Article Text

Abstract
Positron emission tomography (PET) is a powerful imaging technique which enables in vivo examination of brain functions. It allows non-invasive quantification of cerebral blood flow, metabolism, and receptor binding. In the past PET has been employed mainly in the research setting due to the relatively high costs and complexity of the support infrastructure, such as cyclotrons, PET scanners, and radiochemistry laboratories. In recent years, because of advancements in technology and proliferation of PET scanners, PET is being increasingly used in clinical neurology to improve our understanding of disease pathogenesis, to aid with diagnosis, and to monitor disease progression and response to treatment. This article aims to provide an overview of the principles of PET and its applications to clinical neurology.
- functional imaging
- neurology
- PET
- positron emission tomography
- AD, Alzheimer’s disease
- CBD, corticobasal degeneration
- DBS, deep-brain stimulation
- DLB, dementia with Lewy bodies
- 18FDG, 18F-2-deoxyglucose
- 18F-dopa, 18F-6-Fluorodopa
- FMZ, flumazenil
- GABA, γ-aminobutyric acid
- GP, globus pallidus
- HD, Huntington’s disease
- LORs, lines of response
- MSA, multiple system atrophy
- PD, Parkinson’s disease
- PET, positron emission tomography
- POp pars opercularis
- PSP, progressive supranuclear palsy
- SMA, supplementary motor area
- STN, subthalamic nucleus
Statistics from Altmetric.com
- AD, Alzheimer’s disease
- CBD, corticobasal degeneration
- DBS, deep-brain stimulation
- DLB, dementia with Lewy bodies
- 18FDG, 18F-2-deoxyglucose
- 18F-dopa, 18F-6-Fluorodopa
- FMZ, flumazenil
- GABA, γ-aminobutyric acid
- GP, globus pallidus
- HD, Huntington’s disease
- LORs, lines of response
- MSA, multiple system atrophy
- PD, Parkinson’s disease
- PET, positron emission tomography
- POp pars opercularis
- PSP, progressive supranuclear palsy
- SMA, supplementary motor area
- STN, subthalamic nucleus
PRINCIPLES OF PET
Positron emission tomography (PET) involves introduction, usually via an intravenous injection, of a radioactive tracer into the human body. A tracer is essentially a biological compound of interest labelled with a positron emitting isotope, such as 11C, 18F, and 15O. These isotopes are used because they have relatively short half-lives (minutes to less than two hours), allowing the tracers to reach equilibrium in the body, but without exposing the subjects to prolonged periods of radiation.
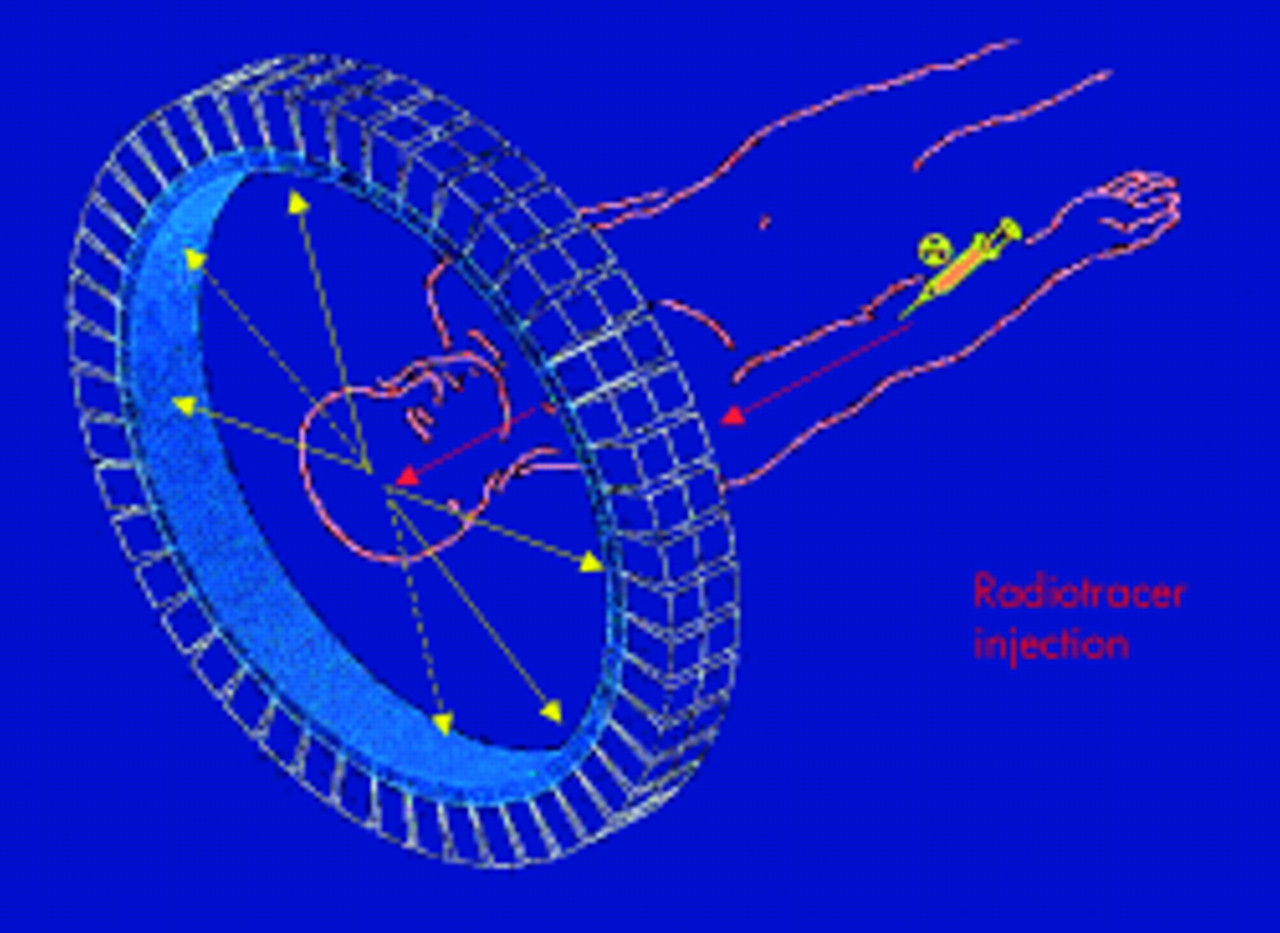
