Article Text

Abstract
Background Patients with systemic ventricles of right ventricular morphology are at high risk of contractile dysfunction, the cause of which has not been fully elucidated.
Objective To assess whether ischaemia or infarction contributes to ventricular impairment in unoperated patients with uncomplicated congenitally corrected transposition of the great arteries (TGA) by studying myocardial perfusion and function.
Setting Paediatric and adult congenital cardiac clinics of a tertiary referral centre.
Patients Five patients with congenitally corrected TGA but without associated structural cardiac defects (aged 3.5 to 34 years).
Interventions Maximal exercise stress testing using standard or modified Bruce protocols. Sestamibi (technetium-99m methoxy isobutyl isonitrile) scanning after isotope injection at maximal exercise and rest.
Main outcome measures Maximum exercise capacity; right ventricular myocardial perfusion, regional wall motion, and thickening; right ventricular ejection fraction.
Results The two youngest patients (3.5 and 11 years) had normal exercise capacity for age, while the others had reduced exercise performance. Sestamibi scanning showed reversible myocardial ischaemia in four patients and fixed defects indicating infarction in five. Irreversible defects were mostly associated with impaired wall motion and thickening. The ejection fraction was normal (65%) in the youngest patient but < 55% in the others (mean (SD) 47(11)%).
Conclusions Patients with unoperated congenitally corrected TGA have a high prevalence of myocardial perfusion defects, with consequent abnormalities of regional wall motion and thickening, and impaired ventricular contractility. These data suggest that ischaemia and infarction are important in the pathogenesis of ventricular failure in this condition.
- congenitally corrected transposition of the great arteries
- ventricular dysfunction
- myocardial perfusion
- sestamibi scanning
Statistics from Altmetric.com
- congenitally corrected transposition of the great arteries
- ventricular dysfunction
- myocardial perfusion
- sestamibi scanning
Patients with congenitally corrected transposition of the great arteries (TGA) are at high risk of developing systemic ventricular dysfunction, independent of their commonly associated structural defects.1-6 The systemic ventricle is of right ventricular morphology and it is considered that long term exposure to systemic pressure may cause gradual failure of the myocardium.5-7 Patients with this condition have hypertrophy of the systemic ventricle persisting beyond the neonatal period, placing an increased demand on the coronary arterial supply, which mostly frequently is from a morphologic right coronary system.1 Research has shown that patients with a systemic right ventricle following atrial baffle repair for simple transposition of the great arteries (dTGA) have defects of right ventricular myocardial perfusion, which may contribute to right ventricular dysfunction in this group.8 ,9 In these patients, however, the effects of systemic arterial hypoxaemia for the first three to 12 months of life and of cardiopulmonary bypass (CPB) are not known and may contribute to the observed abnormalities on perfusion imaging.
Isolated case reports suggest that perfusion defects may also be present in patients with congenitally corrected TGA.10 ,11The aim of this investigation was to assess the contribution of myocardial ischaemia or infarction to the aetiology of systemic ventricular dysfunction in a group of unoperated, fully saturated patients with congenitally corrected TGA, using advanced nuclear medicine techniques to evaluate right ventricular myocardial perfusion, wall motion, and wall thickening.
Patients and methods
Five patients (three male and two female aged from 3.5 to 34 years) with congenitally corrected TGA and without associated structural cardiac defects were studied (table 1). They were considered representative of all patients with uncomplicated, unoperated congenitally corrected TGA from the Sydney area attending our institution at the time of the study. One patient had had a permanent transvenous pacemaker system (VVIR) implanted three years earlier, but the others had not undergone surgery. Significant Ebstein’s anomaly of the tricuspid valve was not present, but echocardiograms showed mild or moderate tricuspid regurgitation in each patient except the youngest. None had complained of chest pain suggestive of angina pectoris. Informed consent was given by all patients and/or parents. The study protocol was approved by the ethics committee of the Royal Alexandra Hospital for Children.
Results of exercise testing and functional assessments
Myocardial perfusion was assessed with the radiopharmaceutical sestamibi (technetium-99m methoxy isobutyl isonitrile) using a one day stress rest protocol.10-13 Patients were exercised on a Schiller CS100 treadmill to maximum exercise capacity according to a standard or modified Bruce protocol after overnight fasting.14 Approximately one minute before the end of the period of exercise—that is, at peak exercise, 5.29 MBq/kg sestamibi was injected intravenously. The second study was performed four hours later at rest using 15.86 MBq/kg sestamibi. Single photon emission computed tomographic (SPECT) images were acquired one hour after each injection using a Siemens triple detector gamma camera (MULTISPECT 3).
