


Abstract
SUV normalized by total body weight is affected by the amount of body fat. The SUV of normal tissues and lesions is higher (overestimated) in obese patients than in patients with a normal body mass index (BMI). SUL (SUV normalized by lean body mass [LBM]) is recommended for more accurate SUV results. Given the importance of a quantitative PET parameter, particularly when comparing PET studies, we aimed to revisit the effect of obesity on SUV, measuring SUL in normal-BMI patients and obese patients and testing the effect of the amount of LBM. Methods: 18F-FDG whole-body images of adult patients were analyzed retrospectively. We measured both SUVmax and SUVmean in the blood pool and liver of patients with a normal BMI (18.5–24.9) and a high BMI (≥30) (obese). In all patients, we calculated LBM via an equation using patient height and weight and corrected all SUVs to SULs. Mean (±SD) SUVs and SULs were compared under various circumstances. Scatterplots were generated for weight and SUV–SUL differences. Results: SUVmean in the liver and blood pool was significantly higher in obese patients (30 patients) than in patients with a normal BMI (20 patients) (4.1 ± 0.7 and 3.0 ± 0.5, respectively, in liver, vs. 3.2 ± 0.6 and 2.4 ± 0.4, respectively, in blood pool; P < 0.001). SULmean was significantly lower in both liver and blood pool in all patients, being approximately 75% of SUVmean in patients with a normal BMI and 55% of SUVmean in obese patients (P < 0.001). SULmean in the liver and blood pool did not significantly differ between obese patients and normal-BMI patients (P > 0.05). The SUV–SUL difference was significantly higher in obese patients than in patients with a normal BMI (P < 0.001). These statistical results were the same when SUVmax and SULmax were compared. Conclusion: SUV overestimates metabolic activity in all patients, and this overestimation is more significant in obese patients than in patients with a normal BMI. SUL is not affected by body weight or the amount of LBM.
SUV is a commonly used PET parameter to measure the uptake of various radiopharmaceuticals, mainly 18F-FDG, in normal tissues and lesions (1–3). SUV is simply the ratio of activity concentration in the target tissue or lesion to activity concentration in the whole body:
This equation assumes that injected activity is uniformly distributed in the whole body and that 1 cm3 of tissue weighs 1 g (4). Activity in the lesion or target tissue is decay-corrected.
In routine, many hospitals still use the patient’s weight to normalize SUV, although it is known that SUV is overestimated in obese patients (5–7). This consideration is particularly important when one is comparing the new and old PET studies of a patient whose weight has significantly changed or of a child who has significantly grown between studies. Obese patients have a high amount of body fat. 18F-FDG accumulation in white fat is very low in the fasting state, and PET studies are obtained in the fasting state (8). On the other hand, a significant accumulation of 18F-FDG is seen in brown fat, mostly in children and underweight adults, particularly women, and in cold temperatures (9,10). White fat contributes a significant amount to total body weight. Among young women (20–39 y old), fat makes up 20%–25% of the total body weight in those with a normal body mass index (BMI) (18.5–24.9), 32%–35% in those with a BMI of 25–29.9 (overweight), and 38%–40% in those with a BMI of 30 or higher (obese) (11). These values are lower in men (11). The mean concentration of activity in the patient’s body (MBq/kg or MBq/L) decreases with increasing body weight, causing erroneously higher SUVs in obese patients.
As an alternative to SUV (normalized by total body weight), SUL has been recommended (SUV normalized by lean body mass [LBM]), because 18F-FDG accumulation in fat is minimal and the percentage of fat is high in obese people (5). There are various ways of measuring LBM. It is generally calculated through predictive equations using height and body weight (12). Semidirect measurements of LBM such as bioelectric impedance analysis, dual-energy x-ray absorptiometry, CT, and MRI can provide more accurate results (13). Using the most accurate method to measure LBM will provide a more accurate SUL. A standard formula for calculating LBM will allow more accurate comparison of PET studies.
Although SUL is highly recommended instead of SUV to calculate the metabolic activity of lesions and tissues, particularly in obese patients, SUV is still commonly used. Given the importance of a quantitative PET parameter, particularly when comparing PET studies, we aimed to revisit the effect of body fat on SUV, to measure SUL not only in obese patients but also in patients with a normal BMI, and to test the effect of the amount of LBM on SUL.
