Article Text

Abstract
Background: Idiopathic gastroparesis is a syndrome characterised by severely delayed gastric emptying of solids without an obvious underlying organic cause. Although delayed gastric emptying is traditionally considered the mechanism underlying the symptoms in these patients, poor correlations with symptom severity have been reported.
Aims: To investigate proximal stomach function and to study the correlation of delayed gastric emptying and proximal stomach dysfunction with symptom pattern and severity in idiopathic gastroparesis.
Methods: 58 consecutive patients (19 men, mean (standard deviation) age 41 (2) years) with severely delayed solid gastric emptying (gastric half-emptying time (t1/2)>109 min) without an organic cause were recruited. They filled out a symptom-severity questionnaire and underwent a gastric barostat study for assessment of gastric sensitivity and accommodation. Correlation of these mechanisms with symptom pattern and overall symptom severity (sum of individual symptoms) was analysed.
Results: At two different cut-off levels for gastric emptying (upper limit of normal t1/2 up to 1.5 and 2 times), no significant change in symptom pattern occurred. 25 (43%) patients had impaired accommodation, and this was associated with higher prevalence of early satiety (p<0.005) and weight loss (p = 0.009). 17 (29%) patients had hypersensitivity to gastric distension, and this was associated with higher prevalences of epigastric pain (p = 0.005), early satiety (p = 0.04) and weight loss (p<0.005). Overall symptom severity was not correlated with gastric emptying or accommodation, but only with sensitivity to gastric distension (R = −0.3898, p = 0.003) and body weight (R = −0.4233, p = 0.001).
Conclusions: In patients with idiopathic gastroparesis, the symptom pattern is determined by proximal stomach dysfunction rather than by the severity of delayed emptying.
- MDP, minimal distending pressure
Statistics from Altmetric.com
Gastroparesis is a chronic, symptomatic, gastrointestinal disorder characterised by delayed gastric emptying of food solids with or without liquids. Symptoms of gastroparesis are variable and include nausea, vomiting, abdominal pain, postprandial fullness, bloating, early satiety and weight loss. Diabetes mellitus and prior vagotomy are considered the two major organic causes of gastroparesis. Gastroparesis is characterised as idiopathic when there is no obvious underlying organic cause.1–3
Although delayed gastric emptying is traditionally considered the major pathophysiological mechanism underlying the symptoms in idiopathic gastroparesis, gastric-emptying time has been shown to correlate poorly with symptom severity, and the symptom response to prokinetic therapy is poorly correlated with enhancement of gastric emptying.3–9 Hence, the hypothesis that the symptom pattern in patients with idiopathic gastroparesis is determined by a different pathophysiological mechanism should be considered. In patients with functional dyspepsia, proximal stomach dysfunction has been suggested to be an important mechanism for symptom generation.10,11 However, whether proximal stomach dysfunction contributes to symptom pattern in patients within the spectrum of idiopathic gastroparesis or functional dyspepsia with delayed gastric emptying is unclear.
The aim of this study was to correlate the symptom pattern in patients within the spectrum of idiopathic gastroparesis or functional dyspepsia with delayed gastric emptying (1) with the severity of the delay in gastric emptying and (2) with proximal stomach dysfunction.
PATIENTS AND METHODS
Study participants
Consecutive patients with severe upper gastrointestinal symptoms were eligible for participating in the study. Patients were referred to the outpatient clinic because of upper gastrointestinal symptoms suggestive of gastroparesis, and all underwent careful history taking and clinical examination, upper gastrointestinal endoscopy, routine biochemistry and upper abdominal ultrasound. Only patients with established idiopathic gastroparesis were included in the study. The diagnosis of idiopathic gastroparesis was based on the presence of appropriate symptoms,1–3 severely delayed solid emptying on a standardised solid gastric emptying breath test12–15 and the absence of an obstructive lesion in the stomach or the small bowel. We have previously shown the reproducibility of severely delayed gastric emptying in a similar patient population.9 Exclusion criteria were the presence of oesophagitis, gastric atrophy or erosive gastroduodenal lesions on endoscopy, a history of diabetes mellitus, major abdominal surgery, underlying psychiatric illness and the use of drugs potentially affecting gastrointestinal motility. During upper gastrointestinal endoscopy, biopsy specimens were taken from the antrum and the corpus to stain with cresyl violet for the presence of Helicobacter pylori. A psychiatrist ruled out anorexia nervosa in patients with weight loss in excess of 5% of the initial body weight. Informed consent was obtained from each participant. The protocol had been previously approved by the ethics committee of the University Hospital, Leuven, Belgium.
