


Visual Abstract

Abstract
The goal of this work was to determine U.S. diagnostic reference levels (DRLs) and achievable administered activities (AAAs) for adult renal scintigraphy. Methods: Under an Institutional Review Board–approved protocol, data were collected from the Intersocietal Accreditation Commission during one 3-y accreditation cycle encompassing 110 facilities. Elements included radiopharmaceutical, administered activity, practice type, and examination volume. DRLs and AAAs were calculated and compared with non-U.S. values and societal recommendations as available. Results: Ninety-three facilities provided data on 99mTc-mercaptoacetyltriglycine (99mTc-MAG3), and 15 provided data on 99mTc-diethylenetriaminepentaacetic acid (99mTc-DTPA) for adult renal scintigraphy exams. Analysis demonstrated a DRL of 392.2 MBq (10.6 mCi) for 99mTc-MAG3 and 531.7 MBq (14.4 mCi) for 99mTc-DTPA, with an AAA of 370 MBq (10 mCi) for 99mTc-MAG3 and 445.9 MBq (12.1 mCi) for 99mTc-DTPA. Conclusion: The resultant calculated novel U.S. DRLs and AAAs may serve as benchmarks that nuclear medicine facilities may use to refine renal scintigraphy protocols, reduce patient doses, and potentially guide future societal guideline recommendations.
Given the potential for radiation-induced cancers and other health issues, it is the responsibility of imaging providers to tailor exams using ionizing radiation such that a diagnostic study is achieved with the lowest amount of radiation dose imparted to the patient. In nuclear medicine, the radiation dose is proportional to the administered radiopharmaceutical activity, and hence it is essential that the minimum activity needed for acceptable diagnostic quality be used.
Two metrics that have been identified to aid in this effort are the diagnostic reference level (DRL) and the achievable administered activity (AAA). The DRL, as defined by the International Commission on Radiological Protection (ICRP), is the 75th percentile of dose associated with a diagnostic imaging study, whereas the AAA is defined as the 50th percentile (median) (1). In the field of nuclear medicine and molecular imaging, given the relationship between radiation exposure and the administered activity of the specific radiopharmaceuticals, these values are expressed in megabecquerels (MBq) or millicuries (mCi). The percentiles, and hence the underlying activities, are derived by surveying imaging facilities using various standard techniques and technologies.
Three surveys to date have identified the DRLs and AAAs for many U.S. nuclear medicine examinations, including myocardial perfusion imaging, planar and SPECT bone scintigraphy, hepatobiliary scintigraphy, lung perfusion scintigraphy, 123I and 131I thyroid exams, brain and whole-body 18F-FDG PET/CT, and 18F-amyloid brain PET/CT (2–4). One of the less common nuclear medicine procedures, renal scintigraphy, can impart a moderate dose of 2.59 mSv when administering the standard adult radioactivity but does not have the benefit of well-established DRLs and AAAs. The only prior U.S. data were derived from a small survey with only 9 respondents and were limited to 99mTc-mercaptoacetyltriglycine (99mTc-MAG3); no data pertaining to 99mTc-diethylenetriaminepentaacetic acid (99mTc-DTPA) were gathered (5). The aim of this study was to accurately determine these values (based on accreditation surveys) for adult renal scintigraphy at U.S. nuclear medicine facilities and add them to the growing body of nuclear medicine reference levels so that facilities may use them to optimize protocols and potentially guide future societal guideline recommendations.
MATERIALS AND METHODS
Under an Institutional Review Board–approved protocol with the requirement to obtain informed consent waived, deidentified data regarding administered activities for adult renal scintigraphy were collected from the Intersocietal Accreditation Commission nuclear medicine accreditation program during one 3-y accreditation cycle from October 2015 through December 2018. The accreditation process requires nuclear laboratories to submit demographic and practice data. For each area for which the facility is seeking accreditation (e.g., lung, hepatobiliary, brain scintigraphy; oncologic PET/CT), the facility submits 2 example examinations along with information on the radiopharmaceutical used, the administered activities, the final reports, and the standard operating procedure or protocol. For genitourinary nuclear medicine accreditation, the facility may choose to submit material from adult or pediatric examinations, and these may include any combination of diuretic renography, angiotensin-converting enzyme inhibitor renography, or renal cortical imaging exams. The cycle included 110 facilities applying for genitourinary nuclear medicine scintigraphy accreditation. Two provided information on only pediatric renal scintigraphy, and thus information from 108 sites was included in the final dataset. Facility demographics showed most sites to be hospital-based (n = 74), and approximately one third were outpatient imaging centers (n = 34) with a wide range in volume for both general nuclear medicine studies and genitourinary scintigraphy studies (Table 1).