MATERIALS AND METHODS
In this retrospective study, whole-body 18F-FDG/CT images of adult patients were selected for further analysis. The study was approved by the ethics committee of the Kuwait Ministry of Health, and the requirement for informed consent was waived.
The 18F-FDG PET/CT images were obtained at Mubarak Al-Kabeer Hospital, mainly for oncology patients, on a Gemini time-of-flight PET/CT camera (Philips). The images were acquired 60 min after intravenous injection of 222 MBq (6 mCi) of 18F-FDG for a 70-kg patient (3.17 MBq/kg). Blood glucose levels were measured using a glucometer before the 18F-FDG was injected; at our institute we usually do not injected 18F-FDG unless the blood glucose is no higher than 150 mg/dL. A low-dose CT scan was first obtained for attenuation correction and anatomic localization. Afterward, the PET acquisition took place at a speed of 2–3 min per bed position from the top of the head to the mid thighs or toes. PET images were corrected for attenuation on the basis of the CT data, were reconstructed using a standard iterative algorithm, and were reformatted into transaxial, coronal, and sagittal views. Maximum-intensity projections were also generated. Both attenuation-corrected and uncorrected PET images were reviewed, as well as PET/CT fusion images.
We recorded each patient’s weight, height, and net injected activity (18F-FDG dose before injection minus residual activity in the syringe after injection).
We measured SUVmax and SUVmean in the normal liver and blood pool in patients with a normal BMI (18.5–24.9) and a high BMI (≥30). SUVmean more accurately estimates activity in the blood pool and liver; however, because SUVmax is used to assess the lesions, we also measured SUVmax in the blood pool and liver to see if any results differed when SUVmax and SUVmean were corrected to SULmax and SULmean. A 1 cm2 spheric region of interest was placed over the right hepatic lobe in a normal-appearing area, and a 1 cm2 spheric region of interest was placed over the blood pool in the left or right atrium, excluding the atrial wall. If there was activity in the atrial wall, we used the ventricular cavity.
We determined LBM via an online calculator by entering the patient height and weight, and we then calculated the SUL for each SUV (12).
Data management and statistical analysis were performed using SPSS software (version 25.0; IBM Corp.). Mean (±SD) was calculated for the blood-pool and liver SUVmax, SUVmean, SULmax, and SULmean; the injected doses; and the LBMs. To compare the values in 2 patient groups (patients with a normal BMI and obese patients), 2-sample t testing was used if the data showed normality according to the Shapiro–Wilk test; otherwise, the nonparametric Mann–Whitney U test was used. To compare the values in the same patient group, a paired t test was conducted if the mean of differences were normally distributed; otherwise, the Wilcoxon signed-rank test on the differences was used. All tests were 2-tailed, and a P value of less than 0.05 was considered statistically significant. Scatterplots were also generated for weight and SUV–SUL differences. We used Spearman rank correlation to quantify the strength of relationships between weight and SUV–SUL differences.
RESULTS
We evaluated the 18F-FDG PET/CT whole-body images of 50 patients: 20 with a normal BMI (mean age, 61.3 y; range, 43–74 y; 6 women and 14 men) and 30 with a high BMI (obese) (mean age, 61.7 y; range, 30–77 y; 19 women and 11 men). The injected 18F-FDG activity was 223.4 ± 28.1 MBq (∼6 mCi) in patients with a normal BMI and 299.9 ± 23.3 MBq (∼8 mCi) in obese patients. The SUVmax, SUVmean, SULmax, and SULmean of the blood pool and liver are shown in Figures 1 and 2.

