

Abstract
We report a case of a large abdominal pseudocyst detected on scintigraphy in a patient with a history of ventriculoperitoneal shunt placement who presented with headache and suspected shunt malfunction.
- abdominal CSF pseudocyst
- VP shunt malfunction
- 111In-DTPA shunt study
Abdominal pseudocyst is an uncommon complication of ventriculoperitoneal shunting. It should be considered a differential diagnosis in patients with a ventriculoperitoneal shunt who complain of abdominal symptoms such as distention and pain. Early diagnosis improves clinical outcomes.
CASE REPORT
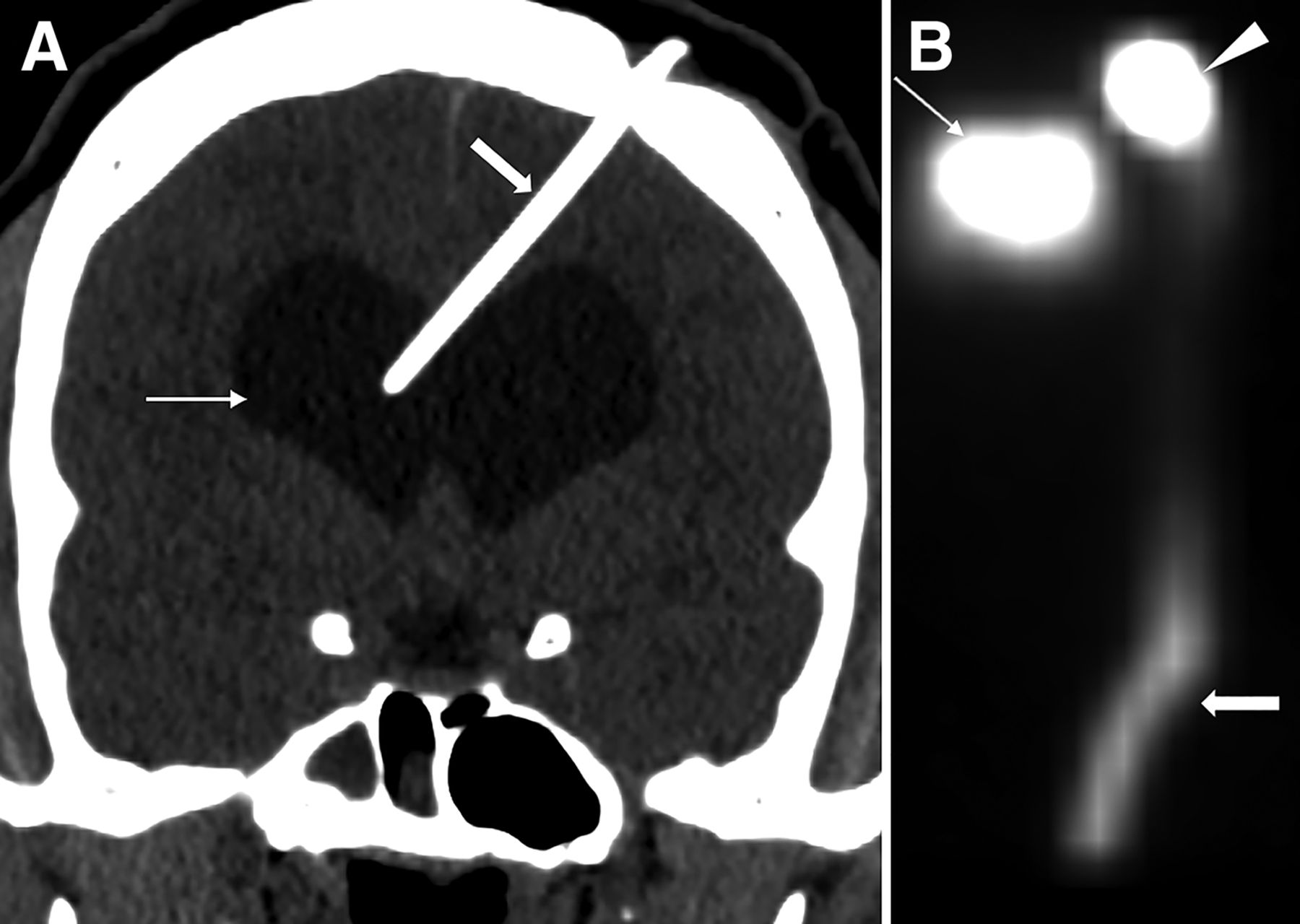
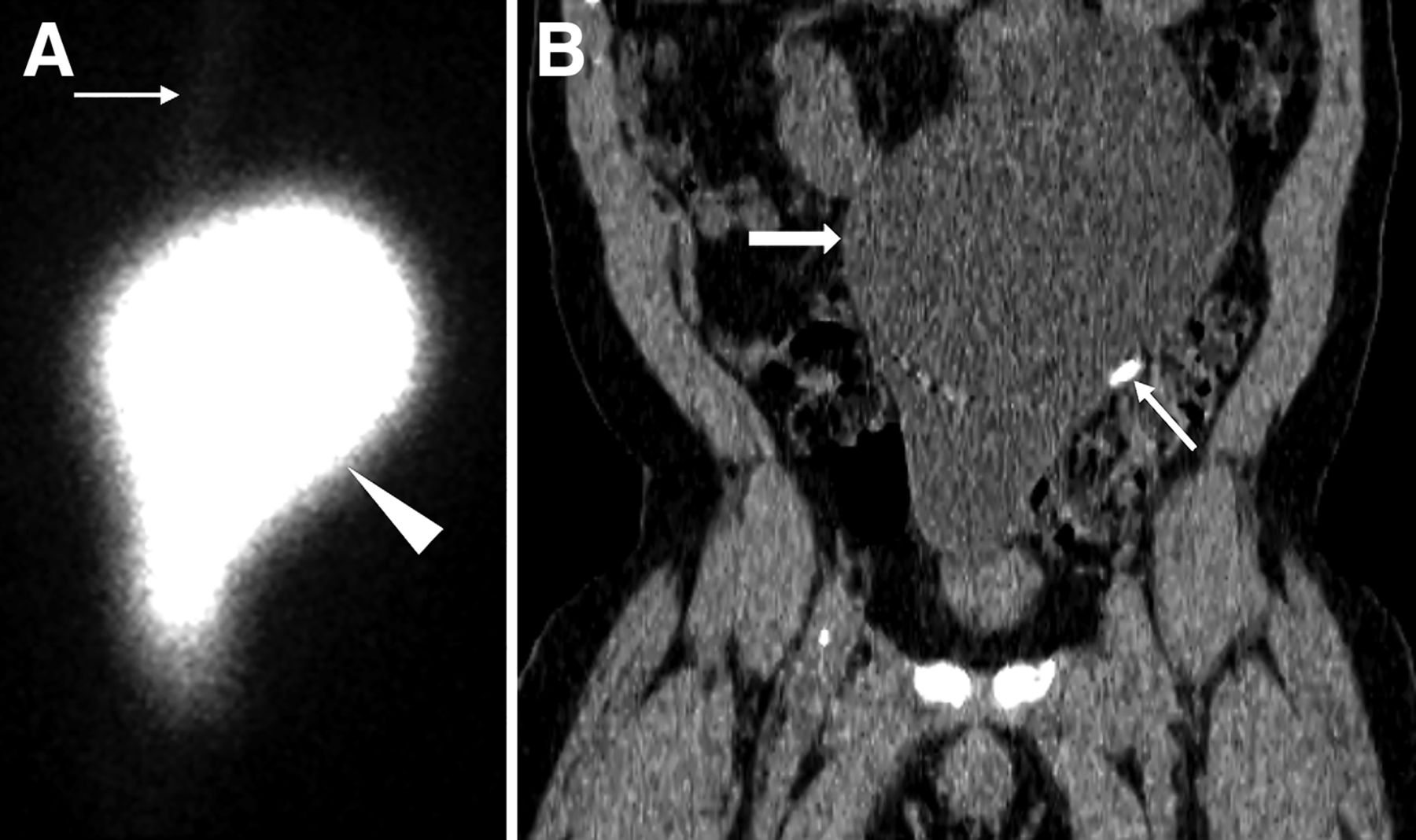
A 41-y-old man with a history of communicating hydrocephalus and ventriculoperitoneal shunt placement 11 y previously presented with headache. Shunt malfunction was suspected. A radionuclide cerebrospinal fluid shuntogram was done after injection of 106.93 MBq (2.89 mCi) of 111In-diethylenetriaminepentaacetic acid into the shunt reservoir on the left scalp. Dynamic images of the head and chest and static image of the abdomen were acquired. Injected activity was noted in the shunt reservoir. Tracer activity in the lateral ventricles suggested patent proximal tubing, and activity along the distal tubing suggested patent distal tubing (Fig. 1). However, there was a large area of well-defined loculated activity in the abdomen (Fig. 2). Further