The cyclotron accelerates a beam of protons using two high voltage electrodes and directs it towards the target nuclei, thereby incorporating an extra proton into them. This generates new isotopes with a neutron-to-proton ratio that is energetically unstable. The isotopes are then coupled to the compound of interest—that is, the tracer. Most of these unstable isotopes undergo a process of decay whereby the excess proton is converted into a neutron, a positron, and a neutrino. A positron is similar to an electron, except that it carries a positive charge. The emitted positron travels up to a range of a few millimetres in tissue before being annihilated along with an electron from the surroundings. This mutual annihilation process produces two photons of equal energy (511 keV) travelling in opposite directions. PET scanners contain several rings of scintillation detectors, usually made of bismuth germanate (BGO). The pair of photons produced from a single annihilation will register almost simultaneously on opposing pairs of BGO detectors as a “coincidence event”. The paths of these two photons, called lines of response (LORs), can thus be traced (fig 1). The rings of BGO detectors register thousands of coincidence events emitted from the subject per second. The data gathered from the coincidence events and LORs are used to determine the source of positron annihilation at a given time. These are then converted into a tomographic image using standard reconstruction software.1

Schematic representation of detectors in a tomograph, and the annihilation of a positron with an electron and the resulting pair of 511 keV γ rays released at 180° (yellow arrows).
Acquisition of data in the three dimensional mode using a state-of-the-art scanner greatly increases the spatial resolution of PET images.2 The improved signal-to-noise ratio and the accompanying enhanced sensitivity of three dimensional scanners also allow a lower effective dose of radiation to be administered to subjects (typically 1–5 mSv per scan at our centre compared with around 4 mSv administered in a head computed tomography (CT) scan). PET images taken with most modern scanners have a reconstructed spatial resolution of about 4 mm. Coregistration of PET images to high resolution magnetic resonance images (MRI) enables the accurate anatomical localisation of functional changes displayed on PET.
For full quantification of the acquired PET data, it is necessary to make certain corrections. The photons or γ rays generated by the positron annihilation process, especially those originating from the centre of the brain, may be attenuated by the tissue before reaching the detectors. On an average, about 80% of photon pairs emitted from the centre of the brain will be lost to tissue attenuation.1 This can be overcome by performing a transmission scan using an external positron emitting source before injecting the tracer. The tissue attenuation factor can then be calculated and applied.