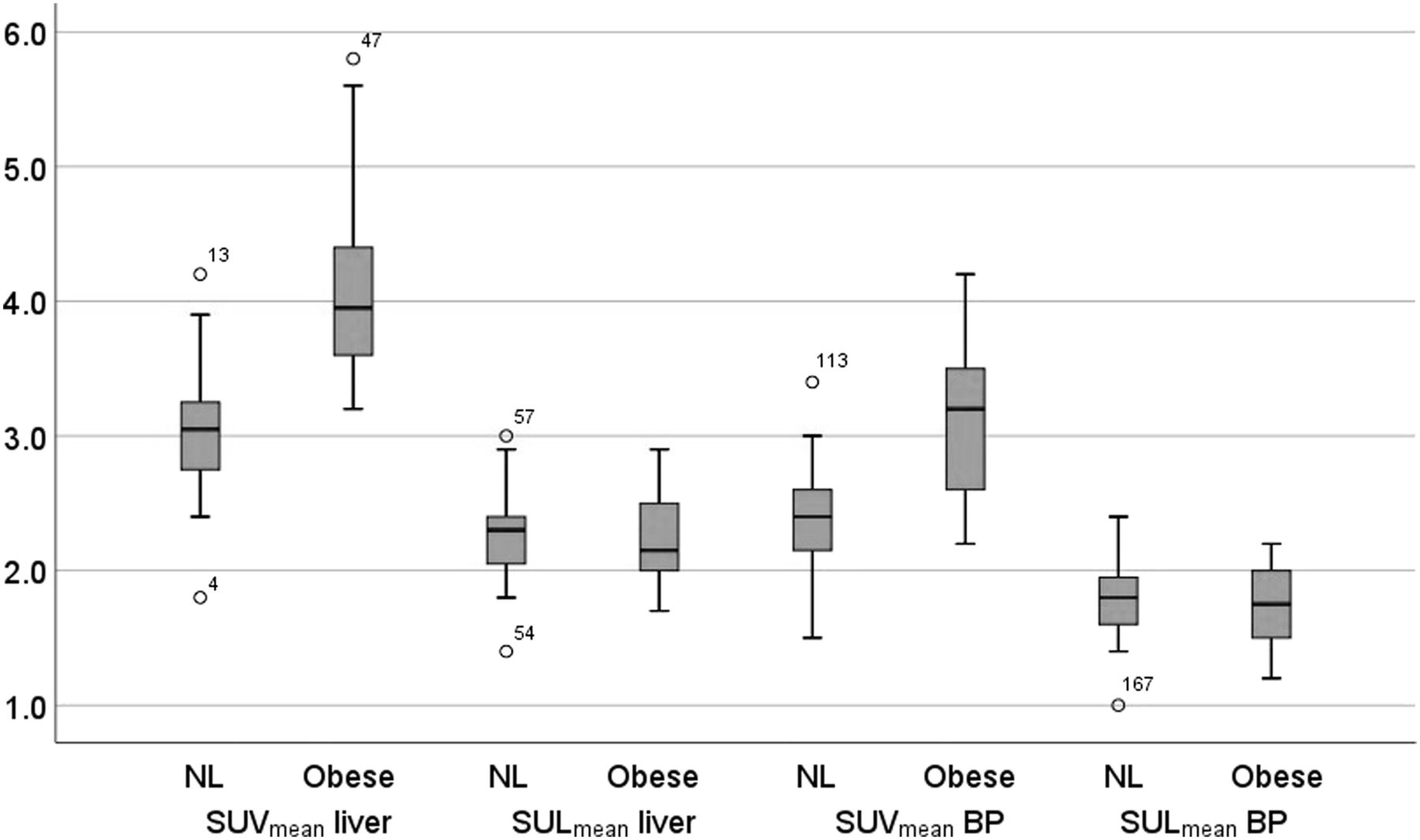
Mean ± SD SUVmean and SULmean of liver and blood pool in patients with normal BMI and obese patients. BP = blood pool; NL = normal BMI.
