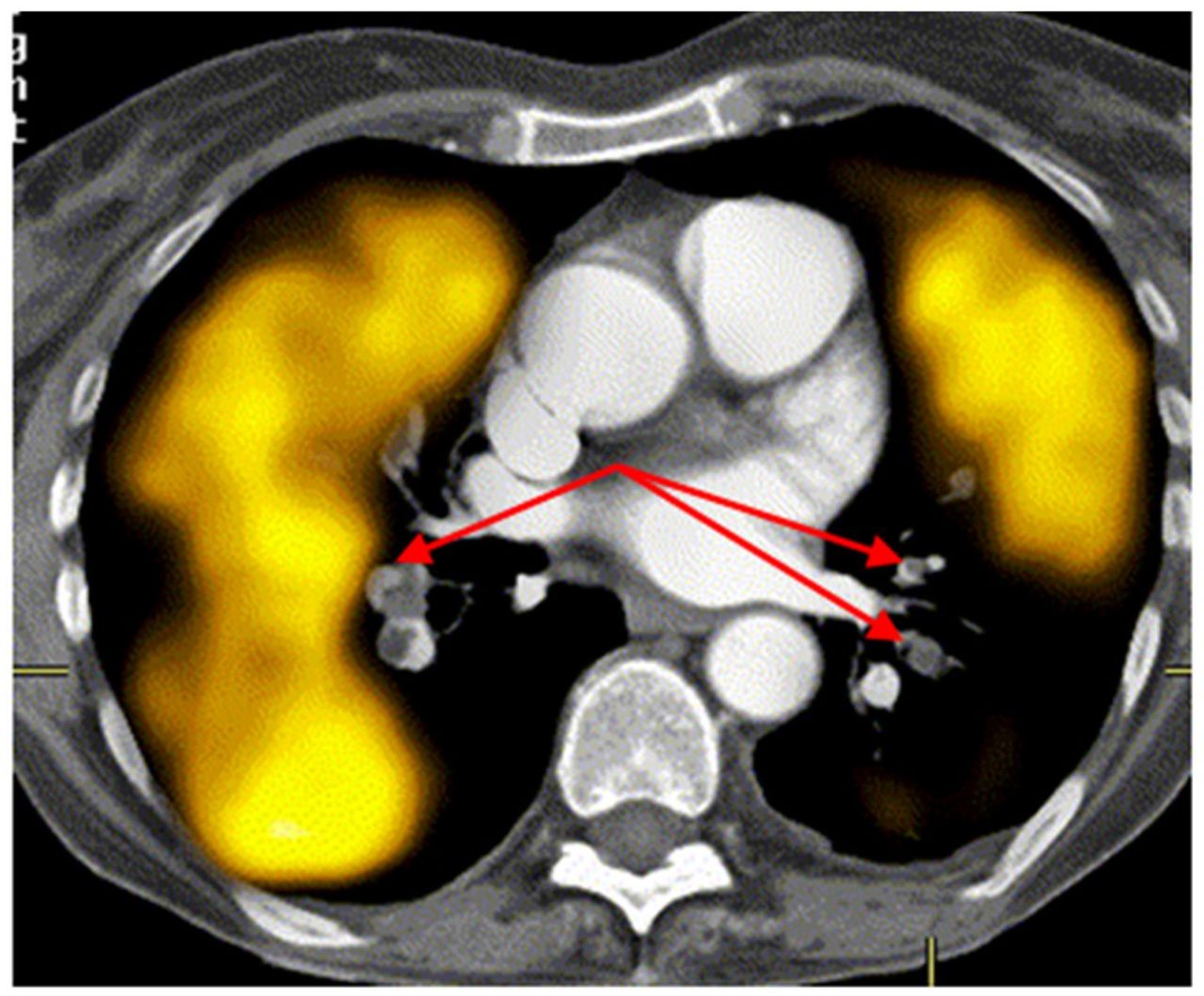
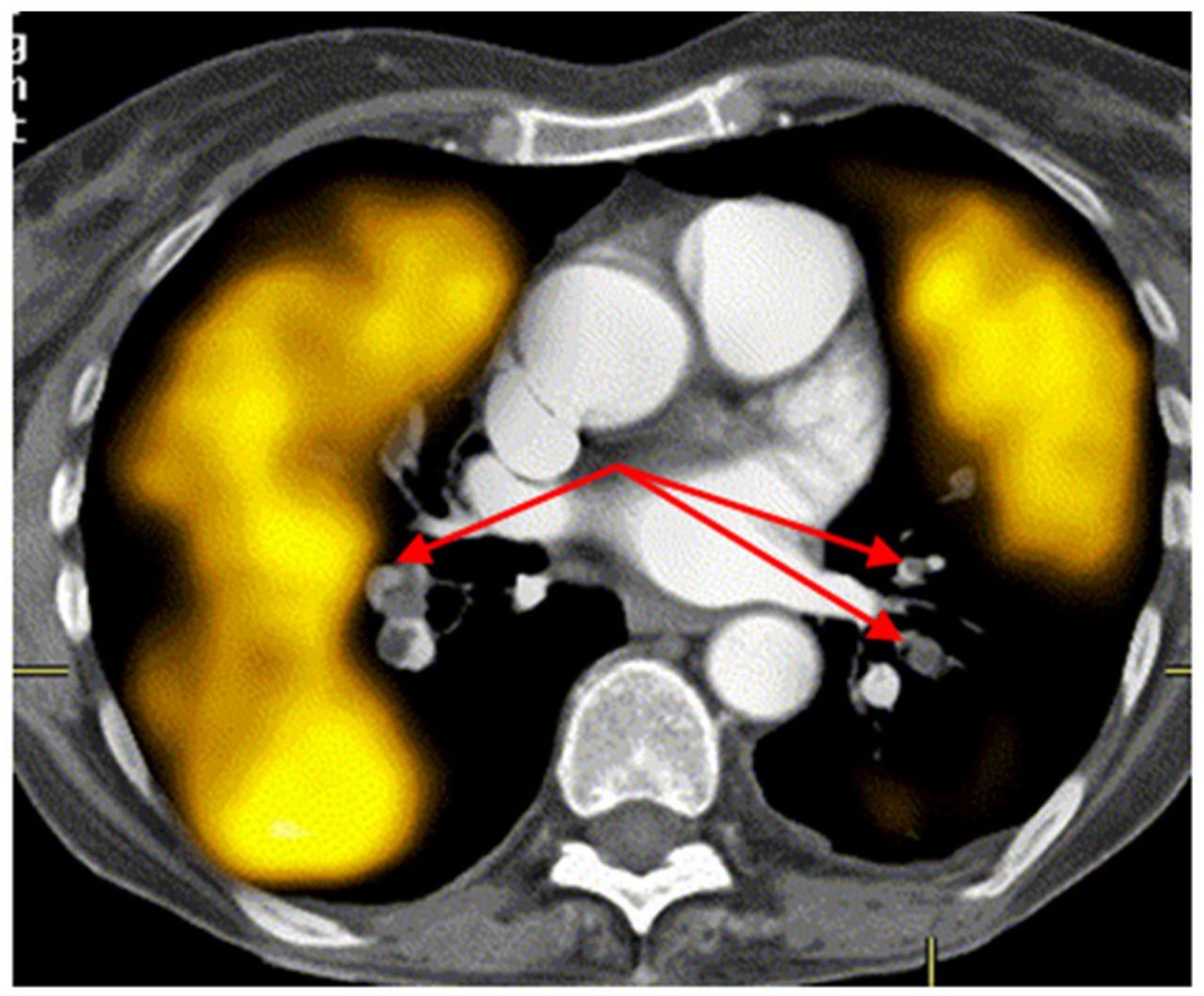
Fused perfusion SPECT and CTPA showing pulmonary emboli (arrows) bilaterally in arteries with associated perfusion defects on SPECT. (Reprinted with permission of (4).)
CTPA might be performed using 80–120 kVp, 150–200 mAs per slice, a 512 × 512 matrix, and a pitch of 0.9 with 80 mL of iodine contrast medium using bolus tracking and a deep-inspiration breath hold producing a dose upward of 8–20 mSv (14,16). A key concern for CTPA is the adverse effects from the contrast medium, the risk of nephropathy, and the high radiation dose. These factors preclude justification of CTPA in premenopausal women, pregnant women, patients with renal dysfunction or diabetes, and patients taking some types of medications. The breast radiation dose during CTPA is a significant issue that perhaps does not get enough attention. The breast dose from CTPA ranges from 10 to 70 mSv—equivalent to as many as 25 mammograms or 400 chest radiographs, which substantially increases the lifetime risk of developing breast cancer (16).
Although adverse reactions to iodinated contrast medium have been reduced with the introduction of nonionic, low-osmolality contrast media, there remains a 3% adverse reaction rate with a 1 in 170,000 fatality rate (17). Acute kidney injury and contrast-induced nephropathy are of particular concern, with as many of 3% of contrast administrations resulting in contrast-induced nephropathy (16). Generally, contrast-induced nephropathy is evidenced by increased serum creatinine; however, these effects may not be noted until 2 d after contrast administration, peaking at 4 d after the scan and returning to baseline after 1–3 wk later (18). It is likely that in many patients with contrast-induced nephropathy, it goes undetected, and consequently, the incidence is probably underestimated. Although the risk factors for contrast-induced nephrotoxicity are well documented (e.g., renal dysfunction, diabetes, and congestive heart failure), there is a paucity of literature outlining the longer-term effects of contrast media on