High resolution collimators were used with a non-circular orbit with two detectors undergoing a 120 rotation for 32 frames, at 40 seconds per frame with a 64 × 64 matrix. Reconstruction of the stress images was performed using a Butterworth filter (cut off 0.28 to 0.40 and power factor 10). Acquisition parameters were the same for the rest study with the addition of electrocardiogram gated acquisition. The best histogram was set at 20% around the peak heart rate, slightly offset to the lower side. Images were gated at eight frames per cardiac cycle using an R wave trigger. Reconstruction of the rest data used a Butterworth filter with slightly higher cut off (0.4 to 0.5) and power factor 10.
Perfusion scans were read by a single observer (EJB) who was aware of exercise test results but was blinded to the clinical status and echocardiographic data of each patient. The perfusion studies were read in transaxial, horizontal long axis, and vertical long axis views (represented schematically in fig 1).15 ,16 For reasons of simplicity and clarity we used four segments each (anterior, lateral, inferior, and septal) at basal, mid-ventricular, and apical levels, giving a total of 12 segments. Tracer uptake in each segment was graded as normal or mildly, moderately, or severely reduced; defects were confirmed in orthogonal planes. Gated SPECT images were read in cine mode to assess wall motion, which was scored as normal or reduced. End diastolic and end systolic frames were compared to assess wall thickening, which was also graded as normal or reduced. Right ventricular ejection fraction was calculated using Siemens’ automated gated SPECT processing software.

Standardised right ventricular perfusion images used for segmental analysis in patients with congenitally corrected TGA. (A) Transaxial (cross sectional) view. (B) Vertical long axis view. (C) Horizontal long axis view. S, septum; An, anterior wall; L, lateral wall; I, inferior wall; Ap, apex.
Results
Table 1 lists details of individual exercise tests and functional assessments. The results of right ventricular perfusion are described below (table 2).
Location and severity of perfusion defects
PATIENT 1
A 3.5 year old boy was diagnosed at 1 day old having presented with supraventricular tachycardia and a murmur. He was asymptomatic (New York Heart Association (NYHA) class I) at the time of the study. Perfusion scanning showed a mild fixed defect in the inferior wall indicating infarction. There was a moderate reversible defect in the anterior wall and a mild reversible defect in the inferior wall. Wall thickening and wall motion in all areas were normal, with a right ventricular ejection fraction (RVEF) of 65%.
PATIENT 2
An 11 year old boy was diagnosed at 4 months old having presented with a respiratory arrest complicating an episode of bronchiolitis, at which stage a murmur was found. He was in NYHA class I at the time of the study. Perfusion scanning showed a moderate fixed defect in the anterior wall and mild fixed defects in the mid-inferior and basal inferior walls indicating infarction. There was a severe reversible defect in the inferoapical wall and a moderate reversible defect in the septum. Wall thickening and wall motion of the anterior and inferior walls and septum were reduced, with an RVEF of 39%.
PATIENT 3
An 18 year old woman was diagnosed at 10 years old having presented with a murmur and bradycardia. A permanent transvenous VVIR pacemaker was inserted for symptomatic complete heart block when she was 15 years old. She was asymptomatic (NYHA class I) at the time of the study. Perfusion scanning showed mild and moderate fixed defects in the mid-inferior and basal inferior walls and septum indicating infarction. There were no reversible defects. Wall thickening and wall motion of the inferior wall and septum were reduced, with an RVEF of 42%.
PATIENT 4
A 33 year old man was diagnosed at 18 years old having presented with an abnormal chest radiograph during pre-immigration testing. He was in chronic atrial fibrillation with A-V dissociation, had reduced exercise tolerance, and in NYHA class II at the time of the study. Perfusion scanning showed a moderate fixed defect in the inferior wall indicating infarction and a severe reversible defect in a small area of the basal septum. Wall thickening and motion of the inferior wall were reduced, with an RVEF of 52%.