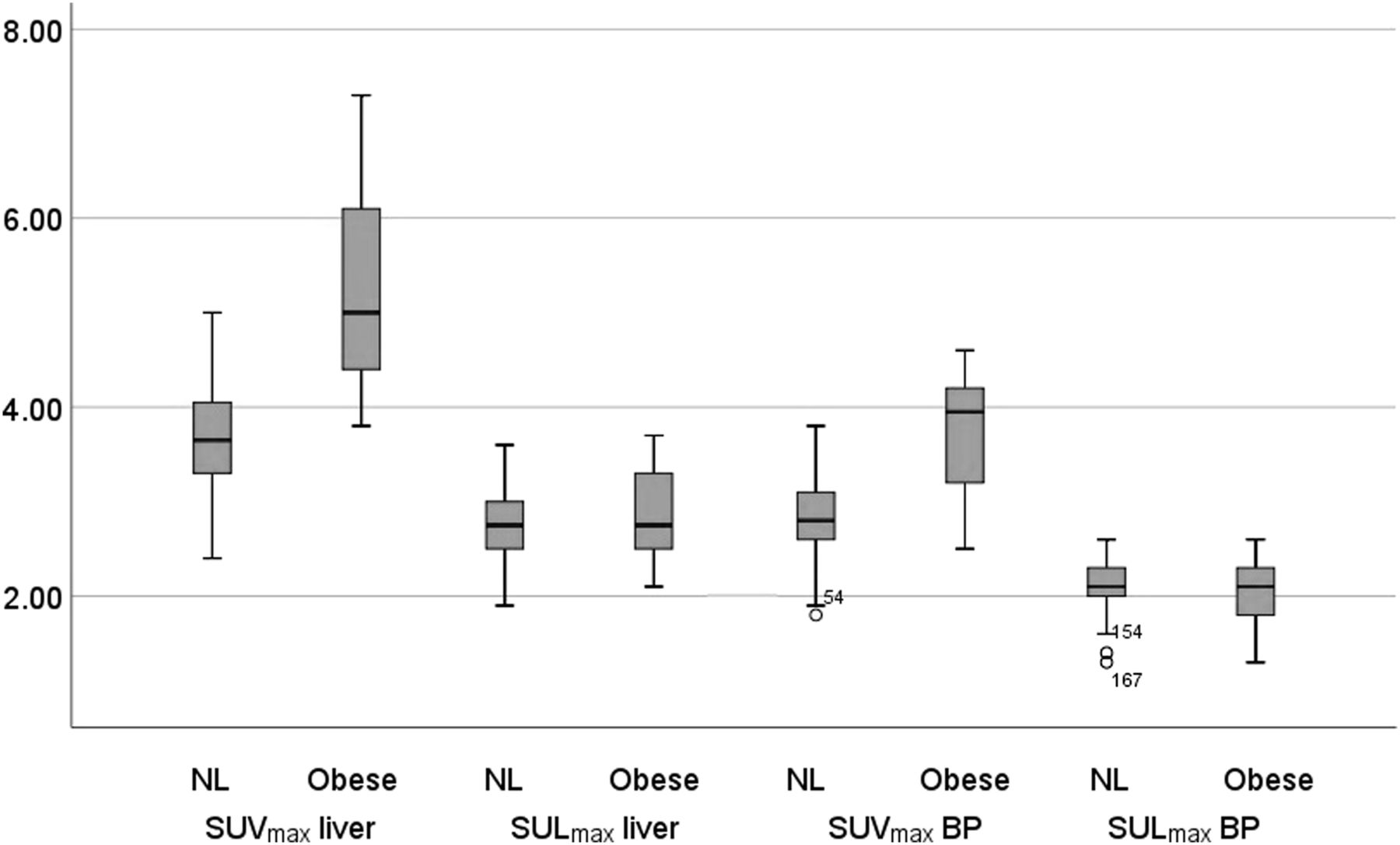
Mean ± SD SUVmax and SULmax of liver and blood pool in patients with normal BMI and obese patients. BP = blood pool; NL = normal BMI.
SUVmean and SUVmax in the liver and blood pool were significantly higher in obese patients than in normal-BMI patients (P < 0.001); SUVmean was 33%–36% higher, and SUVmax was 36%–41% higher.
SULmean and SULmax in liver and blood pool were significantly lower than SUVmean and SUVmax in all patients. SULs were approximately 75% of SUVs in patients with a normal BMI and 55% of SUVs in obese patients (P < 0.001). These comparisons show that SUVs were overestimated in all patients (both normal-BMI and high-BMI patients), but more so in obese patients.
SULmean and SULmax in liver and blood pool did not significantly differ between obese patients and normal-BMI patients (P > 0.05).
When comparing obese patients with different amount of LBM (50.3 ± 1.7 kg vs. 59.1 ± 2.8 kg, 10 patients in each subgroup), we found that SULs did not significantly differ (P > 0.05) (Table 1).