evaluation with SPECT/CT confirmed that the activity in the abdomen correlated with a large pseudocyst occupying the abdomen and pelvis. The distal tip of the shunt was seen within the pseudocyst. Excision of the pseudocyst was planned for the patient.

(A) Coronal CT of head shows hydrocephalus (thin arrow) and left frontal approach ventricular shunt catheter terminating in right ventricle (thick arrow). (B) Planar scintigraphy in anterior projection shows injected activity in shunt reservoir on left scalp (arrowhead). Activity is seen in lateral ventricles (thin arrow) suggestive of patent proximal tubing. Activity is seen tracking through distal tubing along chest and upper abdomen (thick arrow).

{kind=link}
{kind=link}
(A) Planar scintigraphy of abdomen demonstrates well-defined loculated activity in abdomen (arrowhead), as well as part of distal tubing in upper abdomen (arrow). (B) Coronal CT depicts correlating large pseudocyst occupying abdomen and pelvis (thick arrow) with fluid density and thin wall, as well as distal end of shunt catheter tip terminating within pseudocyst (thin arrow).
DISCUSSION
Ventriculoperitoneal shunting is the common treatment for hydrocephalus, with the cerebrospinal fluid being absorbed into the peritoneal cavity. When cerebrospinal fluid is not adequately absorbed, there can be focal peritonitis with inflammatory pseudocyst formation. Other etiologies for pseudocyst include adhesions from previous abdominal surgeries or silicone allergy (1,2). Symptoms include abdominal pain, distension, and constipation. There can be signs of increased intracranial pressure such as headache, nausea, vomiting, and fatigue due to shunt malfunction. Sometimes the pseudocyst can get infected. Ultrasonography is the initial method to diagnose a pseudocyst and can be confirmed with CT. Routine radiography can detect other shunt complications, such as kinking or disconnection. With persisting suspicion, cerebrospinal fluid shunt scintigraphy aids to further assess shunt patency. In our case, the pseudocyst was incidentally detected on the scintigram done to evaluate shunt patency. Excision of the cyst and shunt relocation is the definitive treatment. Percutaneous drainage can be therapeutic and diagnostic.
CONCLUSION
Though ultrasonography is the method of choice for the initial diagnosis, we report initial detection of a large abdominal pseudocyst incidentally on scintigraphy in a patient with a history of ventriculoperitoneal shunt placement and headache. An abdominal pseudocyst has to be suspected, especially if there are abdominal symptoms. Timely diagnosis and management can alleviate the patient’s symptoms.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 12, 2023.
REFERENCES
- 1.
- 2.
- Received for publication May 17, 2023.
- Revision received August 4, 2023.