The tracer is distributed to various body compartments following administration to the subject. In order to model the kinetics of the tracer accurately, we need to know its plasma concentration (often by continuous arterial blood sampling to obtain arterial input function) and cerebral concentration (from dynamic sequences of PET images) over time, correcting for metabolism and radioactive decay of the compound. However, if a study is undertaken to compare two different groups of subjects or two different conditions, a more qualitative approach can be adopted. For example, there is a negligible number of dopamine receptors in the cerebellum, and hence a dopamine D2 receptor ligand such as 11C-raclopride will not have significant specific binding in the cerebellum. The kinetics of 11C-raclopride in this region will closely resemble those in the plasma. Therefore, the cerebellum can act as a “reference region”, providing tissue input function and obviating the need for invasive arterial cannulation.3 The data can be analysed by defining specific regions of interest on the images if there is an a priori hypothesis regarding expected changes to be observed, or by comparing values throughout the whole brain volume on a voxel-by-voxel basis using statistical parametric mapping.4
Specific tracers are chosen to illustrate the particular brain functions the investigators are interested in. For example, 18F-2-deoxyglucose (18FDG) is used to investigate cerebral glucose metabolism, whereas H215O is used to examine cerebral blood flow. Table 1 lists some of the commonly used tracers and their specific applications. The tracer used usually has very high specific activity (ratio of radioactive to cold compound) such that only a very small amount (in the range of nanomoles to picomoles per gram) is administered. Therefore the tracer will have minimal effect on the subject’s biological system.1
Common PET tracers used to study neurological disorders
PET scans may be carried out at rest, while performing certain tasks or after administration of challenge compounds. Several recent studies have suggested that using the principle of competition between endogenous neurotransmitters and administered tracers for the same neuroreceptors, it is possible to image acute fluctuations in the concentration of synaptic neurotransmitters.5 One of the most commonly performed studies is the 11C-raclopride displacement study. 11C-Raclopride, a competitive reversible ligand, competes with endogenous dopamine for postsynaptic dopamine D2 receptors. According to the classic occupancy model, when there is an increased synaptic release of dopamine after performing a task mediated by dopamine or after administration of a dopamine depleting agent such as methamphetamine, most of the D2 receptors will be occupied by endogenous dopamine. Fewer receptors will be available to 11C-raclopride, and this is evidenced by a reduction in 11C-raclopride binding. Other mechanisms such as receptor internalisation after agonist stimulation may also contribute to the signal change observed.5 Data from a microdialysis study in rhesus monkeys suggest that after administering 0.2 mg/kg of amphetamine, a 1% reduction in striatal 11C-raclopride binding corresponds to at least an 8% increase in striatal extracellular dopamine levels.6 This technique has a significant advantage over H215O activation studies and functional MRI, which are modelled on haemodynamic changes following a task, since a ligand displacement study enables researchers to study the role of a particular neurotransmitter in mediating certain tasks or functions, such as the release of dopamine while performing a goal-directed motor task with a reward.7 Pharmacological challenge using methamphetamine is used to show the ability of the surviving fetal striatal grafts in Parkinson’s disease to release normal levels of dopamine (see section on Movement disorders).
APPLICATION OF PET TO CLINICAL NEUROLOGY
Movement disorders
Dopamine is the key neurotransmitter in the nigro-striatal-pallidal-thalamo-cortical circuit. 18F-6-Fluorodopa (18F-dopa) is one of the most commonly used ligands for studying the dopaminergic system in movement disorders. Following intravenous injection 18F-dopa is taken up by the terminals of dopaminergic neurones and converted to 18F-dopamine by dopa decarboxylase, and subsequently to other dopamine metabolites. The influx constant (Ki) of 18F-dopa reflects dopa transport into the terminals, dopa decarboxylase activity and dopamine storage capacity.818F-dopa PET can therefore provide an in vivo indicator of the function and integrity of presynaptic dopaminergic terminals. Tracers that bind to presynaptic dopamine transporters, such as 11C-methylphenidate, and dopamine terminal vesicle monoamine transporters, such as 11C-dihydrotetrabenazine, have also been developed as markers of presynaptic dopaminergic function.