Symptom questionnaire
Before the barostat studies, each patient completed a questionnaire as previously reported.10,11,14 The patient was asked to grade the intensity (0–3; 0, absent; 1, mild; 2, relevant; and 3, severe, interfering with daily activities) of eight different symptoms (epigastric pain, bloating, postprandial fullness, early satiety, nausea, vomiting, belching and epigastric burning) over the past 3 months. Also, the amount of weight lost since the onset of the symptoms was noted and expressed as a percentage of the current body weight.
Gastric emptying studies
Gastric emptying for liquid and solids was measured in all patients, using the previously validated 14C-octanoic acid and 13C-glycin breath test.12–15 All studies were carried out in the morning after an overnight fast. The test meal consisted of 60 g of white bread and one egg, the yolk of which was spiked with 74 kBq of 14C-octanoic acid sodium salt. The meal was ingested within 10 min, immediately followed by 150 ml of water spiked with 100 mg of [1-13C]-glycine. The total caloric value of the test meal was 250 kcal. Breath samples were taken before the meal and at 15-min intervals for a period of 240 min postprandially. Gastric half-emptying time (t1/2) was calculated as previously described.12–15 Delayed emptying was defined as t1/2 above the 95% confidence interval (CI) in healthy volunteers (>74 min for liquids and >109 min for solids).12–15
Barostat studies
All patients underwent a gastric barostat study, within 4 weeks of gastric emptying measurement, to assess sensitivity to gastric distension and meal-induced accommodation. After an overnight fast of at least 12 h, a double lumen polyvinyl tube (Salem sump tube 14 Ch, Sherwood Medical, Petit Rechain, Belgium) with an adherent, finely folded plastic bag (1200 ml capacity, 17 cm maximal diameter) was introduced through the mouth and secured to the patient’s chin with adhesive tape. The position of the bag in the gastric fundus was checked fluoroscopically.
The polyvinyl tube was then connected to a programmable barostat device (Synectics Visceral Stimulator, Stockholm, Sweden). To unfold the bag, it was inflated with a fixed volume of 300 ml of air for 2 min with the study patient in a recumbent position, and again deflated completely. The patients were then positioned in a comfortable sitting position with the knees bent (80°) and the trunk upright in a specifically designed bed. After a 30-min adaptation period, the minimal distending pressure (MDP) was first determined by increasing the intrabag pressure by 1 mm Hg every 3 min until a volume of ⩾30 ml was reached.13 This pressure level equilibrates the intra-abdominal pressure. Subsequently, isobaric distensions were performed in stepwise increments of 2 mm Hg starting from MDP, each lasting for 2 min, while the corresponding intragastric volume was recorded. Patients were instructed to score their perception of upper abdominal sensations at the end of every distending step, using a graphic rating scale that combined oral descriptors on a scale graded 0–6.16 The end point of each sequence of distensions was established at an intrabag volume of 1000 ml, or when the patients reported discomfort or pain (scores 5 or 6).
After a 30-min adaptation period with the bag completely deflated, the pressure level was set at MDP with 2 mm Hg during at least 90 min. After 30 min, a standardised liquid meal (200 ml, 300 kcal, 13% proteins, 48% carbohydrates, 39% Nutridrink, Nutricia, Bornem, Belgium) was given. In all patients, gastric tone measurement was continued for at least 60 min after the meal.
Data analysis
A symptom-severity score was constructed by adding the intensities of all eight dyspeptic symptoms obtained in the questionnaire (maximum score of 24). This score was increased by 1 for every 5% of body weight lost since the onset of symptoms.
