

Abstract
After therapeutic pelvic radiation for malignancy such as prostate cancer, patients are at greater risk for spontaneous ureteral rupture. Bladder outlet obstruction and other more proximal causes of obstruction also exacerbate this vulnerability. Here we present a case of spontaneous ureteral rupture during a 99mTc-mercaptoacetyltriglycine nuclear renal scan secondary to Foley catheter obstruction in a 73-y-old man with a prior ureteral reimplantation procedure. Prompt detection of Foley catheter malfunction could potentially prevent such adverse events.
- ureteral rupture
- radiation
- Foley catheter malfunction
- prostate cancer
- ureteral implantation
After therapeutic pelvic radiation for malignancy such as prostate cancer, patients are at greater risk for spontaneous ureteral rupture. Bladder outlet obstruction and other more proximal causes of obstruction also exacerbate this vulnerability. Here we present a case of spontaneous ureteral rupture during a 99mTc-mercaptoacetyltriglycine nuclear renal scan secondary to Foley catheter obstruction in a 73-y-old man with a prior ureteral reimplantation procedure. Prompt detection of Foley catheter malfunction could potentially prevent such adverse events.
CASE REPORT
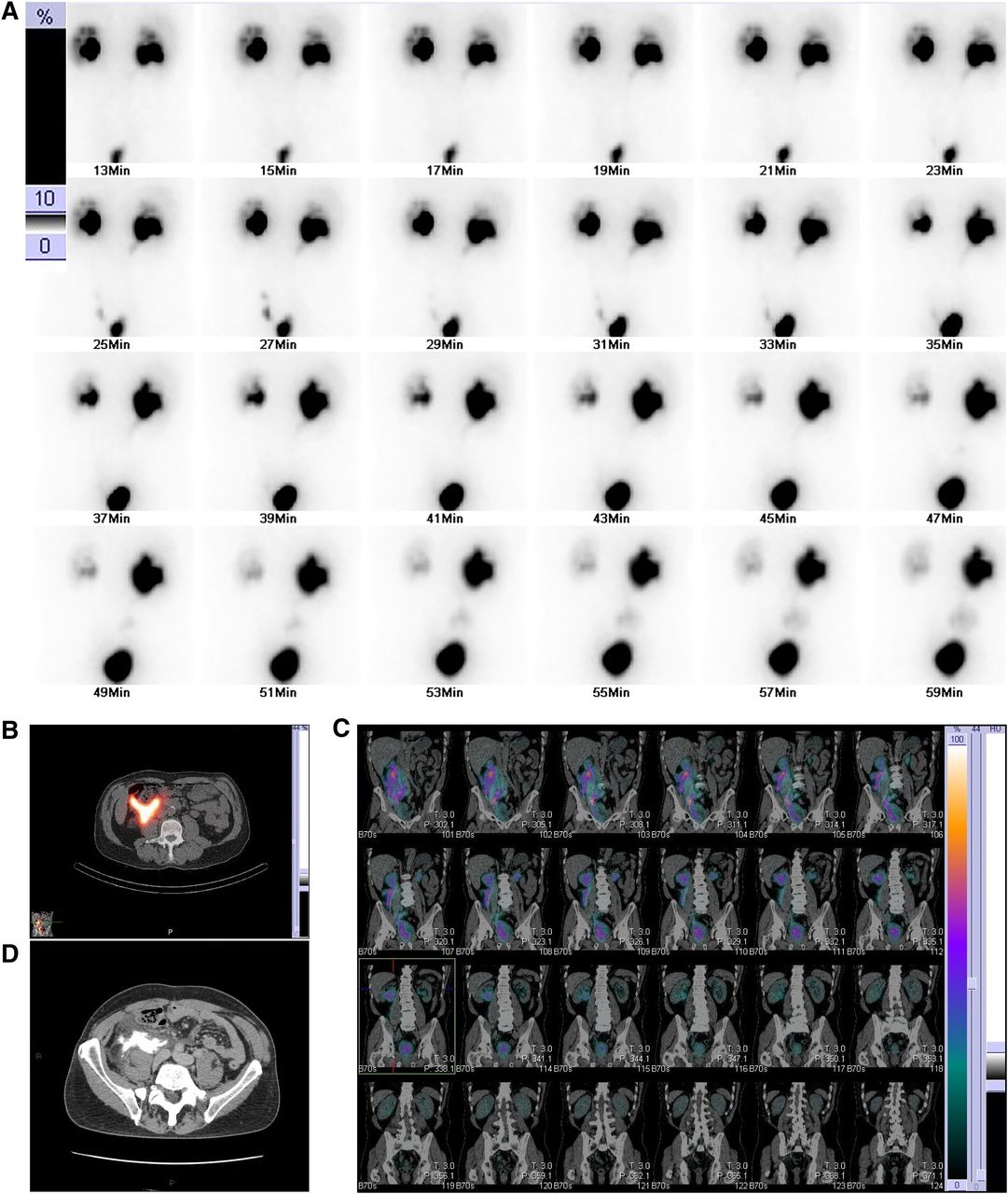
A 73-y-old man with a history of prostate cancer treated with external-beam radiation developed right ureteral stenosis, for which he underwent ureteral reimplantation with a psoas hitch approximately 1 y prior. A routine 99mTc-mercaptoacetyltriglycine renal scan was ordered to evaluate renal function and ureteral patency. Before starting the study, an interventional radiology nurse experienced difficulty placing the Foley catheter. The patient was subsequently injected with 367.41 MBq of 99mTc-mercaptoacetyltriglycine, and initially there was normal excretion of radiotracer from the kidneys with accumulation in the bladder (Fig. 1). At 30 min after radiotracer injection, 40 mg of furosemide were administered. Several minutes later, the patient reported discomfort in the right flank. Images demonstrated a progressive accumulation of radiotracer in the region of the mid-distal right ureter at approximately 47 min (Fig. 2A). SPECT/CT images displayed retroperitoneal accumulation of urine (Figs. 2B and 2C). This was also confirmed on contrast-enhanced CT delayed-phase images of the abdomen and pelvis, which demonstrated active extravasation of urine into the right retroperitoneal space (Fig. 2D). The patient was treated with a nephrostomy tube and right ureteral stenting.