Differentiating various types of parkinsonian syndromes clinically, especially in the early stages of the disease, can be difficult. Conventional imaging methods such as MRI often do not reveal any abnormality. PET may be employed as an adjunct to clinical diagnosis in equivocal cases. Parkinson’s disease (PD) is characterised by loss of dopaminergic neurones in the pars compacta of the substantia nigra. The greatest loss of neurones is seen in the ventrolateral tier of the pars compacta, with lesser involvement in the dorsomedial tier. Dopaminergic neurones in these regions project to the putamen and head of the caudate nucleus, respectively.9 These changes are detected by 18F-dopa PET, as evidenced by progressive decline in 18F-dopa Ki in the putamen in a caudal-rostral pattern. The biggest decrease is seen in the putamen contralateral to the side with the most severe symptoms. The caudate nucleus is also affected later on.10 Diffuse loss of nigrostriatal dopaminergic projection is seen in multiple system atrophy (MSA) and progressive supranuclear palsy (PSP), as reflected by the symmetrical loss of 18F-dopa signal in the entire striatum (fig 2). Corticobasal degeneration (CBD) shows asymmetric and equivalent reduction in 18F-dopa Ki of the caudate and putamen. 18F-Dopa PET is able to discriminate PD from the striatonigral degeneration form of MSA in 70% of cases and from PSP in 90% of cases11; it is, however, less effective in discriminating between the atypical parkinsonian syndromes.

18F-Dopa PET in a healthy volunteer (normal); in a subject with Parkinson’s disease (PD) showing asymmetrical loss of putaminal 18F-dopa Ki, with relative preservation of the caudate Ki earlier on in the disease; and in a subject with progressive supranuclear palsy (PSP) showing diffuse and symmetrical decrease in striatal Ki.
The various parkinsonian syndromes also exhibit different patterns of cerebral glucose metabolism. 18FDG PET in PD reveals normal or increased glucose metabolism in the striatum but decreased metabolism in temporoparietal areas.12 PSP shows bilateral striatal and frontal hypometabolism, whereas decreases in striatal, brainstem, and cerebellar metabolism are found in MSA. In CBD, there is asymmetric hypometabolism of the striatum, thalamus, frontal and temporoparietal cortices, with the hemisphere contralateral to the most affected limb displaying the greatest reduction. However, 18FDG PET does not provide additional discriminatory information to 18F-dopa PET.10 Table 2 summarises the major PET findings in parkinsonian syndromes.
Summary of positron emission tomography (PET) findings in parkinsonian syndromes
According to current models of basal ganglia connectivity, the internal segment of the globus pallidus (GPi) receives nigrostriatal projections via distinct direct and indirect pathways. In PD, the loss of nigral dopaminergic cells results in loss of inhibitory output to GPi in the direct pathway. In contrast, the inhibitory striatal output to the external segment of globus pallidus (GPe) becomes overactive in the indirect pathway. This, in turn, causes a reduction of inhibitory output from GPe to the subthalamic nucleus (STN). There is, therefore, increased excitatory activity from the STN to the GPi, and the consequence of all this is that the GPi, which provides major inhibitory output to the ventral thalamus, becomes disinhibited or overactive. Consequently, there is a reduction of excitatory projections from the ventral thalamus to the supplementary motor area (SMA) and prefrontal cortex,13 both of which are involved in motor planning and preparation. It has been proposed that their underactivation in PD results in hypokinetic symptoms such as akinesia. This model has been supported by H215O activation studies of PD patients performing paced joystick movements in freely chosen directions. Decreased cerebral blood flow in the SMA and prefrontal cortex compared with controls improved after subcutaneous administration of apomorphine, a dopamine D1 and D2 receptor agonist, with concomitant reduction in the subjects’ akinesia.14
Surgical treatments for advanced PD with motor complications have been developed on the basis of the above understanding of basal ganglia circuitry. The aim of these treatments is to reduce inhibitory output from the GPi to the ventral thalamus, either directly by deactivating GPi or indirectly by deactivating STN, thereby reducing its excitatory output to GPi. This can be accomplished structurally by stereotactic thermocoagulation (for example medial pallidotomy) or functionally using high frequency electrical deep-brain stimulation (DBS), which causes a depolarising conduction block. The advantages of the latter are that it is reversible, and the frequency of electrical stimulation can be adjusted according to patient’s response. However, it does require insertion of electrodes into appropriate targets with the accompanying surgical and infectious risks. Several randomised controlled trials have shown the efficacy of these techniques in improving “off” medication motor function and “on” medication dyskinesia in advanced PD.15,16 As predicted, H215O activation studies of PD patients following STN DBS or medial pallidotomy showed improvement in SMA and prefrontal cortex activation when performing paced joystick movements in freely chosen directions.17,18
