

Abstract
Indium chloride (111In-Cl3) scintigraphy has been used to evaluate various hematologic diseases for many years. However, there have been few reports on patients with bone marrow reconversion showing high uptake in 111In-Cl3 scintigraphy. Here, we report the case of a 68-y-old man with esophageal cancer who underwent 18F-FDG PET/CT for staging of the disease. In the first lumbar vertebral body, 18F-FDG PET/CT demonstrated high uptake that made it difficult to distinguish bone metastasis from bone marrow reconversion. 111In-Cl3 scintigraphy demonstrated specific findings with high uptake in the lesion, indicating bone marrow hyperplasia or reconversion.
- 111In-Cl3 scintigraphy
- bone marrow reconversion
- chemical shift study
Indium chloride (111In-Cl3) scintigraphy is a useful modality for bone marrow imaging and has been used for evaluating various hematologic diseases for many years. However, there are few reports in which high uptake helped differentiate bone marrow reconversion from bone metastasis.
This report highlights the utility of 111In-Cl3 scintigraphy for differentiating bone marrow reconversion from bone metastasis.
CASE REPORT
A 68-y-old man with esophageal cancer presented to our hospital for further evaluation and surgical resection. Findings on physical examination were normal. Laboratory examination showed anemia (hemoglobin, 9.7 mg/μL) and a high level of blood glucose but was negative for tumor markers.
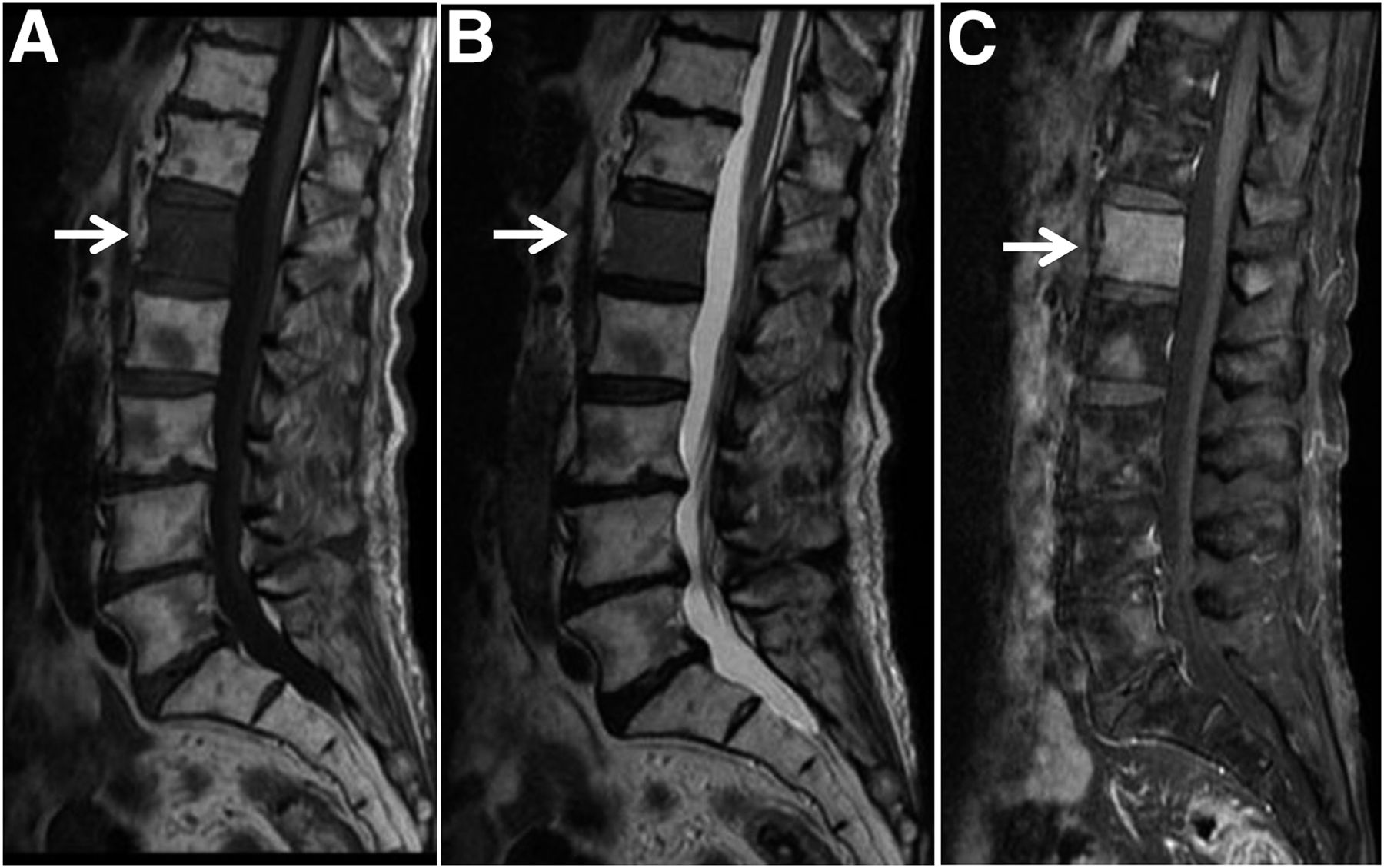
18F-FDG PET/CT showed relatively high uptake (SUVmax, 3.33 for the early phase and 4.46 for the delayed phase) in the first lumbar vertebral body, in addition to slightly high uptake in the primary lesion (chest to lower esophagus). CT showed a slightly sclerotic lesion in the first lumbar vertebral body (Fig. 1). On both T1- and T2-weighted imaging, MRI demonstrated decreased signal intensity, which showed enhancement with gadolinium. MRI also showed several patchy signal changes in the thoracic vertebral bodies (Fig. 2).