Gastric tone before and after the meal was measured by calculating the mean balloon volume for consecutive 5-min intervals. The meal-induced gastric relaxation was quantified as the difference between the average volumes during 30 min before and 60 min after the meal. Impaired accommodation to a meal was defined as a meal-induced relaxation below the mean – 2SD in healthy volunteers (<64 ml).10
In the gastric sensitivity studies, for each 2-min distending period, the intragastric volume was calculated by averaging the recording. Pressure–volume curves were obtained from the stepwise distensions. Gastric compliance was calculated as the slope of the pressure–volume curve obtained during the stepwise isobaric distensions. The perception threshold was defined as the first level of pressure and the corresponding volume that evoked a perception score of ⩾1. Discomfort threshold was defined as the first level of pressure and the corresponding volume that provoked a score of ⩾5. Pressure thresholds were expressed as pressures relative to MDP. Hypersensitivity to gastric distension was defined as a distending pressure inducing discomfort below the mean – 2SD in healthy volunteers (<6.6 mm Hg).11
Statistical analysis
Demographic characteristics, barostat parameters and symptom pattern were compared at two different cut-offs, multiples of the upper limit of normal solid gastric-emptying rate (up to 1.5 and 2 times). The same parameters were compared in patients with and without impaired accommodation, and in patients with or without hypersensitivity to gastric distension. Demographic variables, thresholds to gastric distension, gastric compliance and gastric accommodation were compared using Student’s t test. The prevalence of dyspeptic symptoms and sex distribution in patient groups were compared by χ2 