PET has been developed as a biological marker of disease severity and progression in PD. Striatal 18F-dopa Ki is shown to correlate with postmortem dopaminergic cell density in the substantia nigra.19 The reduction in putaminal Ki in PD also correlates with cross-sectional motor disability.20 A longitudinal progression study of PD found a 9–12% annual decline in putaminal dopa Ki.21
Several neuroprotective/restorative trials have used 18F-dopa PET as a biological marker of response to treatment. The clinical improvement seen in PD patients receiving human fetal neural transplantation and intraputaminal infusion of glial cell line derived neurotrophic factor is accompanied by increases in striatal dopa Ki.22–24 At the postmortem examination of two PD patients with transplants, who died of unrelated causes, increased striatal 18F-dopa uptake was associated with the survival of grafts and dopaminergic reinnervation of the striatum.25 “Off” phases dyskinetic involuntary movements observed in some PD patients following transplantation procedures are not associated with abnormal increases in 18F-dopa uptake indicating that this side effect does not result from excessive growth of grafted dopaminergic neurones.26,27
H215O activation scans of four PD patients 18 months after receiving bilateral fetal transplantation showed restoration of premotor and prefrontal activation whilst performing a paced motor task, suggesting functional integration of the grafts into host neuronal circuitry.28 In one PD patient who had sustained clinical improvement 10 years after unilateral fetal striatal implantation, the implanted striatum exhibited normal levels of basal and methamphetamine induced dopamine release as evidenced by his 11C-raclopride PET displacement study.29
PET has also been widely used to study hyperkinetic movement disorders. Huntington’s disease (HD) is an autosomal dominant disorder arising from expanded CAG repeats in the IT15 gene on chromosome 4. Medium spiny neurones in the striatum, which express dopamine D1 and D2 receptors, bear the brunt of HD pathology and are progressively lost. Using 11C-SCH23390 and 11C-raclopride PET, parallel reduction in striatal D1 and D2 receptor binding was found in HD patients.30 Striatal D2 binding decreases by approximately 5% per year in HD, and the reduction correlates with the duration and clinical severity of the disease.3118FDG PET showed striatal glucose hypometabolism in HD, with the cortex becoming progressively involved with increasing severity of disease, reflecting the widespread nature of HD pathology.3211C-Raclopride and 18FDG PET have both been used as markers of graft survival in HD fetal striatal transplantation trials. One recent study reported increased striatal glucose metabolism in HD patients who experienced clinical improvement following bilateral striatal implantation but not in those without any clinical improvement, suggesting such improvement can be attributed to the surviving grafts.33
Although HD can be diagnosed accurately using genetic tests, there is, as yet, no reliable way to predict disease onset in presymptomatic carriers. Several PET studies have found reduced striatal D2 binding and glucose metabolism in some HD carriers.34,35 Larger trials are ongoing to ascertain the accuracy of PET in identifying carriers nearing the onset of disease, since intervention at this early stage with putative neuroprotective agents such as minocycline and riluzole may be of greater benefit than treatment in later stages.
Striatal D2 receptor binding and glucose metabolism are also reduced in chorea due to other degenerative conditions (for example neuroacanthocytosis), but are preserved in non-degenerative chorea (for example systemic lupus erythematosus, Sydenham’s chorea).36
Epilepsy
Complex partial seizures in a significant proportion of patients remain uncontrolled despite optimal medical therapy. Surgical removal of epileptogenic foci in partial seizures such as intractable temporal lobe epilepsy results in significant improvement in control of the seizures and the quality of life.37 Modern MRI is able to identify the source of the seizure in the majority of patients with partial seizures. However, 20–30% of potential surgical candidates with focal epilepsy have normal MRI.38 These patients are also less likely to become seizure free if they do undergo epilepsy surgery.39 Microscopic structural abnormalities, which may only be evident on histological examination, may not be detected on MRI.40 The main clinical uses of PET in epilepsy are localisation of epileptogenic foci in potential surgical candidates with partial seizures and corroborating findings from other investigational modalities such as electroencephalography (EEG).