SULmax and SULmean in Obese Patients with Different Amounts of LBM
The differences between liver and blood-pool SUV and SUL (SUV minus SUL) were significantly higher in obese patients than in normal-BMI patients (P < 0.001) (Fig. 3). Scatterplots of the relationship between weight and SUV–SUL differences are seen in Figure 4; there is clearly a positive linear relationship. The correlations between SUV–SUL differences and weight for liver SUVmean, liver SUVmax, blood-pool SUVmean, and blood-pool SUVmax were 0.727, 0.766, 0.673, and 0.729, respectively, and all were significant (P < 0.001).
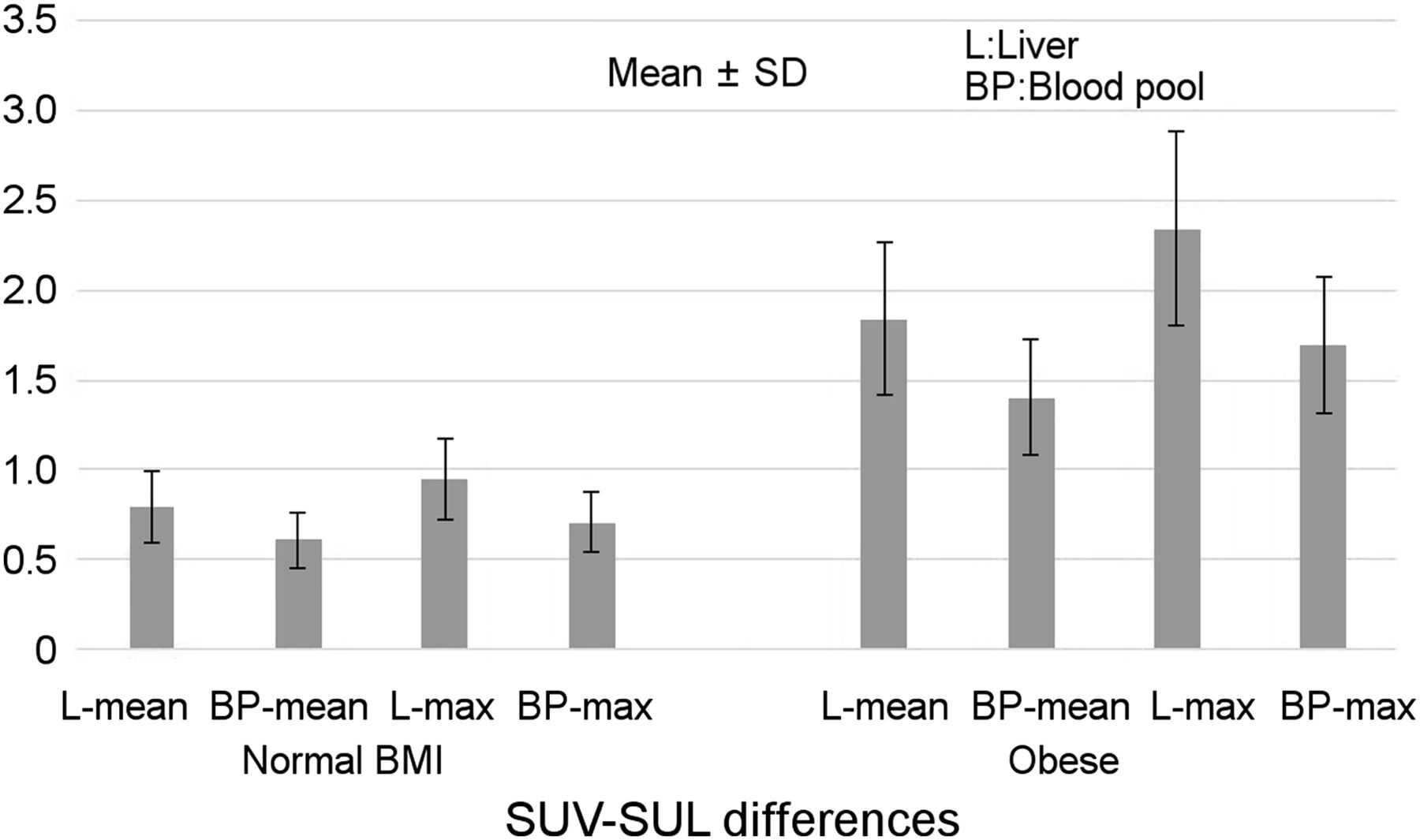
Mean ± SD SUV–SUL differences (mean and maximum) in liver and blood pool in patients with normal BMI and obese patients.