tests. Linear correlation analysis was used to study the relationship between the symptom-severity score and demographic and pathophysiological variables. Differences were considered to be significant at the 5% level. All data are given as mean (standard error of mean (SEM)).
RESULTS
Patient selection and characteristics
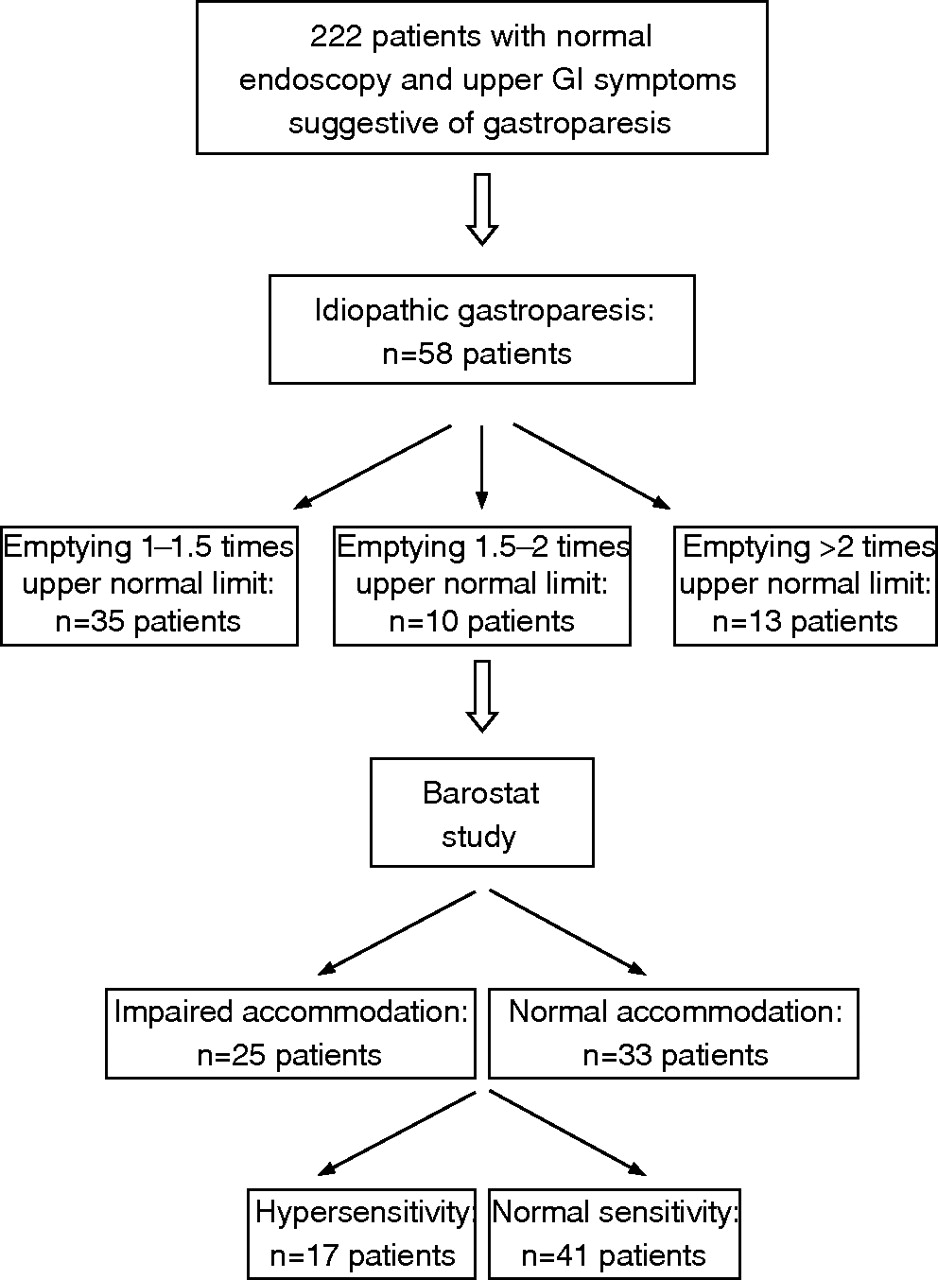
Of a total of 222 screened consecutive patients, 58 (19 men, mean (SD) age 41 (2) years) with severely delayed solid emptying (t1/2 >109 min) and without structural abnormalities were eligible for the study (fig 1). We have previously shown the reproducibility of severely delayed gastric emptying in this patient population.9 In this population, a chart review shows that an average (SD) of 2.2 (0.1) gastric emptying studies had been performed in these 58 patients, which resulted in severely delayed emptying in 1.9 (0.1) studies (91%), and with a mean (SD) interval between two studies of 18.1 (3.5) months. Figure 2 summarises the prevalence of individual symptoms among the patients with idiopathic gastroparesis. Fullness and bloating were the most prevalent symptoms, present in, respectively, 97% and 90% of the patients. Nausea (79%), early satiety (72%) and pain (71%) were also reported often. Epigastric burning, belching and vomiting were present in, respectively, 62%, 57% and 41% of the patients. Weight loss in excess of 5% of the original body weight was observed in 28 (48%) patients. In accordance with the selection of patients with idiopathic gastroparesis, the prevalence of nausea and vomiting is clearly higher in this study population compared with previous reports on patients with functional dyspepsia from our group.10,11,14 Only 8 (14%) patients were H pylori positive.

Selection of patients for this study. GI, gastrointestinal.