In partial seizures, there is an increase in glucose metabolism and cerebral blood flow in the region of the epileptogenic focus during the ictal period.41 Post-ictally, the hyperperfusion gradually returns to baseline, but the glucose metabolism remains elevated for another 24–48 hours after the seizure.42 Interictal PET shows decreased glucose metabolism and blood flow in the epileptogenic focus. It is important to perform PET with concomitant scalp EEG recordings to correlate the PET findings with the clinical status of the patient. Interictal studies in patients with temporal lobe epilepsy using 18FDG PET have found a 60–90% incidence of temporal lobe hypometabolism.38 However, the area with abnormal cerebral blood flow and metabolism seen on PET is considerably larger than the actual structural abnormality, possibly due to reduced synaptic inhibition or deafferentation of neighbouring neurones in areas of epileptic propagation.38 Therefore, false localisations may occur, the probability of which can be lessened by using quantitative rather than qualitative assessment of regional cerebral metabolism. Overall, for epileptogenic foci 18FDG PET may be more suitable as a lateralising rather than localising tool.
γ-Aminobutyric acid (GABA) is the principal inhibitory neurotransmitter in the brain, acting at up to 40% of synapses. A decreased number of GABAergic inhibitory interneurones was found in epileptogenic cortex.43 Flumazenil (FMZ) is a specific reversible antagonist that binds to the benzodiazepine binding site of the GABAA–central benzodiazepine receptor complex. 11C-FMZ PET therefore provides an in vivo marker of GABAA receptor binding.4411C-FMZ binding is reduced by 30% in epileptogenic foci.45 An autoradiographic and histopathological study of sclerotic hippocampi revealed that the decreased 11C-FMZ binding is due to reduced number of neurones and decreased density of central benzodiazepine receptors per neurone.46 There is also a good correlation between quantitative in vivo hippocampal 11C-FMZ PET and ex vivo 3H-FMZ autoradiographic studies in individual patients with hippocampal sclerosis.47 One study examined 100 patients with partial seizures who had undergone presurgical evaluation including 18FDG and 11C-FMZ PET. The latter demonstrated abnormalities in 94% of the patients with temporal lobe epilepsy. 11C-FMZ abnormality coincided with MRI abnormality in 81% of the cases. The area with abnormal 11C-FMZ binding is usually smaller than that seen on 18FDG PET but larger than the abnormality detected on MRI.48 This suggests that the area of neuronal loss is more circumscribed than the region with reduced metabolism. Another study which examined the focus localising abilities of 11C-FMZ and 18FDG PET, using extra- and intracranial EEG recordings as reference, found the former to be more sensitive and accurate.49
Hammers et al investigated 18 patients with refractory temporal lobe epilepsy and normal MRI using 11C-FMZ PET. Sixteen patients showed abnormalities in temporal lobe 11C-FMZ binding, in seven of whom the findings were concordant with clinical and EEG data50 (fig 3). Three patients subsequently underwent anterior temporal lobe resection with significant clinical improvement. Neuropathological findings from the surgical specimens from these patients suggest that some of the abnormalities seen on 11C-FMZ PET are likely to be due to microdysgenesis, which is not often detected even with optimal MRI.

{kind=link}
{kind=link}
{kind=link}
Comparison of 18FDG PET (A) and 11C-FMZ PET (B) in a 28 year-old patient with complex partial seizures, interictal left temporal epileptiform discharges and left temporal seizure onset on video telemetry. MRI including T1 weighted and T2 weighted images, FLAIR and quantitative hippocampal volumetry and T2 mapping was normal. (A) 18FDG PET shows extensive hypometabolism in the left temporal lobe, affecting both the medial temporal cortex (arrow) as well as the inferior and lateral (double arrow) temporal neocortex. (B) 11C-FMZ-PET shows a circumscribed decrease of 11C-FMZ volume-of-distribution (Vd) in the left medial temporal lobe (arrow). (C) Statistical analysis with statistical parametric mapping (SPM99) localised a significant decrease of FMZ-Vd in the left anterior hippocampus, compared with 21 controls. The statistical map is overlaid on the patient’s own MRI; the colour scale shows the t-value. (Images courtesy of A Hammers.)
PET may reduce the need for invasive EEG as part of the preoperative localisation of surgical targets in the future. Some centres have proposed using PET as a routine preoperative evaluation tool for patients undergoing epilepsy surgery. However, PET does not provide additional information if the MRI has identified the obvious cause of the epilepsy, such as hippocampal sclerosis.51 Therefore, PET is likely to be most useful in situations where MRI is equivocal or normal.
