


Abstract
Neuroendocrine tumors (NETs) may manifest as large masses in the abdominopelvic region that exhibit mobility and shifting, potentially leading to diagnostic uncertainty both before and after treatment. A meticulous analysis of PET/CT scans is advantageous in accurately identifying the precise location of large abdominopelvic masses. Tumor heterogeneity may be present in NETs with large abdominopelvic masses and may be easily identified on dual-tracer (68Ga-DOTATATE and 18F-FDG) PET/CT scans. In this scenario, the combined use of chemotherapy and peptide receptor radionuclide therapy is a more effective treatment option than monotherapy. Here, we present a case of a NET with wandering, large, heterogeneous masses in the abdominopelvic regions that were identified using dual-tracer PET/CT. After the administration of temozolomide chemotherapy in a combined chemotherapy–peptide receptor radionuclide therapy approach, we observed an upregulation in the expression of somatostatin receptor in the abdominopelvic masses.
- neuroendocrine tumor
- 68Ga-DOTATATE
- 18F-FDG
- PET/CT
- somatostatin receptor
- peptide receptor radionuclide therapy
Neuroendocrine tumors (NETs) are commonly observed in gastroenteropancreatic systems. Imaging investigations include CT, 68Ga-DOTATATE/DOTANOC/DOTATOC PET, MRI, and 18F-FDG PET. Management of NET patients includes surgery, somatostatin analog therapy, peptide receptor radionuclide therapy (PRRT), and chemotherapy (1,2).
We report a case of NET with large abdominopelvic masses that underwent a change in location during 68Ga-DOTATATE PET/CT and 18F-FDG PET/CT acquisitions. The tumor was heterogeneous and demonstrated a reduction in size and 18F-FDG avidity and an increase in somatostatin receptor (SSTR) expression after a combined chemotherapy–PRRT approach.
CASE REPORT
A 38-y-old woman presented with an initial complaint of abdominal pain. Ultrasonography of the abdomen showed bilateral adnexal masses with hypoechoic liver lesions. A biopsy sample from the pelvic masses showed metastatic grade II NET (Ki-67 index, 10%–12%). 68Ga-DOTATATE PET/CT showed 2 SSTR-expressing heterogeneously enhancing lobulated abdominopelvic masses (one mass on the right side, with intense SSTR expression, and the other mass on the left side, with low-grade SSTR expression; the right mass was relatively cranial to the left mass). Four days later, the patient underwent 18F-FDG PET/CT, which revealed intense 18F-FDG uptake in the masses. However, the mass on the right had moved downward toward the pelvis, whereas the mass on the left had moved upward toward the abdomen. This finding initially produced the sense that the left mass had disappeared and the right mass had appeared in a different location. The patient received 177Lu-DOTATATE combined with capecitabine and temozolomide as sandwiched chemotherapy and PRRT.
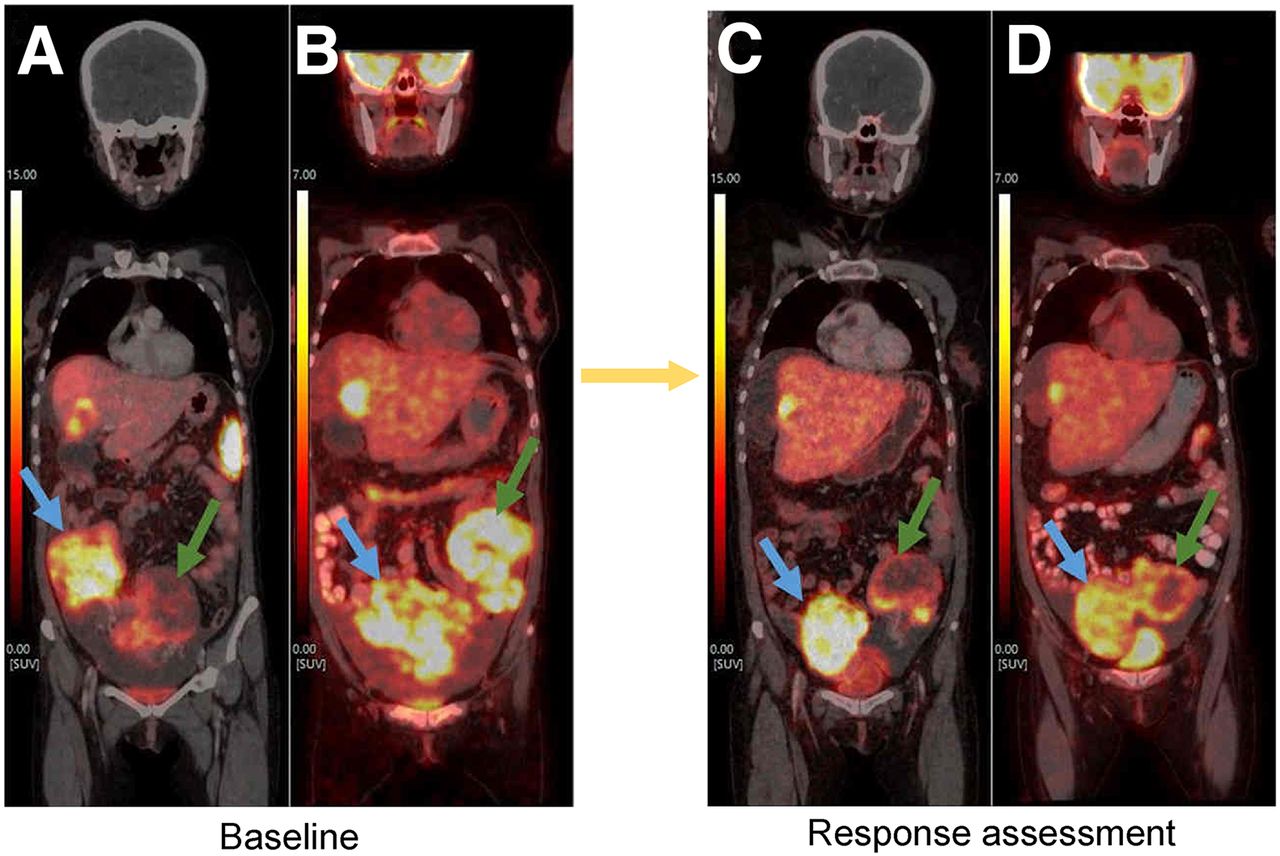
For both abdominopelvic masses, follow-up scans showed an increase in SSTR uptake (baseline SUVmax, 20.7 for right mass and 13.6 for left mass; follow-up SUVmax, 22.1 for right mass and 15.3 for left mass) and a reduction in 18F-FDG uptake (baseline SUVmax, 15.3 for right mass and 17.0 for left mass; follow-up SUVmax, 9.8 for right mass and 6.39 for left mass) (Fig. 1). The follow-up scans also showed a reduction in size (right abdominal mass, 8.1 × 6.1 cm at follow-up vs. 8.3 × 11.8 cm at baseline; left abdominal mass, 7.0 × 8.3 cm at follow-up vs. 7.4 × 8.5 cm at baseline) and an increase in necrosis, which suggest a favorable response to the sandwiched chemotherapy and PRRT (Fig. 2).