Practice Characteristics of 108 Facilities Included in Intersocietal Accreditation Commission Accreditation Survey Period of October 2015 to December 2018
RESULTS
Most facilities used 99mTc-MAG3–based protocols; a small minority used 99mTc-DTPA, and a few used both. This resulted in 99mTc-MAG3 dose data being provided by 93 facilities and 99mTc-DTPA dose data by 15 facilities, with 182 99mTc-MAG3 and 24 99mTc-DTPA adult administered activities available for assessment. Additionally, there was one report using 99mTc-DMSA and one using 99mTc-glucoheptonate included in the submissions and discarded from the analysis. Two submitted adult diuretic renal scintigraphy reports failed to note the dose and were also excluded and 10 reports were excluded because they were for children. Minimum, average, and maximum administered activities were determined; DRLs and AAAs are presented in Table 2 and are later compared with the DRLs and AAAs of non-U.S. facilities, as available.
Analysis of Administered Activities by Radiopharmaceutical
DISCUSSION
The priority for any imaging study is to achieve the diagnostic quality necessary to answer the clinical question. In the setting of exams using ionizing radiation, this priority must be carefully balanced with the patient radiation dose. In the absence of empiric experimental data, survey data and the resultant determined reference levels may be used to guide practitioners and professional societies. DRLs, indicating the 75th percentile for administered activities for a specific nuclear medicine procedure and radiopharmaceutical, can indicate whether the amount administered is unusually high and are viewed as the first step in optimizing patient dose (6). Facilities routinely exceeding the DRL may benefit from reviewing their technique to determine whether exams may be performed using a lower administered activity while maintaining adequate diagnostic quality. In contrast, the AAA, indicating the 50th percentile, is considered a goal for nuclear laboratories to strive for with prescribed administered activities. The overarching objective of both these metrics is to aid facilities in avoiding unnecessary patient radiation dose.
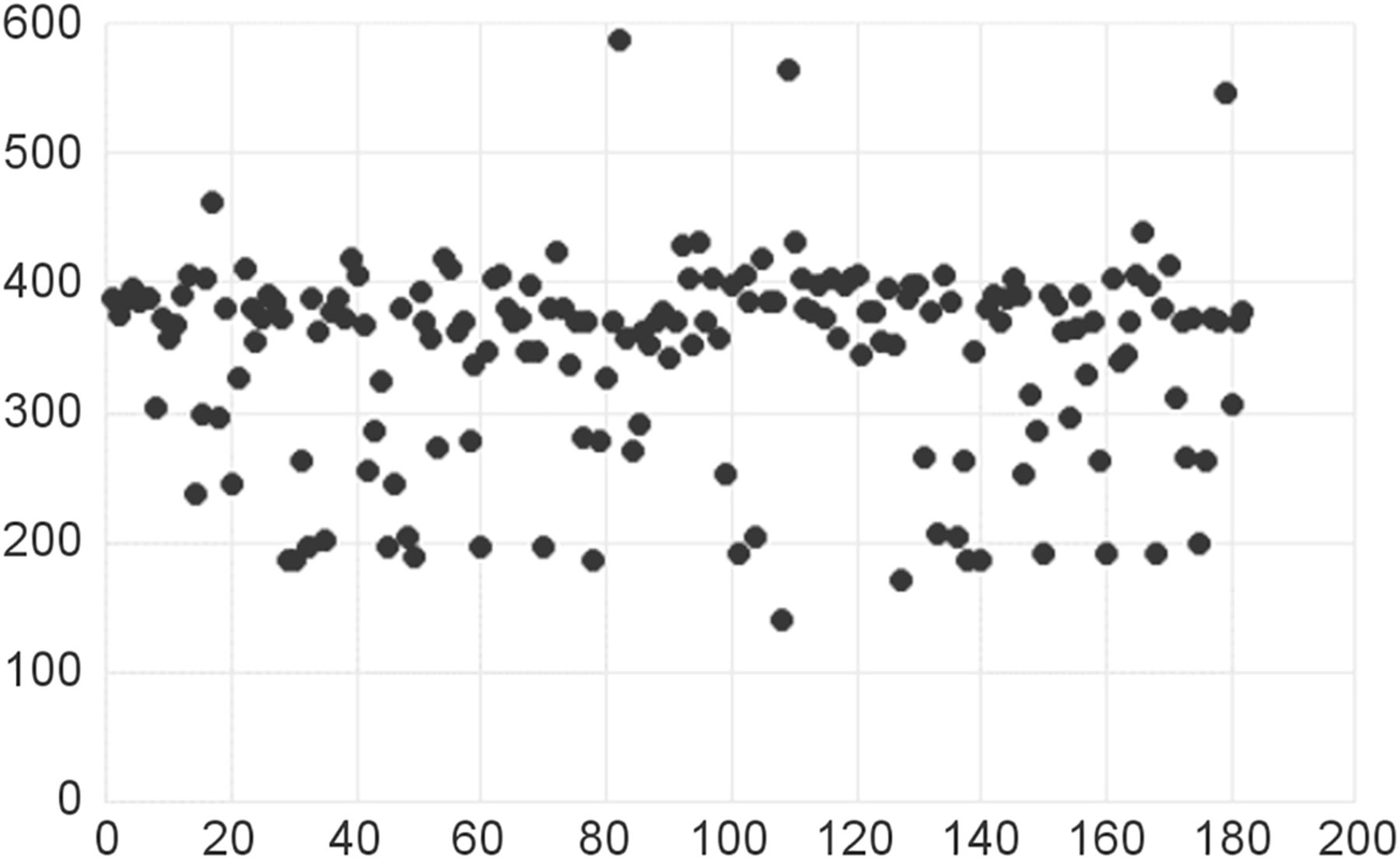
Several high-quality surveys of U.S. nuclear medicine facilities have identified the DRLs and AAAs for many radiopharmaceuticals and studies; however, renal scintigraphy either has not been reviewed or has yielded too few data points to provide accurate values until now (2–4). Analysis of survey results from Intersocietal Accreditation Commission accreditation data revealed a U.S. DRL of 392.2 MBq (10.6 mCi) for 99mTc-MAG3 and a minimally lower AAA of 370 MBq (10 