


Abstract
A 51-y-old man underwent 18F-FDG PET for disease restaging of non-Hodgkin's lymphoma. Initial attenuation correction images demonstrated unilateral hemispheric cerebral hypometabolic activity. The remainder of the scan was otherwise unremarkable. Non–attenuation correction images demonstrated a patient motion artifact attributable to lateral movement of the patient's head during image acquisition. Subsequent repeat 18F-FDG PET showed normal cerebral cortical activity.
The following case report illustrates the importance of preventing motion of the patient's head during 18F-FDG PET, because of the consequent motion artifact resembling decreased cerebral metabolism.
CASE REPORT
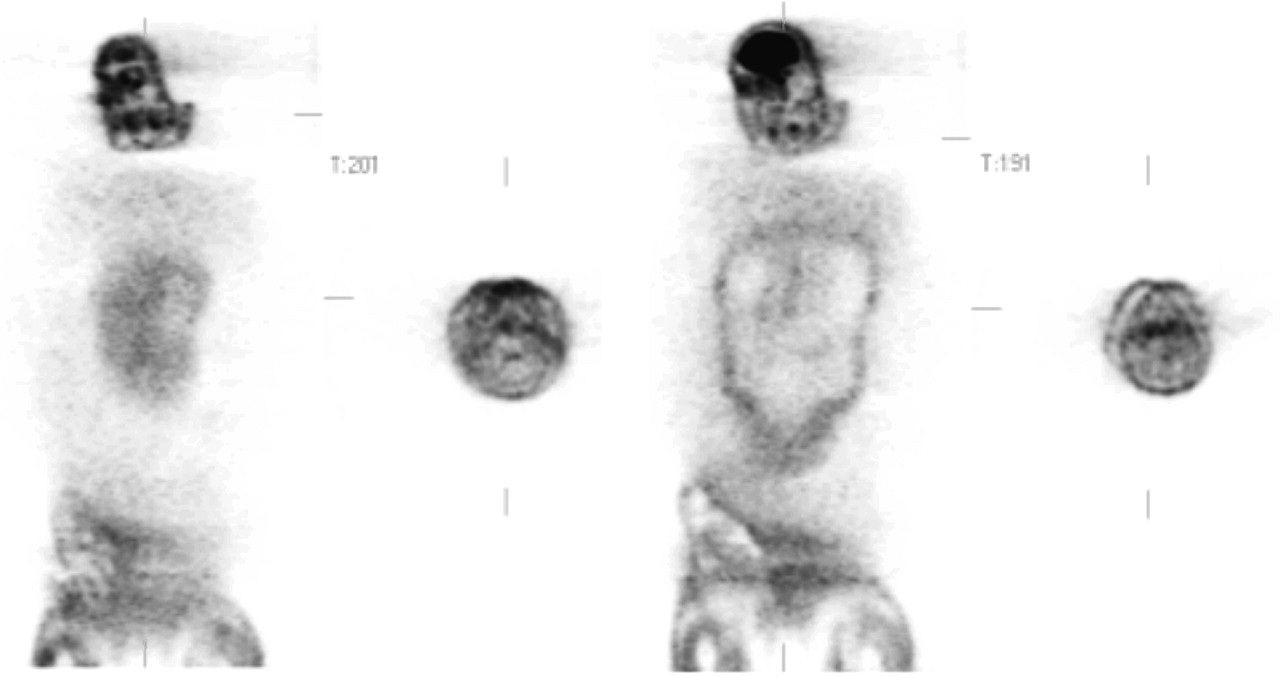
A 51-y-old man with a diagnosis of non-Hodgkin's lymphoma underwent 18F-FDG PET for disease restaging. Initial attenuation correction images demonstrated unilateral hemispheric cerebral hypometabolic activity (Fig. 1). The ipsilateral scalp also demonstrated hypometabolic activity (Fig. 1). The remainder of the scan was otherwise unremarkable. Non–attenuation correction images demonstrated lateral displacement of the patient's head during image acquisition (Fig. 2). As a result of this movement, the images presented a motion artifact simulating a unilateral decrease in cerebral metabolic activity. The patient was rescheduled for repeat 18F-FDG PET. Subsequent images revealed normal cerebral cortical activity (Fig. 3).