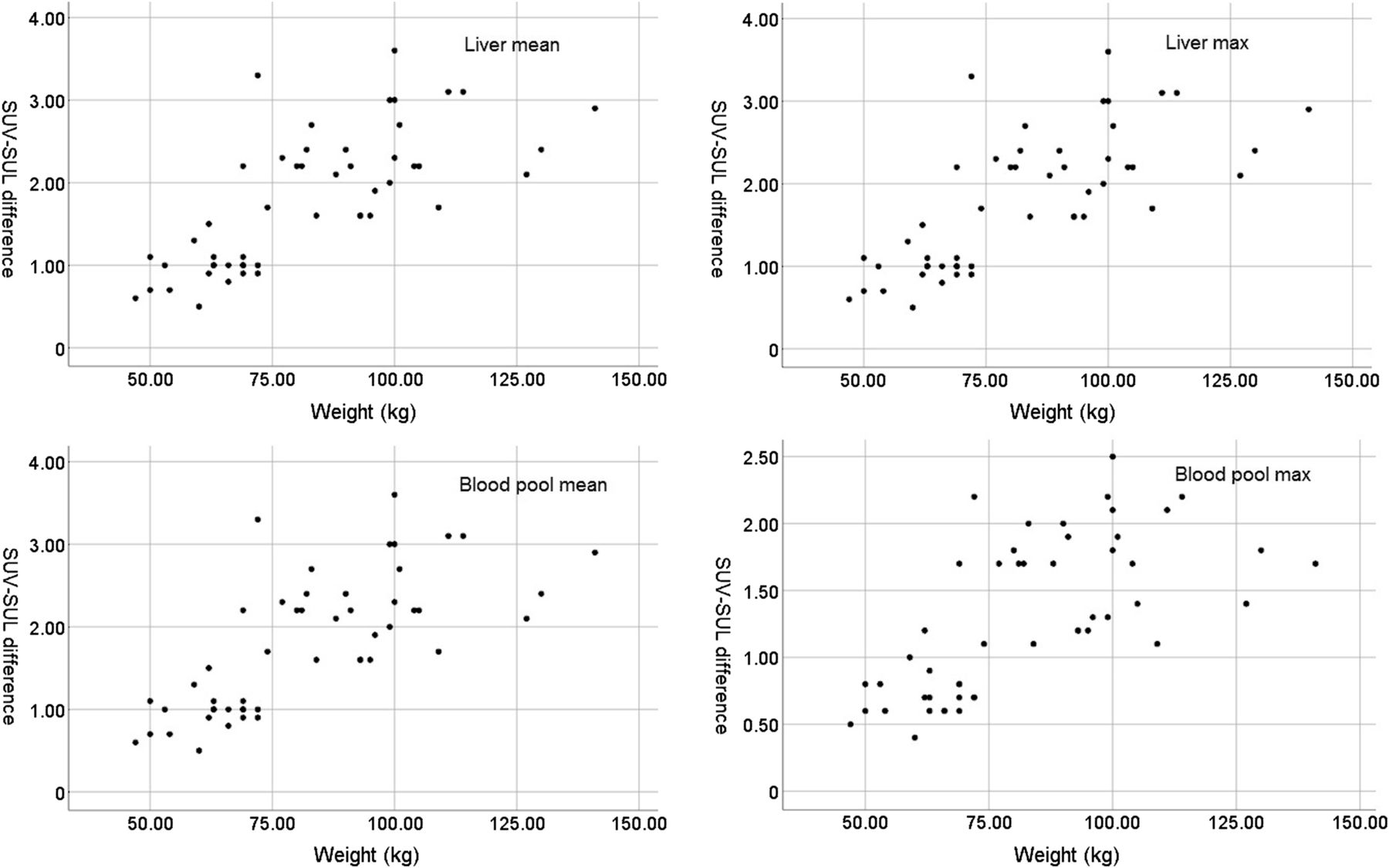
Scatterplots of weight and SUV–SUL differences.
DISCUSSION
Visual assessment of PET images for areas of abnormal uptake is adequate and accurate. However, a quantitative or semiquantitative method can better assess such parameters as metabolic activity, perfusion, or the receptor density of lesions and tissues, depending on the PET study. Such assessments are important to estimate the grade of malignancy, to calculate the dose of therapeutic agents, and to compare posttreatment studies with pretreatment studies (14–16).