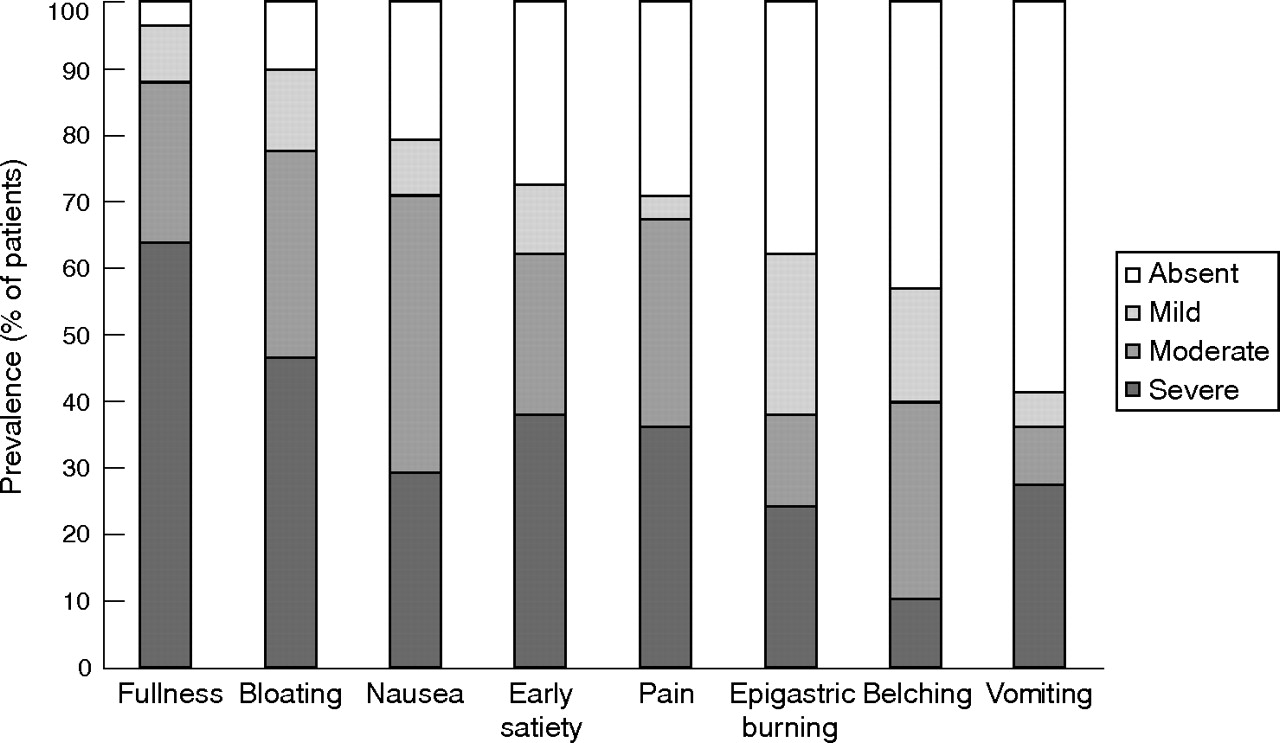
Symptom pattern in 58 patients with idiopathic gastroparesis recruited for this study.
Demographic, symptomatic and pathophysiological characteristics of patients with gastroparesis at two different cut-offs of delayed gastric emptying
In all, 23 (40%) and 13 (22%) patients with idiopathic gastroparesis had a solid gastric t1/2 that was >1.5 or >2 times the upper limit of normal. As summarised in tables 1 and 2, demographic characteristics did not differ significantly between patients with gastroparesis at these different cut-offs. Figure 3 summarises the prevalence of each of the abdominal symptoms at the two different cut-offs. No major difference in symptom pattern was found when using cut-offs of 1.5 and 2 times the upper limit of normal gastric emptying.
Demographic characteristics and barostat findings in patients with idiopathic gastroparesis with delayed gastric emptying 1–1.5 times the upper limit and >1.5 times the upper limit of normal emptying rate
Demographic characteristics and barostat findings in patients with idiopathic gastroparesis with delayed gastric emptying 1–2 times the upper limit and >2 times the upper limit of normal emptying rate

(A) Prevalence of symptoms in patients with gastroparesis with delayed gastric emptying >1.5 times the upper limit of normal (n = 23) compared with those with delayed gastric emptying <1.5 times the upper limit of normal (n = 35). (B) Prevalence of symptoms in patients with gastroparesis with delayed gastric emptying >2 times the upper limit of normal (n = 13) compared with those with delayed gastric emptying <2 times the upper limit of normal (n = 45).
During gastric barostat testing, patients with more delayed gastric emptying had lower intragastric balloon volumes, both at the pressure inducing discomfort, and postprandially during the measurement of meal-induced gastric accommodation (tables 1 and 2).