mCi), with nearly a third of values falling between these 2 values and another third being within 37 MBq (1 mCi) of either side of this range, indicating a narrow band of administered activities across most sites (Fig. 1). The same analysis revealed slightly greater values for 99mTc-DTPA, with a U.S. DRL of 531.69 MBq (14.4 mCi) and an AAA of 445.85 MBq (12.1 mCi) (Fig. 2).
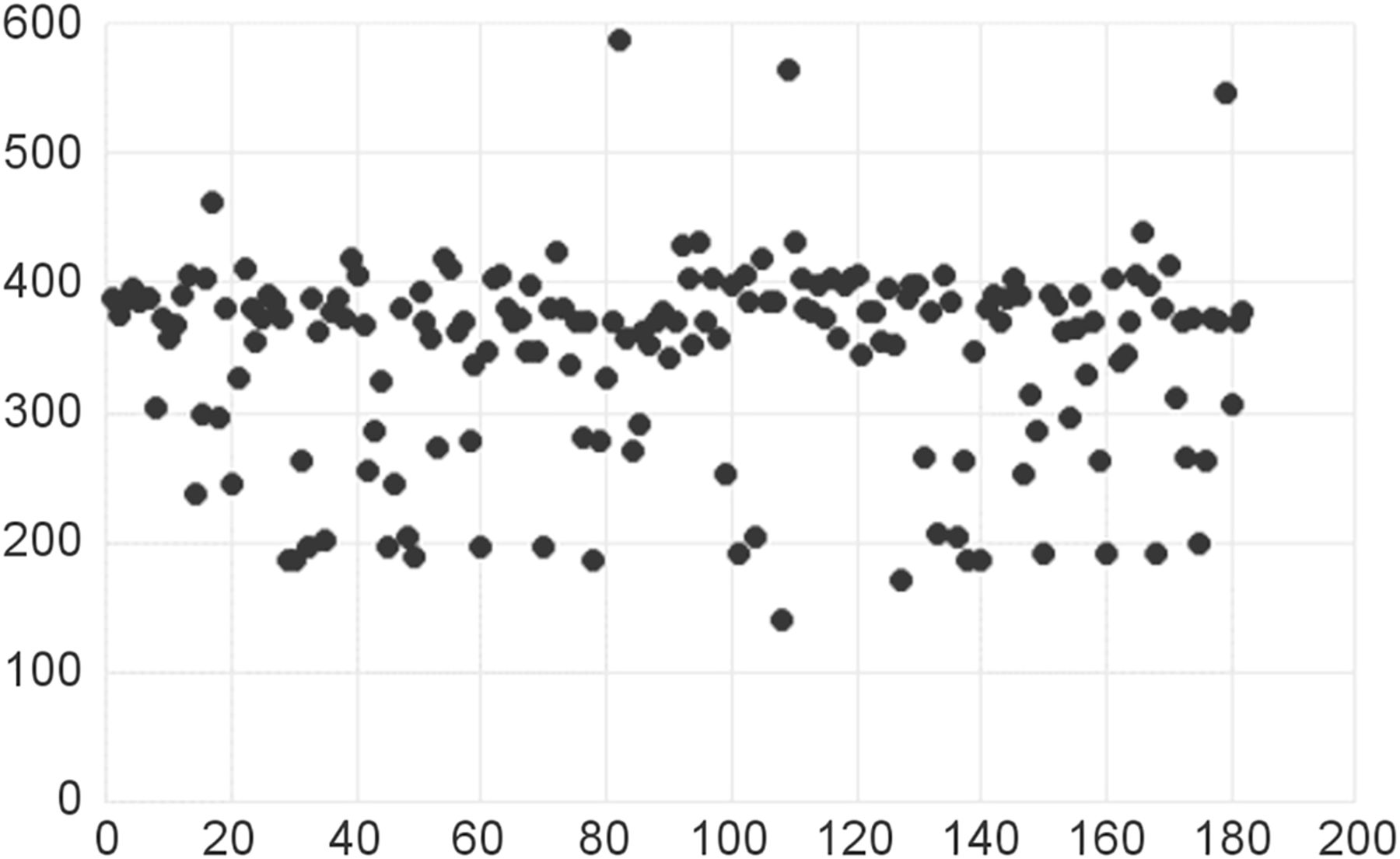
Distribution of 182 99mTc-MAG3 administered doses. Vertical axis is activity (MBq). Horizontal axis is number of doses. Most values are close to 370 MBq (10 mCi).

Distribution of 24 99mTc-DTPA administered doses. Vertical axis is activity (MBq). Horizontal axis is number of doses. Nearly all fall within 370- to 555-MBq (10–15 mCi) range.
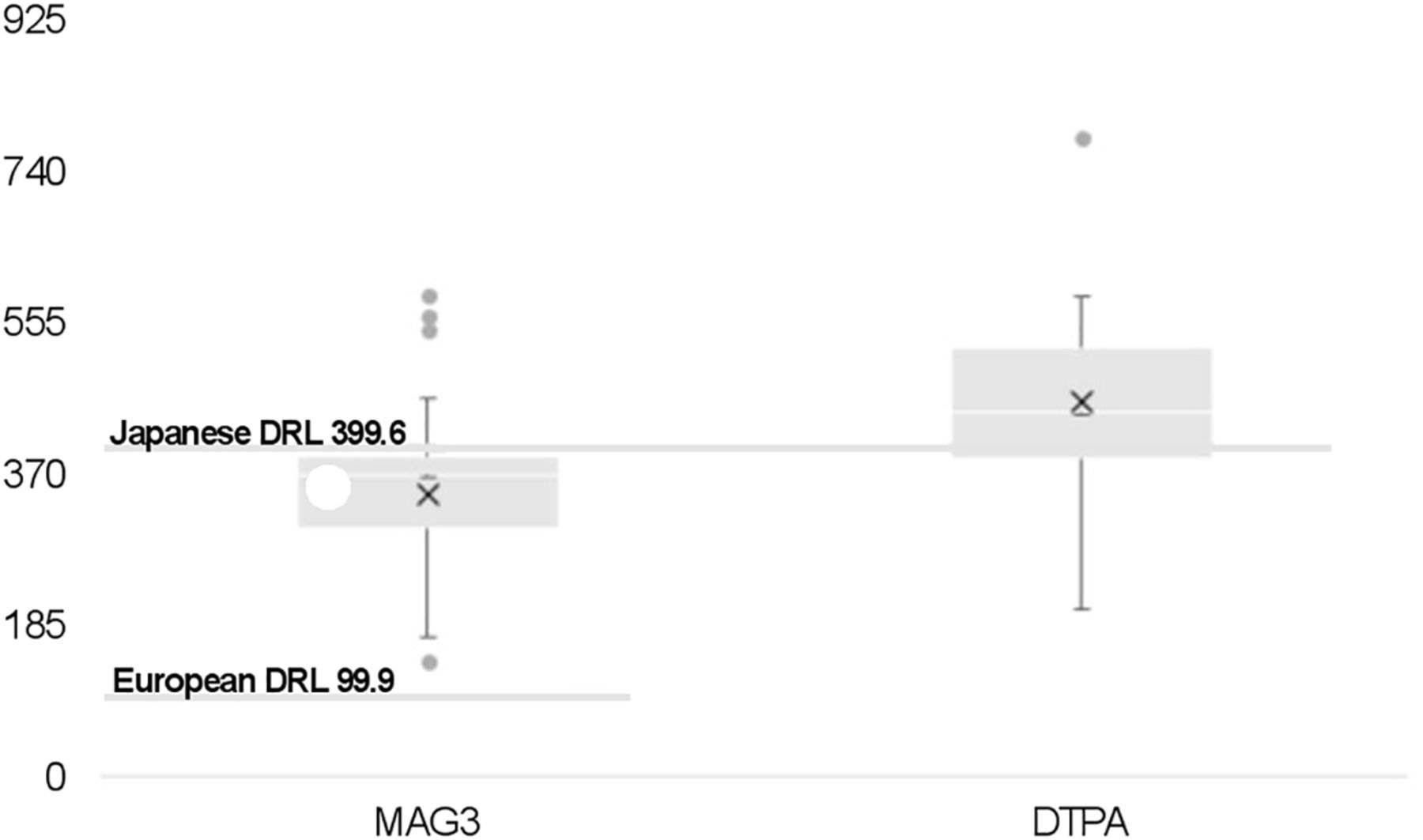
Such values are available for Japan and much of Europe, providing an opportunity to compare and contrast with the Intersocietal Accreditation Commission survey results. DRLs for Japan are 399.6 MBq (10.8 mCi) for both 99mTc-MAG3 and 99mTc-DTPA (7). In contrast, European researchers found a much lower 99mTc-MAG3 DRL of 99.9 MBq (2.7 mCi) to be the most common value reported from its survey of 36 countries, with the individual-country DRLs ranging from 99.9 to 370 MBq (2.7–10 mCi) (8). Most U.S. 99mTc-MAG3 administered activities fell below Japan’s DRL, but all exceeded the European DRL. In contrast, most U.S. 99mTc-DTPA administered activities exceeded Japan’s DRL (Fig. 3).