SUV is the most commonly used PET parameter to assess uptake of various radiopharmaceuticals in lesions and normal tissues. SUV generally accurately estimates the degree of uptake in lesions and normal tissues but is affected by various patient, biologic, and technical factors that can cause over- or underestimation of activity. 18F-FDG uptake can be affected by many factors, such as suboptimal patient preparation; high blood glucose and insulin levels; the presence of diabetes; the patient’s BMI, age, and sex; the imaging start time after radiotracer injection; significant extravasation of activity; the image acquisition and reconstruction parameters; conditions during the postinjection uptake period; inaccurate entry of patient weight, height, and injected activity into the computer; the effect of CT contrast material on attenuation-corrected PET images; patient and organ motion; the presence of other diseases; and the effects of medications (17–22).
In overweight people, SUV is usually overestimated in lesions and normal tissues (5,6). SUL more accurately estimates radiopharmaceutical uptake and compares PET studies. Zasadny et al. reported that in heavy patients, the SUVs of blood, liver, and spleen were up to twice those in lighter patients (5). SUL provided lower values than SUV in their study. In our obese patients, the SUVs of blood pool and liver were also significantly higher than expected normal values. SUVmean was 33%–36% higher and SUVmax 36%–41% higher in obese patients than in patients with a normal BMI. As expected, SULs were lower than SUVs in all patients, even more so in obese patients. SULs were approximately 50% of SUVs in obese patients and 75% of SUVs in patients with a normal BMI.
The SULs of liver and blood pool did not significantly differ between obese patients and patients with a normal body BMI or between obese patients with higher and lower amounts of LBM. This finding shows that SUL is not affected by weight or amount of LBM. LBM can change over time within the same patient if there is a change in tissue composition, such as a gain in muscle. Figure 5 illustrates this principle.
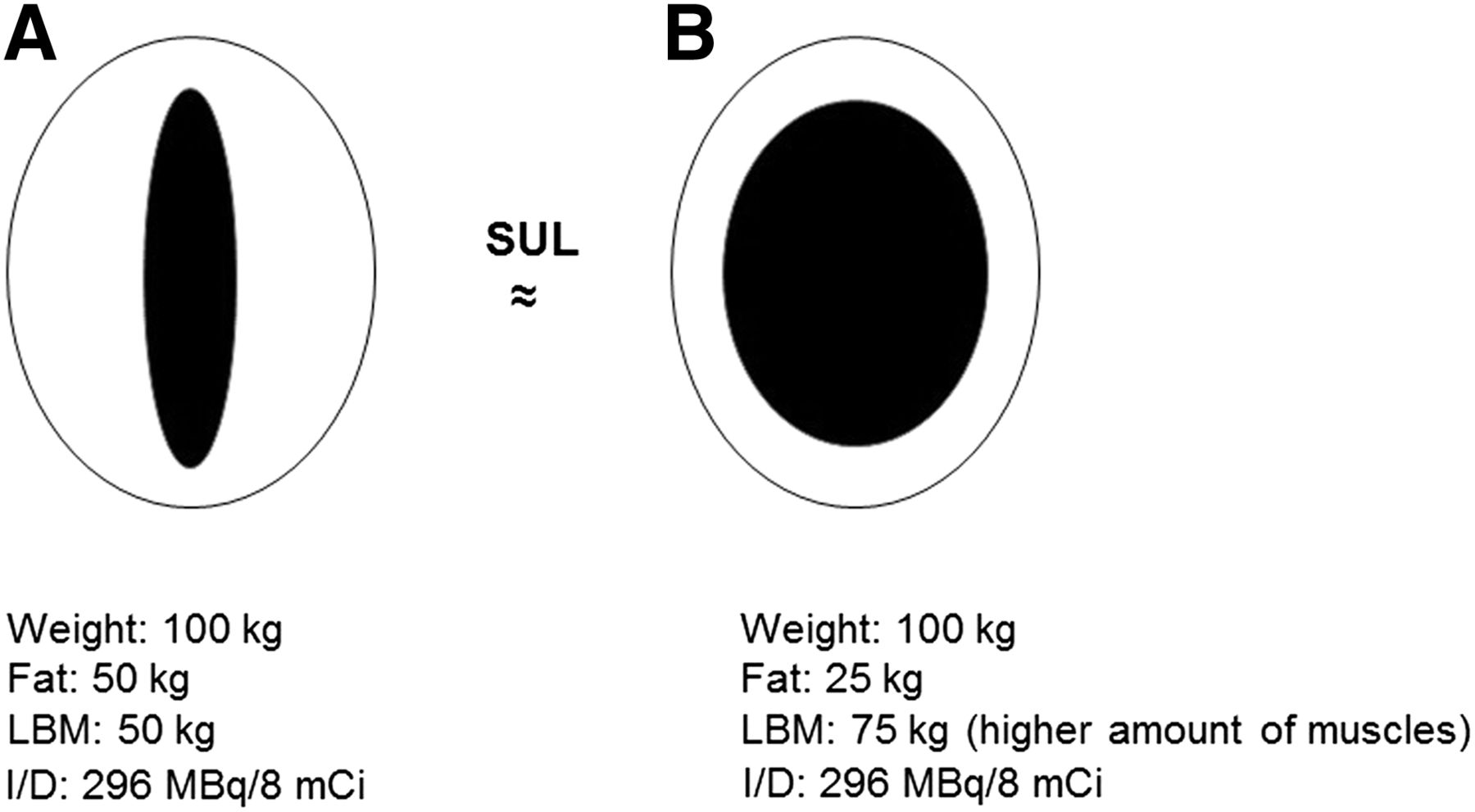
Principle of patient who, at different times, had same body weight but different LBMs and was injected with same 18F-FDG activity per body weight. In A, patient has more fat; in B, patient has more muscle. LBM activity (injected dose/LBM) is higher in A than in B, but target-area activity (kBq/mL) is also higher in A (because of smaller LBM volume in A and more available activity for target area). LBM activity is lower in B than in A, but target-area activity is also lower in B (because of higher volume of LBM and competitive reduction in target-area uptake caused by uptake in muscle). Both sides of SUL equation are higher in A and lower in B; as a result, SULs of target in A and B do not significantly differ. I/D = injected dose.