PATIENT 5
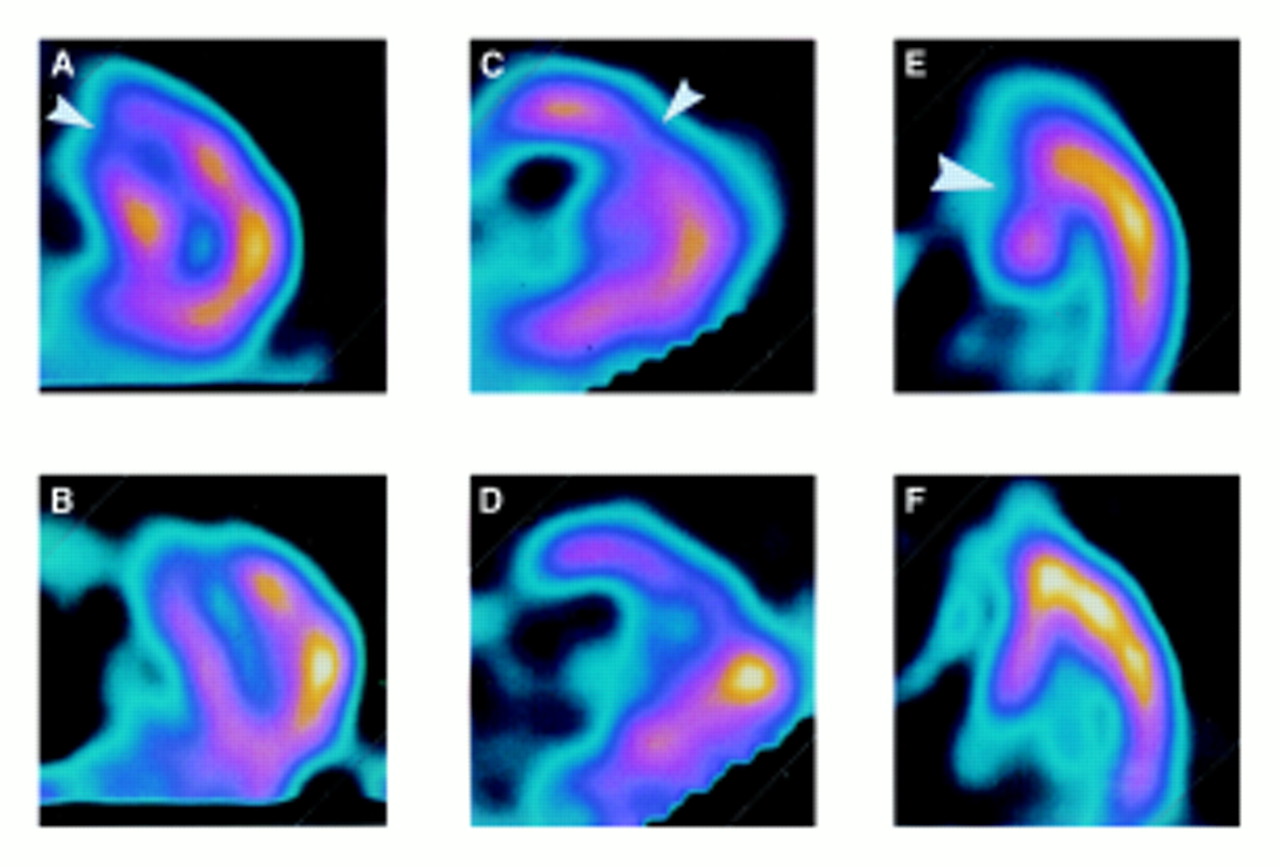
A 34 year old woman, was diagnosed at the age of three years, having presented with a murmur. She was mildly symptomatic (NYHA class II) at the time of the study. Perfusion scanning showed moderate fixed defects in the anterior wall and basal septum indicating infarction, with a moderate reversible defect in the apical and mid-septum (fig 2). Wall thickening and motion of the septum and anterior wall were reduced, with an RVEF of 38%.

Sestamibi scan of patient 5 showing a fixed defect (indicating infarction) in the anterior wall (small arrowheads) and reversible ischaemia in the septum (large arrowhead). Transaxial views at mid-ventricular to basal level at (A) stress and (B) rest. Vertical long axis views at (C) stress and (D) rest. Horizontal long axis views at stress (E) and rest (F).(Refer to fig 1 for diagram of standard views).