Demographic, symptomatic and pathophysiological characteristics of patients with gastroparesis with or without impaired accommodation
In all, 25 (43%) patients with idiopathic gastroparesis had impaired gastric accommodation. As summarised in table 3, demographic characteristics, sensitivity to gastric distension and gastric compliance did not differ significantly in patients with gastroparesis with or without impaired accommodation. The presence of relevant or severe early satiety was significantly higher in patients with idiopathic gastroparesis and impaired accommodation (23/25 v 13/33, p<0.005; fig 4). Weight loss in excess of 5% of the original body weight was also significantly more prevalent in patients with gastroparesis with impaired accommodation (17/25 v 11/33, p = 0.009). The prevalence of other symptoms did not differ significantly between patients with gastroparesis with or without impaired accommodation.
Demographic characteristics and barostat findings in patients with idiopathic gastroparesis with or without impaired accommodation

Symptom pattern in patients with idiopathic gastroparesis, with (n = 25) or without (n = 33) impaired accommodation. Early satiety and weight loss >5% of original body weight were significantly more prevalent in patients with impaired accommodation. *p<0.05.
Demographic, symptomatic and pathophysiological characteristics of patients with gastroparesis with or without hypersensitivity to gastric distension
In all, 17 (29%) patients with idiopathic gastroparesis had hypersensitivity to gastric distension. As summarised in table 4, demographic variables were not significantly different in patients with gastroparesis with or without hypersensitivity to gastric distension. In patients with gastroparesis with hypersensitivity to gastric distension, intragastric balloon volume at discomfort, postprandial volume and meal-induced accommodation were significantly lower than in patients without hypersensitivity.
Demographic characteristics and barostat findings in patients with idiopathic gastroparesis with or without hypersensitivity to gastric distension
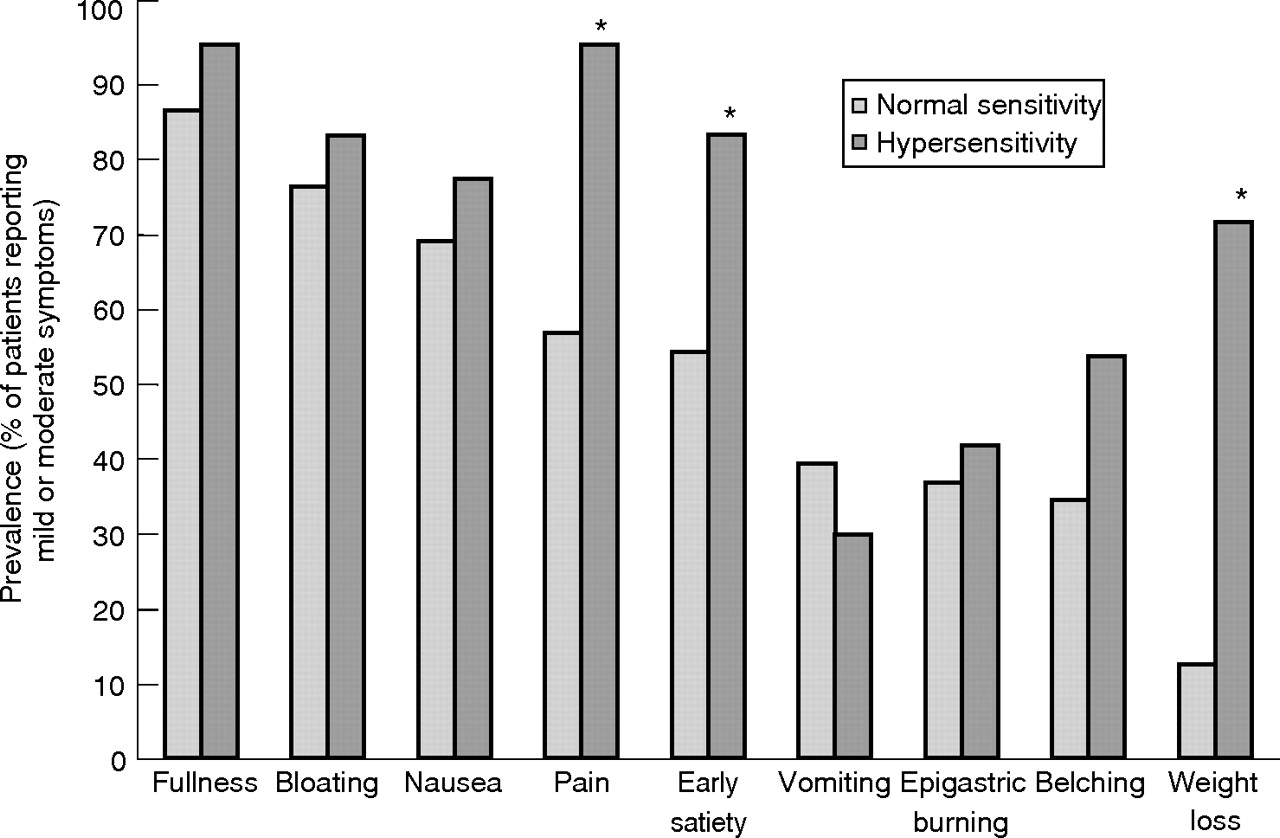
The presence of relevant or severe pain (16/17 v 23/41, p = 0.005) and early satiety (14/17 v 22/41, p = 0.04) was significantly higher in the patients with gastroparesis and hypersensitivity (fig 5). Weight loss in excess of 5% of the original body weight was also significantly prevalent in patients with gastroparesis with hypersensitivity (12/17 v 5/41, p<0.005). The prevalence of other symptoms did not differ significantly between patients with or without hypersensitivity to gastric distension.

Symptom pattern in patients with idiopathic gastroparesis, with (n = 17) or without (n = 41) hypersensitivity to gastric distension. Pain, early satiety and weight loss >5% of the original body weight were significantly more prevalent in patients hypersensitivity. *p<0.05.