18F-FDG PET/CT showing relatively high uptake in L1 vertebral body: anterior maximum-intensity projection (A), fused axial delayed-phase images of primary lesion (B) and L1 vertebral body (C), and sagittal CT image of slightly sclerotic lesion in L1 vertebral body (D).

L1 vertebral body (arrows) showing decreased signal intensity on both T1-weighted (A) and T2-weighted (B) MRI and enhancement with gadolinium (C).
It was difficult to distinguish bone metastasis from bone marrow reconversion; therefore, an MRI chemical shift study and bone marrow scintigraphy (48 h after intravenous injection of 74 MBq of 111In-Cl3) were performed. We used chemical shift imaging to assess for fatty infiltrates, which would suggest bone marrow reconversion. However, no significant decrease in signal was seen on out-of-phase images (Fig. 3). 111In-Cl3 SPECT/CT demonstrated high uptake in the first lumbar vertebral body (Fig. 4).

In-phase (A) and out-of-phase (B) MR images, with the latter showing no significant decrease in signal in L1 vertebral body (arrows).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
111In-Cl3 SPECT/CT showing high uptake (arrowheads) in L1 vertebral body and lower uptake in the primary tumor: scintigraphy (A), fused axial image (B), and fused sagittal image (C). Arrows indicate lower uptake in thoracic vertebral bodies as well as bone marrow reconversion.
The high uptake of 111In-Cl3 was suggestive of bone marrow hyperplasia and not bone marrow metastasis. The patient underwent surgical resection of esophageal cancer, and the first lumbar vertebral lesion showed no changes on a follow-up MRI scan that was acquired 1 y later.
DISCUSSION
In patients with cancer, it is occasionally difficult to differentiate bone marrow reconversion from bone metastasis. There are reports in which localized bone marrow reconversion sometimes mimics malignant tumors, such as bone metastasis in both MRI and 18F-FDG PET/CT (1,2). Several reports have recommended an MRI chemical shift study (3,4). However, no significant findings were seen in the present case. Diffusion-weighted MRI is a potential imaging modality to differentiate malignant from benign lesions. However, studies on this topic have been controversial, and findings should be interpreted in line with routine marrow sequences (3).
After 111In-Cl3 is injected, it binds to transferrin in the same manner as ions and is distributed throughout the bone marrow system. The biologic behaviors of indium and iron are similar, and in many previous reports, bone marrow 111In-Cl3 uptake has been thought to reflect the distribution of erythropoietic marrow. 111In-Cl3 has been clinically used for bone marrow studies. Approximately 30% of the administered tracer is found in the bone marrow, 20% in the liver, 7% in the kidneys, and 1% in the spleen (5).
111In is a cyclotron-produced isotope with a half-life of 2.8 d emitting γ-rays with energies of 171 keV (89%) and 245 keV (94%). It decays by electron capture to stable 111Cd (5). In comparison with the 99mTc-labeled colloids, the specificity to bone marrow accumulation is thought to be higher, but radiation exposure is also higher because of relatively long half-life.
111In-Cl3 may accumulate in tumors (6). However, to our knowledge, there has been no report concerning bone metastasis in a patient with esophageal adenocarcinoma taking up 111In-Cl3.
CONCLUSION
111In-Cl3 scintigraphy in the present case demonstrated high uptake in the lesion and was effective for differentiating between bone marrow reconversion and bone metastasis from esophageal adenocarcinoma.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 10, 2017.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- Received for publication July 26, 2017.
- Accepted for publication October 12, 2017.