PET is less useful clinically for primary generalised seizures. During seizures there is a global increase in cerebral glucose metabolism, but the interictal pattern is usually normal.38
Brain tumours
Tumour cells, especially of higher histological grades, typically have increased metabolic and mitotic rates compared with normal brain tissue. 18FDG PET can provide important prognostic information as increased glucose metabolism of gliomas correlates with higher histological grades (III and IV) and shorter survival period.52,53 It can also detect transformation of low grade glioma into a high grade variety.54 The information obtained may influence the choice of the therapeutic approach. Response to chemotherapy and radiotherapy is associated with a significant reduction in tumour glucose metabolism.55,56 Therefore, 18FDG PET may provide an objective subclinical evidence of response to treatment. The European Organization for Research and Treatment of Cancer PET Study Group recommends that a reduction of 15–25% in glucose uptake after one cycle of chemotherapy would be classified as partial metabolic response; a complete metabolic response occurs when there is complete resolution of glucose uptake within the tumour volume so that it is indistinguishable from surrounding normal tissue.57 However, there is often a transient increase in tumour glucose uptake within 24 hours of treatment, which is not present in studies done 7–14 days after treatment.56,58 Therefore, a one to two week post-treatment interval is recommended prior to performing 18FDG PET to accurately assess response to treatment.57 Increased glucose metabolism in recurrent cerebral glioma can help differentiate it from post radiotherapy changes that may be indistinguishable with conventional imaging techniques such as CT or MRI.59,60
Similarly, increased uptake of 11C-methionine, which reflects cellular amino acid uptake, is indicative of high grade glioma and poorer survival.6111C-Methionine is useful for discriminating between recurrences of local or metastatic tumours and radiation induced changes. In one recent study, 11C-methionine PET had a sensitivity of 77.8% and specificity of 100% for differentiating recurrence of metastatic brain tumours from post radiotherapy changes.62 However, 11C-methionine uptake may also be elevated in other conditions where there is a disruption of the blood–brain barrier, such as cerebral haematoma or even necrotic areas caused by radiotherapy,63 whereas glucose metabolism may be normal or low in lower grade tumours compared with surrounding cortex. Combined use of 11C-methionine and 18FDG PET enhances the accuracy of discrimination between recurrent tumour and post radiotherapy changes.64 The higher glucose metabolism in cerebral lymphoma also helps to distinguish it from cerebral infections (toxoplasmosis and tuberculoma) in patients with AIDS.65,66
Dementia
18FDG PET has been used extensively to study dementia and it may be an effective tool for early diagnosis and differentiation of various types of dementia. Alzheimer’s disease (AD) patients exhibit characteristic temporoparietal glucose hypometabolism. With progression of disease, there may also be frontal involvement.67 The degree of hypometabolism correlates with the severity of dementia,68 The glucose hypometabolism in AD is likely to be due to a combination of neuronal cell loss and decreased synaptic activity.69 In a recent study of 138 patients with symptoms of dementia, which included postmortem histopathological examination, 18FDG PET was able to identify AD with a sensitivity of 94% and specificity of 73%. It could also correctly predict a progressive course of dementia with 91% sensitivity, and a non-progressive course with a specificity of 75%.7018FDG PET has been used to detect subjects at risk for AD even before onset of symptoms. Asymptomatic carriers of the apolipoprotein E type 4 allele, who are at increased risk for familial AD, showed similar pattern of glucose hypometabolism as AD patients.71,72 After a mean follow up of two years, the cortical metabolic abnormality continued to decline despite preservation of cognitive performance.73,74 Entorhinal cortex hypometabolism on 18FDG PET in elderly people with normal cognition can predict the progression to mild cognitive impairment or even AD.75 The identification of asymptomatic individuals at risk could be important should an effective neuroprotective agent that can delay or prevent progression to AD become available in the future.