Simply calculating the patient’s LBM and using it to normalize the SUV will provide more accurate results than normalizing SUV by total body weight. For accurate comparison of PET studies, LBM should be calculated using a standardized method. However, in patients with a high amount of brown fat, SUL may be underestimated because brown fat takes up a significant amount of activity, causing competitive reduction of uptake in target tissues. On the other hand, if the brown fat is in an underweight patient, there may not be a significant difference between SUV and SUL because total weight will not significantly differ from LBM. Studies assessing SUV in children found that their liver and tumor SUVs were lower than those in adults (23,24) and that SULs were also lower than normal adult values (24). These studies recommended using body surface area–based calculation of SUV in pediatric patients (23,24). The lower SUVs and SULs in children could be due to their higher amount of brown fat, which could competitively reduce uptake in lesions and in other normal tissues.
Using SUL in all patients—whether they have a normal BMI or a high BMI—can provide more accurate results for comparison of PET studies in adults. However, currently, SUL can be used only in overweight and obese patients, not in patients with a normal BMI, because the current standard values (an SUV threshold of 2.5 for differentiating benign from malignant lesions, and reference SUVs for liver, blood pool, and other tissues) have been calculated from patients with a normal BMI or from mixtures of patients with various BMIs. If SUL is going to be used in routine practice, the standard values should be determined in large numbers of people with standard BMI.
The main limitation of this study may be its relatively small number of patients, but the number was enough to achieve an approximate assessment of various effects on SUVs and SULs. Another limitation is that we measured LBM using a predictive equation, but again, this method was acceptable for an approximate assessment of LBM. However, measurement by a more accurate method will provide more accurate results than measurement by a formula using weight and height (e.g., two patients of the same weight and height may have different amounts of fat and muscle and thus different LBMs).
CONCLUSION
SUV overestimates metabolic activity in all patients, and this overestimation is more significant in obese patients than in patients with a normal BMI. SUL is not affected by body weight or by the amount of LBM.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 11, 2019.
REFERENCES
- Received for publication July 4, 2019.
- Accepted for publication September 6, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}