Determinants of symptom-severity score
Figure 6 illustrates the correlations between symptom severity and solid t1/2 or discomfort pressure threshold. No significant correlation was found between the symptom-severity score and sex, age, solid or liquid t1/2, barostat volume thresholds, perception pressure, gastric compliance, and preprandial or postprandial volumes. Significant negative correlations were found between the symptom-severity score and body weight (R = −0.4233, p = 0.001) and the intraballoon pressure needed to induce discomfort (R = −0.3898, p = 0.003). These significances were still present when weight loss was omitted from the symptom-severity score calculation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Correlation of symptom-severity score with gastric solid half-emptying time in 58 patients with idiopathic gastroparesis. No significant correlation was obtained between both variables. (B) Correlation of symptom-severity score with barostat pressure needed to induce discomfort in 58 patients with idiopathic gastroparesis. A highly significant correlation was obtained (R = −0.3898, p = 0.003). The solid line depicts the linear regression model. MDP, minimal distending pressure.
DISCUSSION
Delayed gastric emptying is traditionally considered the major pathophysiological mechanism underlying symptoms in patients with idiopathic gastroparesis, and in patients with functional dyspepsia with delayed gastric emptying.1–3 Several studies investigating the relationship between delayed emptying and symptoms, with or without prokinetic therapy, have failed to establish a convincing relationship between delayed gastric emptying and symptom severity.3–9 We selected patients with established severe delay in gastric emptying rates on repeated gastric emptying testing. Previous studies have confirmed that this is associated with high prevalences of signs of neuromuscular dysfunction on antral manometry, including antral hypomotility and absence of normal interdigestive motility patterns.17,18 Using two different cut-offs, multiples of the upper limit of normal gastric emptying, we were unable to show a significant change in symptom pattern with increasing severity of the delay in gastric emptying. We also failed to find a significant association between the symptom-severity score and the delay in gastric emptying. These results are in accordance with a recent preliminary report, which showed that a change in symptom pattern occurred only with extremely delayed gastric emptying (>3 times the upper limit of normal).19 We could argue that the lack of correlation between delayed gastric emptying and symptom pattern was due to the relatively small number of patients, compared with some previous studies involving gastric emptying.4,14 However, the sample size was large enough to show significant correlations between proximal stomach dysfunction and symptom pattern, as described later.