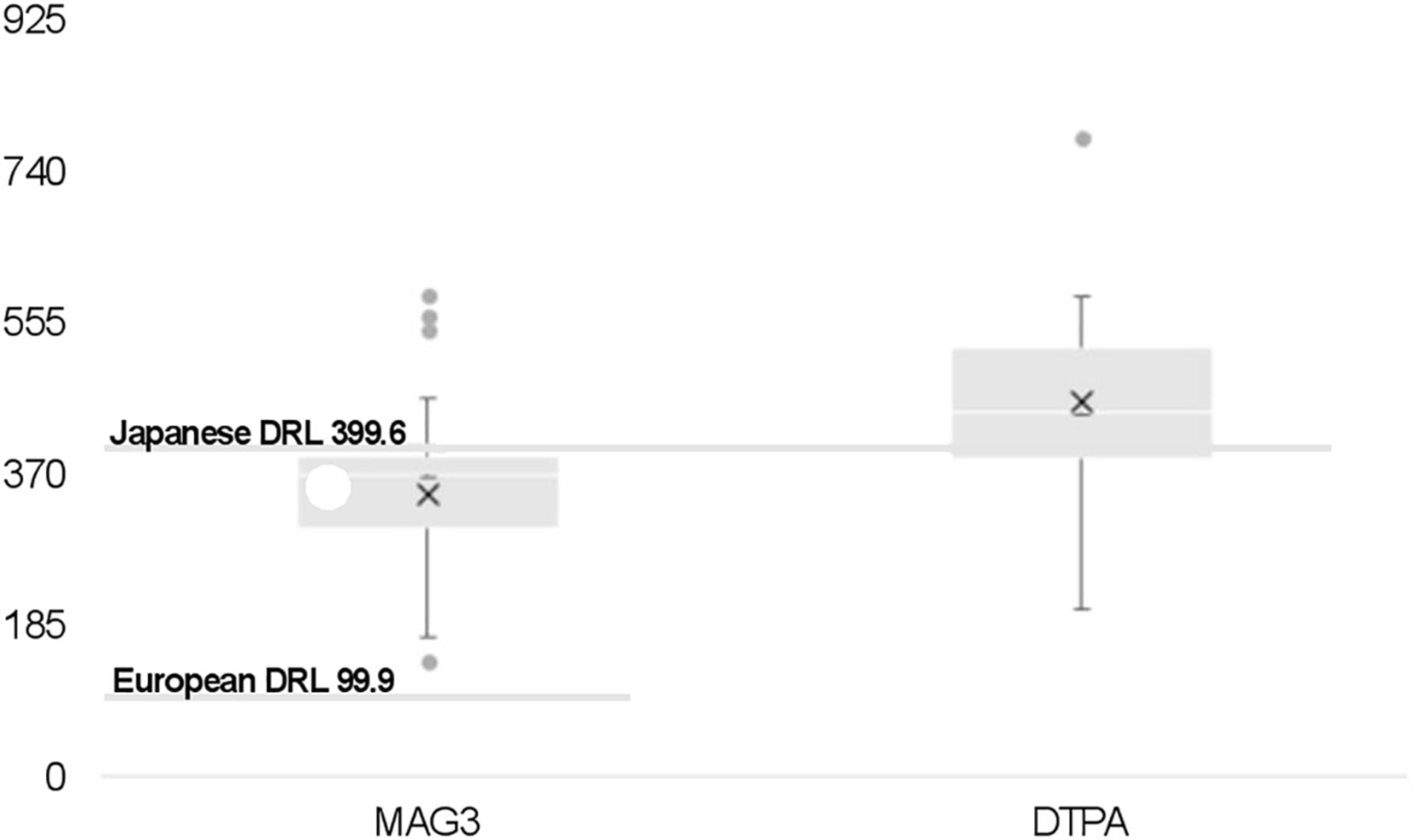
Box-and-whisker plot comparing minimum, maximum, and quartiles for U.S. 99mTc-MAG3 and 99mTc-DTPA administered activities (MBq) along with outliers vs. DRLs from Japan and Europe (99mTc-MAG3 only).
The American College of Radiology–Society for Pediatric Radiology practice parameter for renal scintigraphy allows for adult doses of up to 370 MBq (10 mCi) for 99mTc-MAG3 and 555 MBq (15 mCi) for 99mTc-DTPA (9). In contrast, whereas the SNMMI-EANM procedure standard allows for doses of up to 370 MBq (10 mCi) for both agents, it recommends lower administered activities of 37–185 MBq (1–5 mCi) for most applications (10)]. This lower range is supported by at least one study, which showed no increased interpretation benefit or relative function determination accuracy when comparing doses of 300–370 MBq (8.1–10 mCi) with doses of 37–185 MBq (1–5 mCi) (11). The Intersocietal Accreditation Commission survey analysis shows that administered activities in the United States generally are consistent across facilities at the upper range of the values endorsed by societal parameters and guidelines, with only a small portion of facilities using 99mTc-MAG3 administered activities well below both the DRL and AAA.
CONCLUSION
This practice-based survey of administered activities used by a large number of U.S. nuclear laboratories for the performance of adult dynamic renal scintigraphy has resulted in the first valid national reference levels for this nuclear medicine exam. Resultant DRLs of 392.2 MBq (10.6 mCi) for 99mTc-MAG3 and 531.7 MBq (14.4 mCi) for 99mTc-DTPA, with AAAs of 370 MBq (10 mCi) for 99mTc-MAG3 and 445.9 MBq (12.1 mCi) for 99mTc-DTPA, were identified. These values may serve as benchmarks that nuclear medicine facilities may use to refine their renal scintigraphy protocols and to guide future societal recommendations and organizational accreditation processes. Given that reference levels are dependent on the state of practice and the technology available at a particular point in time, future downward evolution of these values will be likely, based on improvements in equipment, techniques, and expertise.
DISCLOSURE
Mary Farrell and Maria Costello are employees of the Intersocietal Accreditation Commission. Leonie Gordon is on the Intersocietal Accreditation Commission Board of Directors. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online April 5, 2021.
REFERENCES
- Received for publication December 7, 2020.
- Accepted for publication March 18, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}