99mTc-mercaptoacetyltriglycine planar image in posterior coronal projection showing radiotracer accumulation in bladder.

{kind=link}
{kind=link}
(A) 99mTc-mercaptoacetyltriglycine planar images in posterior coronal projection showing radiotracer excretion over time with accumulation in bladder and along mid-distal right ureter. (B) Axial SPECT/CT image with radiotracer accumulation along right psoas muscle. (C) Coronal SPECT/CT images with radiotracer extravasation following right ureteral tract over time. (D) Axial postcontrast CT of pelvis 10 min after intravenous contrast injection, with contrast accumulation along right psoas muscle.
DISCUSSION
Nontraumatic spontaneous ureteral rupture is a rare urologic emergency. Although no definite cause has been identified in this particular case (1), a few risk factors are noted, such as an obstructing calculus, a ureteral stricture, malignancy, and prior surgery (2). Our patient had a medical history of prior prostate cancer and prior ureteral surgery which increased his risk for nontraumatic spontaneous ureteral rupture. We hypothesize that the culminating factor leading to this adverse event was the Foley catheter malfunction during the renal scan. The ordering services and urology department requested Foley catheter placement before the study to ensure bladder emptying. Yet, traumatic placement of the Foley catheter led to clot formation and iatrogenic bladder outlet obstruction. As the renal scan progressed, images demonstrated rapid accumulation of urine with radiotracer into the bladder, an unexpected finding in a patient with a patent Foley catheter. Within minutes, this led to progressive distension of the right renal pelvis and right renal rupture.
Although commonly performed, transurethral catheterization can be a hazardous procedure leading to acute urinary retention in elder men (3). Early signs of Foley catheter malfunction manifest as decreased urine output, abdominal pain, a change in urine color, and urine leakage from the insertion site (4). A nuclear technologist can also detect Foley catheter malfunction on the images, when urine accumulates in the bladder or refluxes back into the pelvis. Early intervention on catheter obstruction is crucial in preventing adverse outcomes such as infections, bladder rupture, ureteral rupture, or, rarely, death (5).
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENTS
We acknowledge our patient—patients are the great source of learning. We also acknowledge PACS Administrator Shane Verrett for all his help with troubleshooting the technology and obtaining high-quality images.
Footnotes
Published online Apr. 16, 2024.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- Received for publication January 10, 2024.
- Revision received March 15, 2024.