Discussion
Although some patients with congenitally corrected TGA may lead normal lives without evidence of cardiac decompensation,2 ,7 many develop right ventricular failure.3 ,4 ,17 This may result in symptoms of congestive cardiac failure, decreased functional capacity, and early death. Most previous studies have suggested that dysfunction of the right ventricle is gradual in onset and may not be manifest until the third or fourth decade of life. The mechanism of failure is unclear but inability to tolerate long term functioning at systemic pressure may result from the macroscopic and microscopic structure of the right ventricular myocardium.17 ,18 This problem may be exacerbated by the common finding of insufficiency of the tricuspid valve. The contribution of inadequate right ventricular myocardial perfusion in this setting has not been assessed.
MYOCARDIAL ISCHAEMIA AND CORONARY SUPPLY
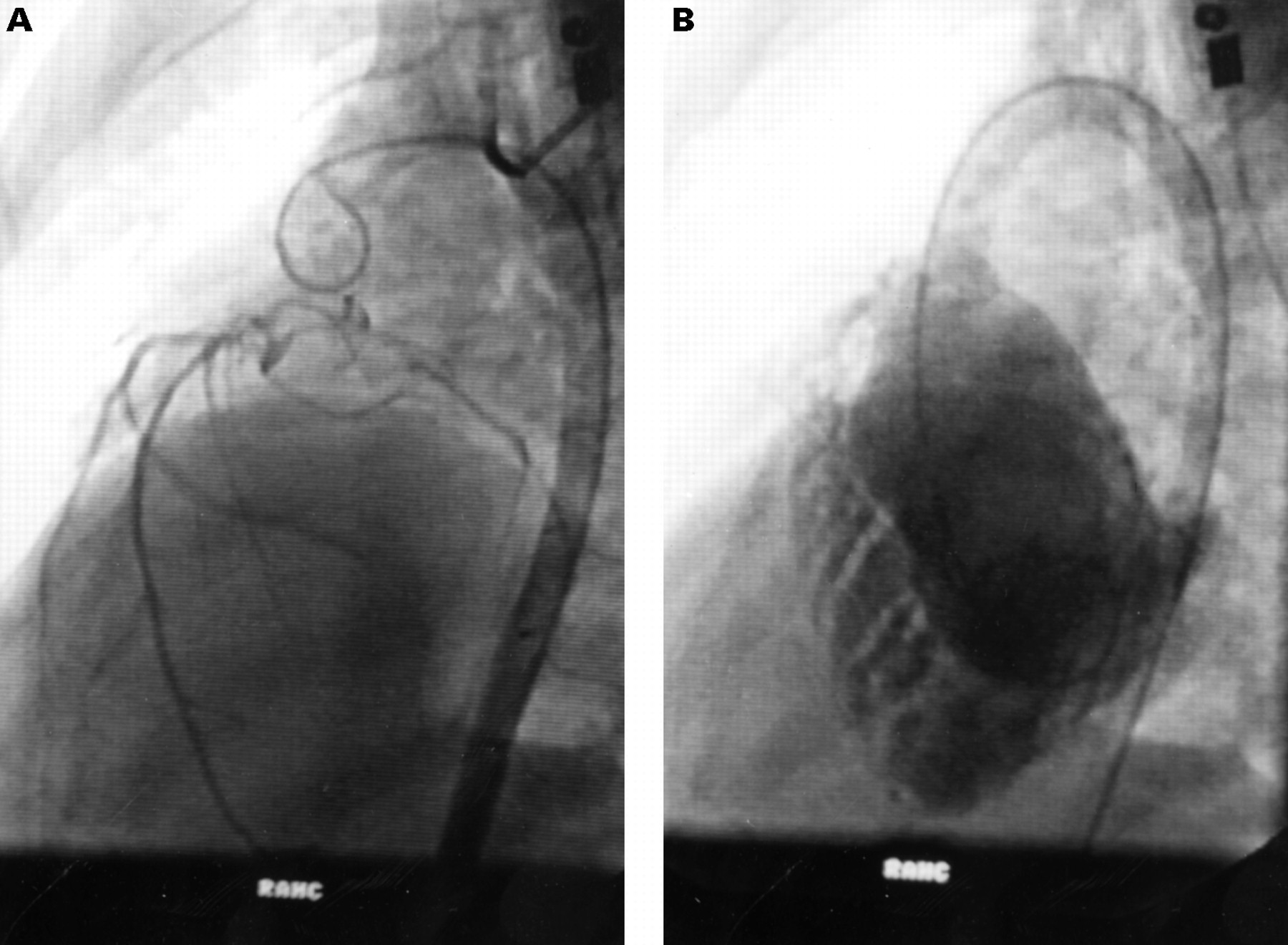
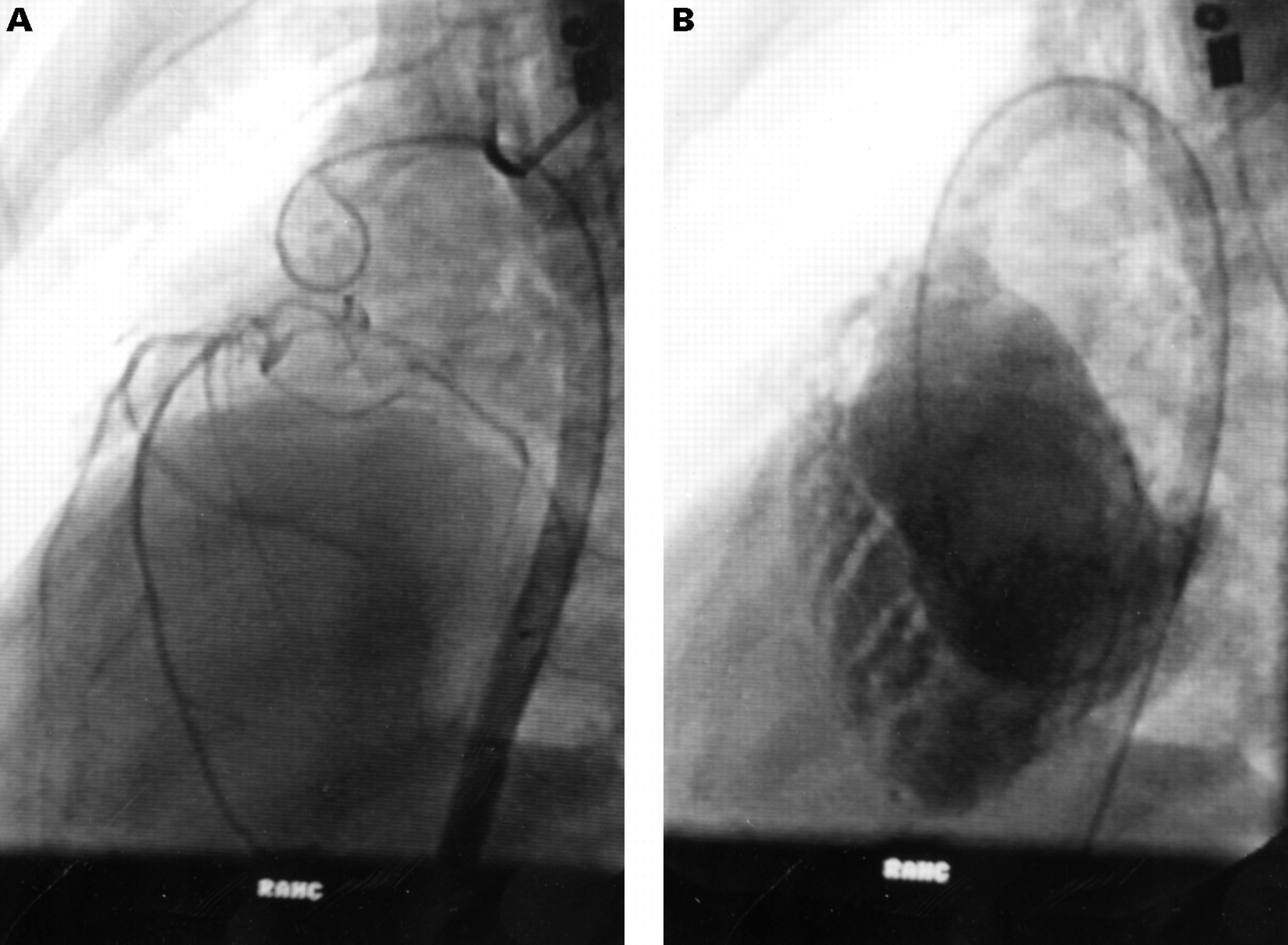
We now report significant ischaemia and infarction in patients with unoperated congenitally corrected TGA, with consequent contractile dysfunction. These findings may result from an inadequate coronary arterial supply, the usual coronary arrangement in patients with congenitally corrected TGA being coronary inversion1 ,17; therefore, although the morphologic right ventricle is on the left side of the heart, it is supplied by a morphologic right coronary artery system (fig 3A). This system may provide inadequate flow in the presence of considerable myocardial hyperplasia and hypertrophy seen when the right ventricle functions at systemic pressures for long periods.17 ,19 ,20 Examination of the right ventricle subjected to systemic pressure shows gross hypertrophy compared with the thin wall of the right ventricle subjected to normal pressure, the discrepancy being especially conspicuous towards the apex (fig 3B). Hypertrophy places substantial extra demand on the right coronary arterial supply, which, as seen in fig 3A is less extensive than from a left coronary system. Progressive ischaemia will probably develop in this condition.