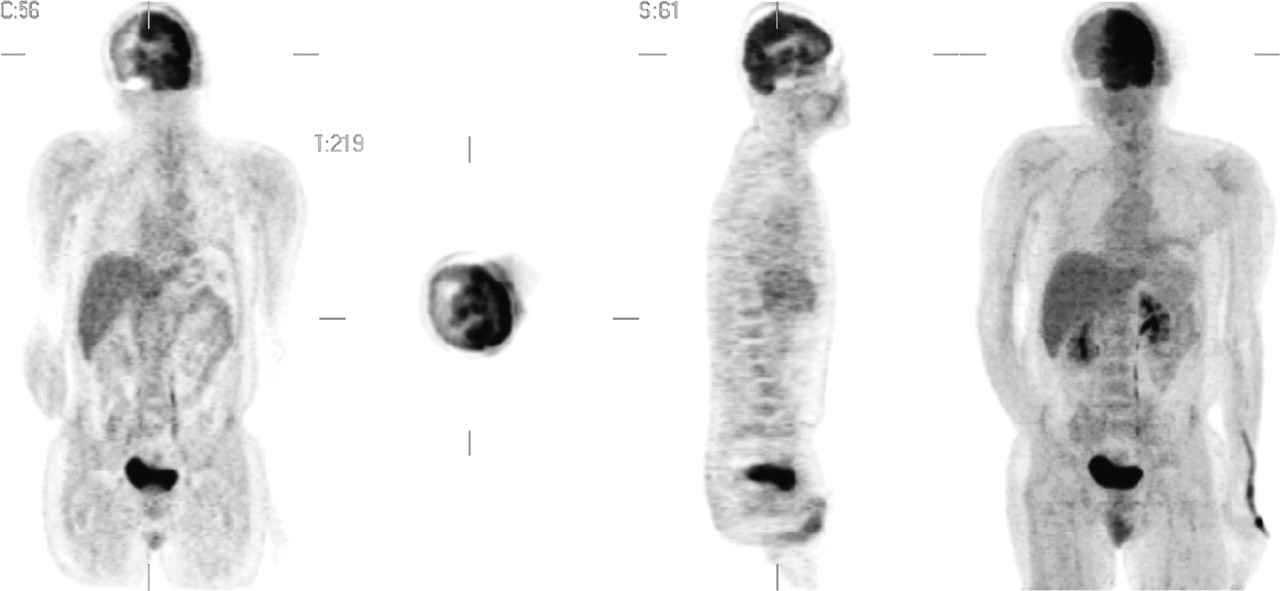
Coronal, transaxial, sagittal, and maximum-intensity-projection 3-dimensional 18F-FDG PET attenuation correction images demonstrating unilateral hemispheric cerebral hypometabolic activity. Decreased activity also was seen in the ipsilateral scalp.