renal function or on the confounding effects of contrast media on medications that increase the risk of renal toxicity (e.g., the triple whammy of a concurrent diuretic, angiotensin-converting enzyme inhibitor, or angiotensin receptor blocker and a nonsteroidal antiinflammatory drug added to the risk of the contrast medium). As a general rule, an effective glomerular filtration rate below 30 mL/min/1.73 m2 estimated from serum creatinine levels is a relative contraindication to contrast medium (17,19). Contrast-induced nephropathy increases in incidence from 3% in normal renal function (>60 mL/min/1.73 m2) to 12%–27% in renal dysfunction to 50% in diabetic nephropathy (17). Indeed, concurrent use of metformin with chronic renal insufficiency and intravenous iodinated contrast medium is associated with a 50% mortality rate (17,19).
CONCLUSION
The literature tends to be mixed and contradictory in terms of appropriate investigation algorithms for pulmonary embolism. This may reflect political, health, economic, or professional preference-based factors. The European Association of Nuclear Medicine provides an evidence-based diagnostic algorithm that serves as an excellent resource (9). The Society of Nuclear Medicine and Molecular Imaging guidelines (7) require updating to reflect the advances discussed. For the patient presenting with suspected acute pulmonary embolism, if V/Q SPECT is available, that is the preferred approach. A positive scan result should direct treatment for pulmonary embolism, a negative scan result excludes pulmonary embolism, and a nondiagnostic SPECT result should be followed up with CTPA. When V/Q SPECT is not available, CTPA or planar V/Q should be used (9). V/Q SPECT and SPECT/CT offer significant advantages over planar V/Q with or without the advantages of Technegas ventilation.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than March 2026. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
Published online Jan. 4, 2023.
REFERENCES
- Received for publication September 2, 2022.
- Revision received December 21, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.