These observations, and several previous reports that changes in gastric-emptying time correlate poorly with the symptomatic response to prokinetic therapy,5–9 prompted us to investigate the contribution of a different pathophysiological mechanism. Recently, evidence has accumulated that proximal stomach dysfunction may contribute to symptom generation, at least in functional dyspepsia.10,11 Using a barostat to evaluate the proximal stomach function in patients with idiopathic gastroparesis, we obtained evidence of a relationship between proximal stomach dysfunction and the symptom pattern in these patients.
Abnormalities of proximal stomach sensorimotor function were quite common, as we found impaired gastric accommodation in 43% and hypersensitivity to gastric distension in 29% of the patients with idiopathic gastroparesis. In these patients, impaired accommodation was associated with a higher prevalence of early satiety and weight loss, and hypersensitivity to gastric distension was associated with higher prevalences of pain, early satiety and weight loss. These findings are reminiscent of findings in patients with functional dyspepsia, not selected on the basis of delayed gastric emptying.10,11 It has often been suggested that the proximal stomach in gastroparesis behaves as a hypotonic, flaccid pouch with reduced distensibility.20,21 This notion is not supported by the fasting gastric compliance and intraballoon volumes measured in the present gastric barostat studies, which are similar to values obtained in health.10,11 In fact, proximal stomach volumes were lower in those patients who had more severely delayed emptying.
Of all putative pathophysiological mechanisms considered in this study, we did not find a significant association between the symptom-severity score and gastric emptying rates or gastric accommodation, but enhanced sensitivity to gastric distension was strongly correlated with the symptom-severity score. This observation may be particularly important when considering pharmacotherapy to improve symptoms in patients with gastroparesis. Traditionally, drug development has focused on enhancement of gastric emptying,1–3,8 but this approach has failed to establish a strong relationship between improvement in gastric emptying and the symptomatic response to prokinetics,3,5–9 and there are several negative or even opposite observations.5,6,9 This study shows that impaired accommodation and, especially, hypersensitivity to gastric distension are determinants of the symptom pattern and symptom severity. Depending on their pharmacological profile, gastroprokinetics may inhibit22–24 or enhance25,26 gastric accommodation. Some prokinetics may also enhance phasic contractility of the proximal stomach.24,27 Recently, we showed that activation of tension mechanoreceptors in the proximal stomach may contribute to the generation of upper gastrointestinal symptom.27,28 Given the observed relevance of impaired accommodation and hypersensitivity to gastric distension to the symptom pattern and symptom severity in idiopathic gastroparesis, gastroprokinetic drugs should preferably not interfere with gastric accommodation and avoid activation of tension-sensitive mechanoreceptors in the proximal stomach.
In this study, the same cut-off for abnormal delayed gastric emptying was used for male and female patients. Several studies in the literature have reported slower gastric emptying rates for healthy women compared with healthy men, suggesting the need for higher upper limits of normal emptying when assessing gastric emptying in female patients.29,30 However, in an extensive study of healthy volunteers and patients with dyspepsia, establishing the normal ranges that were used in this study, no sex-related differences were found for t1/2 or lag time, for both patients and controls.15 Gastric emptying rate in female patients may vary according to the phases of the menstrual cycle, although this was not confirmed in all studies.31–34 Conceivably, the lack of stratification for the phase of the menstrual cycle in the present and the normal range-establishing study15 contribute to the absence of sex-related effects.
In conclusion, we showed that in patients with idiopathic severely delayed gastric emptying, symptom pattern and symptom severity are determined by coexisting proximal stomach dysfunction rather than by the severity of delayed emptying. In patients with idiopathic severely delayed gastric emptying, impaired accommodation is associated with symptoms of early satiety and weight loss, and hypersensitivity to gastric distension with symptoms of pain, early satiety and weight loss.
REFERENCES
Footnotes
-
Published Online First 13 July 2006
-
Competing interests: None.