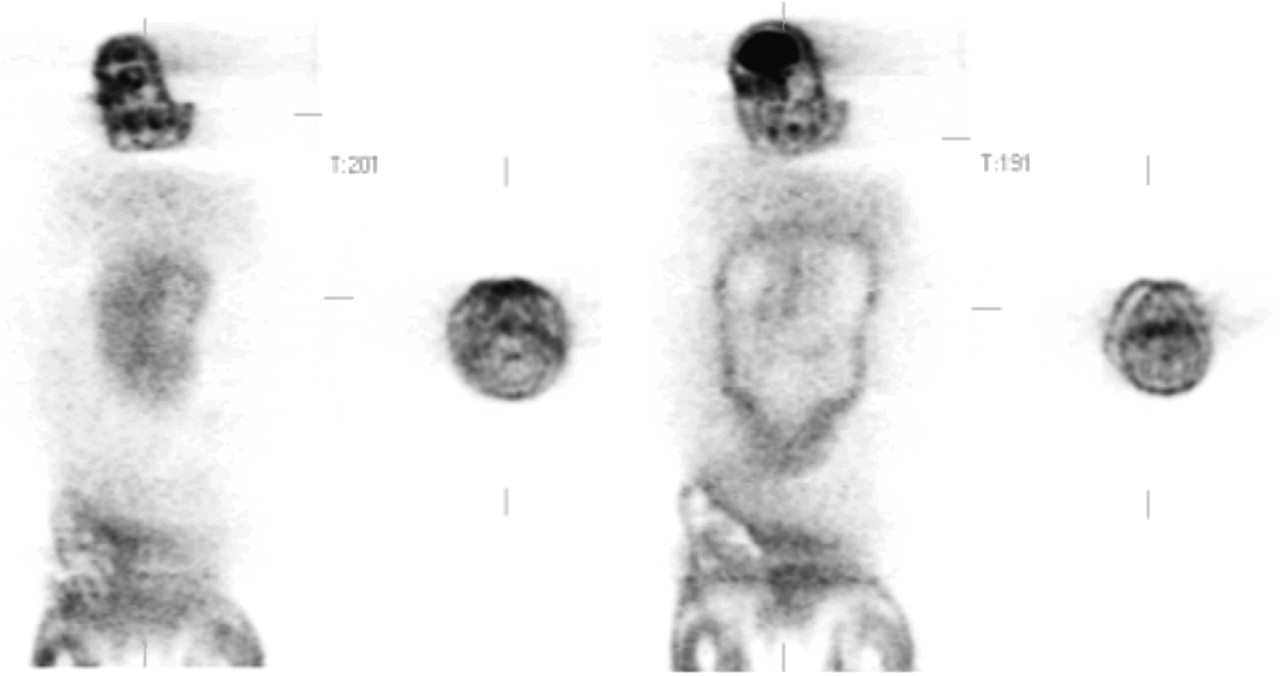
Coronal and transaxial 18F-FDG PET non–attenuation correction images demonstrating patient lateral head motion at sequential stages.
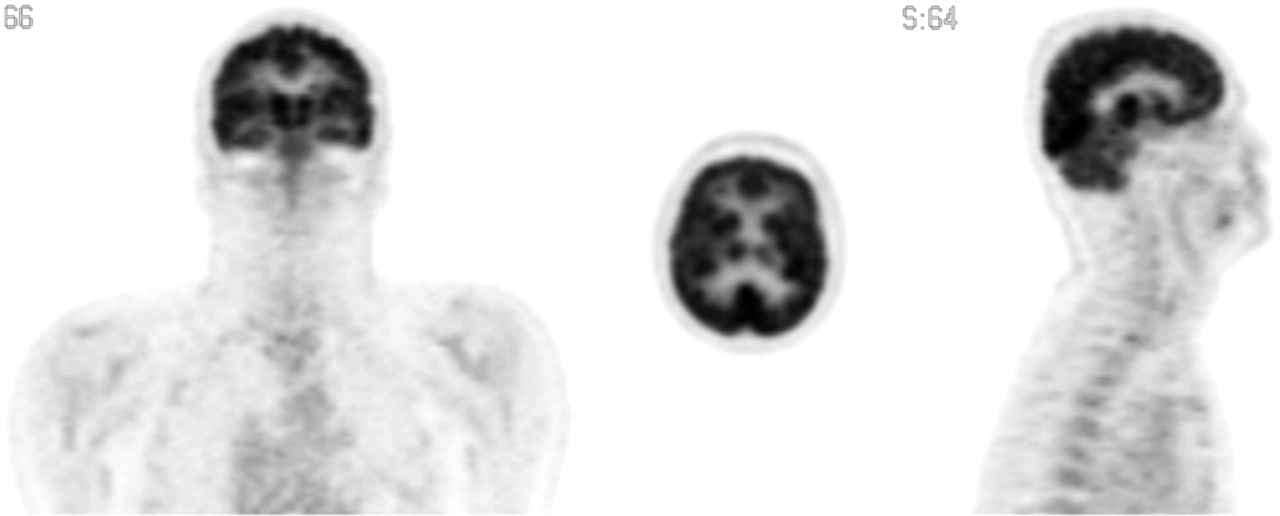
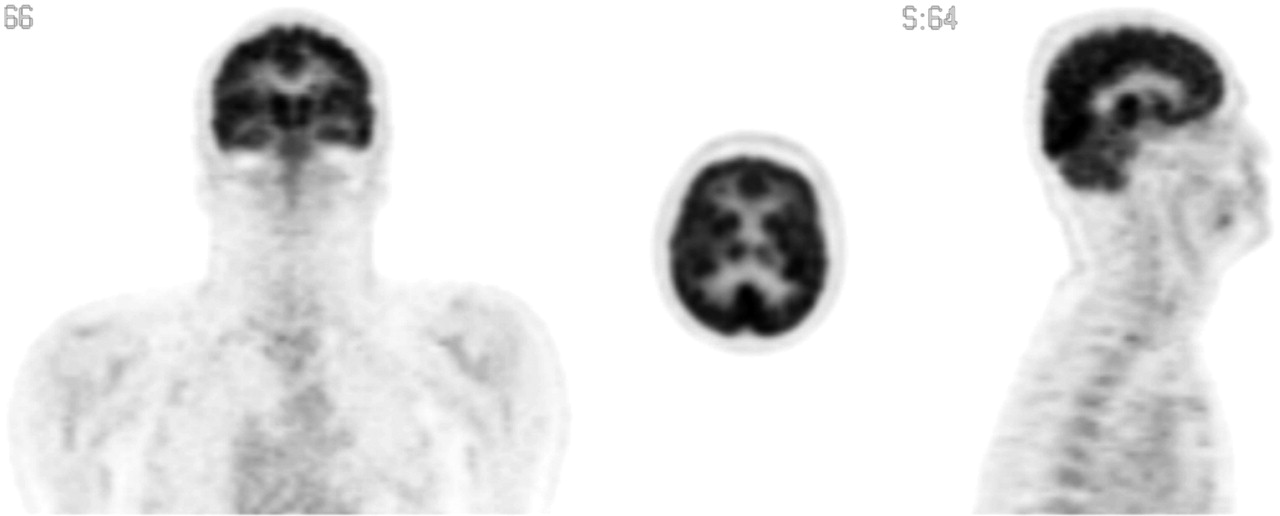
Coronal, transaxial, and sagittal attenuation correction images from repeat scan demonstrating normal cerebral cortical activity.
DISCUSSION
Attenuation correction is needed in PET not only for accurate quantification of the radioactivity detected by the PET scanner but also for proper visualization of different anatomic structures. The accuracy of attenuation correction depends on the proper alignment of transmission and emission scans. Stabilization of the head, either with a brace or lateral cushioning, may aid in reducing lateral motion during the scanning process. Movement that occurs between the emission and the transmission scans will produce inaccurate quantification and, for severe patient motion, even image artifacts. The effect of motion on the accuracy of attenuation correction has been studied with phantom simulations (1). Displacements of as little as 5 mm may cause errors of as much as 14% in measured activity. In PET scans of real brains, a 5-mm mismatch between emission and transmission scans can cause an ∼10% error in a 1-cm-thick cortical region of interest, and a 10-mm mismatch can cause a 25% error (2). With computer realignment of emission and transmission images, the errors can be corrected. However, for severe patient motion, the realignment may be less satisfactory and may leave residual inaccuracies in the attenuation correction. In these cases, attenuation correction can be calculated for the brain without a transmission scan by use of a standard attenuation coefficient. However, this method is not accurate for areas in which there is an interface of soft tissues with air or bony structures, such as in the body, particularly the chest. At present, methods to improve the accuracy of motion correction are being explored (3–5).
References
- Received for publication March 20, 2006.
- Accepted for publication March 27, 2006.





{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.