{kind=link}
{kind=link}
{kind=link}
Angiograms of a (non-study) patient with congenitally corrected TGA. (A) Late phase aortogram (left anterior oblique view) showing inverted coronary artery pattern with sparse coronary supply to the right ventricle. (B) Right ventriculogram (left anterior oblique view) showing gross hypertrophy and trabeculation, especially of the apical half of the ventricle.
PERFUSION DEFECTS AND VENTRICULAR DYSFUNCTION
The data from this small group of patients suggest that substantial reversible and fixed right ventricular myocardial perfusion defects are common in patients with congenitally corrected TGA. Defects were most frequently found in the anterior and inferior walls and septum. The lateral wall of the ventricle was not involved. Perfusion defects at rest were frequently associated with reduced regional wall thickening and wall motion and reduced right ventricular systolic function. This finding suggests a causal relation between fixed myocardial perfusion defects and ventricular dysfunction. Interestingly, the only patient with normal systemic ventricular function was 3.5 years of age, suggesting possible progression of ischaemia related myocardial dysfunction with increasing age.
SESTAMIBI SCANNING OF THE RIGHT VENTRICLE
Assessment of myocardial perfusion, wall motion, and ejection fraction using the radioisotopes thallium-201 or sestamibi is well established in adults and children.21 ,22 While assessment of right ventricular perfusion is less well described, the technique should not be any less applicable to the right than the left ventricle. Recent studies have reported significant right ventricular perfusion defects associated with wall motion abnormalities in patients with dTGA who underwent atrial baffle repair (Mustard or Senning).8 ,9 The heart after a Mustard or Senning procedure is analogous to the congenitally corrected TGA heart in terms of long term functioning of the morphological right ventricle as a systemic ventricle. These groups, however, had a variable period of arterial hypoxaemia and a lengthy cardiopulmonary bypass procedure, often without modern techniques of myocardial protection: both factors may have contributed to the observed perfusion defects. Perfusion defects have been reported previously in other groups of patients who had surgery involving CPB.23 ,24 Hayes et alcompared patients after both arterial switch and CPB surgery not involving the coronary arteries23: each group had a high incidence of perfusion defects, suggesting that CPB may be responsible.
In contrast, our patients have a systemic right ventricle but have not undergone CPB surgery. They therefore serve as a model for anatomical situations in which the systemic ventricle is of right ventricular morphology. We considered that myocardial perfusion data from this group would help to clarify the aetiology of right ventricular dysfunction commonly seen in patients with congenitally corrected TGA and to validate data concerning impaired right ventricular perfusion in patients with dTGA after atrial baffle repair.
STUDY LIMITATIONS
This study examined only a relatively small number of unoperated patients, as congenitally corrected TGA is a rare condition often associated with intracardiac abnormalities requiring open heart surgery.1 The five patients with uncomplicated congenitally corrected TGA, who currently live in the Sydney area, were studied at our institute. In addition, data presented here are from single measurements in each patient and therefore only presumptive conclusions can be made regarding the progression of perfusion defects with increasing age. This question may be more clearly addressed by prospective serial studies.
CONCLUSIONS
In summary, we found evidence of impaired myocardial perfusion associated with regional cardiac dysfunction in the systemic ventricle of patients with unoperated, uncomplicated congenitally corrected TGA. These data suggest that the right ventricular coronary arterial supply may be inadequate for long term ventricular function at systemic pressures and that silent progressive irreversible ischaemia of the right ventricular myocardium may make an important contribution to the development of right ventricular dysfunction.