(A) Baseline maximum-intensity projection of 68Ga-DOTATATE PET/CT showing 2 abdominopelvic masses. (B) Baseline maximum-intensity projection of 18F-FDG PET/CT showing 18F-FDG–avid abdominopelvic masses. Between these scans, mass on right moved downward toward pelvis, whereas mass on left moved upward toward abdomen—suggestive of wandering masses. (C) Post–177Lu-DOTATATE therapy scintigraphy on gamma camera scan showing good concentration of tracer in abdominopelvic masses. (D and E) Maximum-intensity projections of 68Ga-DOTATATE PET/CT (D) and 18F-FDG PET/CT (E) at response assessment showing reduction in 18F-FDG uptake and increase in SSTR expression in abdominopelvic masses. Blue arrows indicate right masses; green arrows indicate left masses; yellow arrows indicate given combined chemotherapy–PRRT.

Coronal views of 68Ga-DOTATATE (A and C) and 18F-FDG (B and D) PET/CT at baseline (A and B) and at response assessment (C and D) showing reduction in size and 18F-FDG uptake and increase in SSTR expression in abdominopelvic masses—suggestive of favorable response to combined chemotherapy and PRRT. Blue arrows indicate right masses; green arrows indicate left masses; yellow arrow indicates given combined chemotherapy–PRRT.
DISCUSSION
In NETs, there have been only a few reported cases of mesenteric masses in the literature; these cases are typically associated with high-grade tumors and are primarily in the small intestine (3).
In our patient, we observed that the location of the abdominopelvic masses on the PET/CT scans had shifted, giving the impression that the left mass had vanished while the right mass had appeared in a different location, indicating that these masses were highly mobile and wandering. In the literature, only a handful of instances of mobile, wandering abdominopelvic masses have been documented. These include mesenteric pseudocysts, mantle cell lymphoma masses, and gastrointestinal stromal tumors of the jejunum. The reason for the mobility of these masses is their attachment to the intestinal mesentery, which is inherently elongated and permits them to move to some extent (4).
Our patient received combined chemotherapy and PRRT, with 2 cycles of capecitabine and temozolamide sandwiched between 2 cycles of 177Lu-DOTATATE PRRT (5). Follow-up response evaluation scans revealed that the abdominopelvic masses had decreased in size and 18F-FDG uptake but increased in SSTR expression. Preclinical studies (6) have shown that temozolamide increases SSTR-2 expression in NET. A similar result was observed in our study, as may be attributable to upregulation of messenger RNA associated with increased SSTR-2 expression after temozolamide administration (6).
CONCLUSION
Large abdominopelvic masses that are mobile and wandering may be observed in NETs. Such a finding may cause confusion during the initial evaluation before therapy and during the follow-up evaluation after therapy. Therefore, careful examination of PET/CT scans with the utmost care is beneficial when determining the location of huge abdominopelvic masses. Dual-tracer 68Ga-DOTATATE and 18F-FDG PET/CT scans can readily detect tumor NET heterogeneity with large abdominopelvic masses. In this situation, combined chemotherapy and PRRT would be a more effective treatment option than monotherapy, as the upregulation of SSTR expression caused by temozolamide chemotherapy will be mitigated through PRRT.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 12, 2024.
REFERENCES
- Received for publication December 16, 2023.
- Revision received January 30, 2024.





{kind=link}
{kind=link}