18FDG PET in dementia with Lewy bodies (DLB) reveals changes similar to those seen in AD, plus additional hypometabolism in the primary and associative visual cortices.76 In a PET study with postmortem confirmatory diagnosis, the antemortem occipital glucose hypometabolism could help distinguish DLB from AD with 90% sensitivity and 80% specificity.7718FDG PET in multi-infarct dementia shows multiple focal areas of hypometabolism, the extent of which is greater than the actual pathology seen on postmortem examination. This is probably due to the degeneration of axons following the infarct with disconnection of remote structures.78,79 Frontotemporal dementia is associated with hypometabolism in the frontal and temporal lobes.79
11C(R)-PK11195 is a selective ligand for the peripheral benzodiazepine binding sites (PBBS). PBBS are present in the normal brain at very low levels, but they are selectively expressed and upregulated by activated microglia. It has been proposed that activated microglia play a role in the pathogenesis of neurodegenerative diseases such as AD by mediating neuroinflammation.8011C(R)-PK11195 PET in AD patients showed increased binding in the entorhinal, temporoparietal and cingulate cortices, corresponding to postmortem distribution of AD pathology.81 The ability to detect microglial activation and neuroinflammatory response in vivo may be deployed to monitor disease activity in the many proposed and ongoing neuroprotective studies in AD using anti-inflammatory agents.80
Despite the characteristic patterns seen in many of the dementia syndromes, there can be considerable overlap in their PET findings. Therefore, PET findings should be interpreted in the context of each individual’s clinical information. Recent efforts to develop a specific ligand for β-amyloid plaques may further enhance the sensitivity of PET for early diagnosis of AD and provide a biological marker of disease progression.82
Stroke and neuronal plasticity
Knowledge acquired from PET cerebral blood flow and metabolism studies has contributed significantly to the development of thrombolysis as a therapeutic approach in ischaemic stroke. Following stroke, PET can identify a “core” region of irreversibly damaged tissue with profoundly depressed cerebral blood flow and metabolism. This core region is surrounded by the “penumbra”, an area of hypoperfused tissue but with relatively normal oxygen consumption, which may yet be salvaged by reperfusion.83 Survival of the penumbra correlates with the degree of recovery after ischaemic stroke.84 The possibility of finding a penumbra and its extent decrease with time since onset of stroke. One study showed that in 90% of patients studied within six hours after onset of stroke, there still was a substantial amount of cortical penumbra. Such findings are detected in about a third of patients even at 5–18 hours after onset.85 The variability in the survival of the penumbra suggests that the therapeutic window for reperfusion strategies may be different for certain subsets of patients, and this should be investigated in future trials of thrombolysis trials.
Results from several PET studies suggest that recruitment of remote areas and functional reorganisation are amongst the mechanisms responsible for the recovery of cerebral functions in adult brains after insults such as stroke. One H215O activation study showed that in patients who recovered from hemiplegic stroke there was bilateral activation of motor cortices when moving the fingers of the affected hand, whereas movement of fingers of the normal hand resulted in the activation of only the contralateral motor cortex and the ipsilateral cerebellum.86 In another study, patients with non-fluent aphasia due to left anterior perisylvian infarction including the left pars opercularis (POp) with subsequent recovery were compared with two control groups: normal subjects and anterior aphasic patients with sparing of the left POp.87 During production of propositional speech, the left POp infarct group showed increased activation of the homotopic right PO when compared with the two control groups. Further understanding of the mechanisms underlying neuroplasticity will help design appropriate strategies for rehabilitation and identify patients who are most likely to benefit from such therapy.
Similar plasticity is seen in neurodegenerative conditions. In PD, there is a decrease of contralateral putaminal 18F-dopa Ki by about 50% before development of symptoms.21 Whone et al showed in early PD a lack of significant clinical progression despite continuing loss of nigrostriatal projections.88 This is probably due to the upregulation of nigropallidal dopaminergic projection to GPi, as evidenced by increased GPi 18F-dopa Ki compared with healthy volunteers, which reduces the inhibitory output from GPi to the thalamus. Such compensatory changes are not seen in more advanced PD with motor complications. This may partially explain why in early PD there is often a good response to dopaminergic medications with little clinical fluctuations. Loss of nigropallidal upregulation may result in alteration of the firing pattern of GPi from tonic to burst firing, heralding the onset of motor complications.
Neuropharmacology
PET receptor ligand studies have generated a wealth of knowledge about disease pathogenesis and potential therapeutic targets for novel pharmaceutical agents. PET offers the opportunity to use an in vivo technique to study the pharmacodynamics and biodistribution of new agents and to ensure they target the organs or compartments of interest—for example, in the case of neuropharmacology, the ability of drug to cross the blood−brain barrier and bind to specific receptors in the brain. The study of drug occupancy can provide information about the occupancy of the binding sites for a particular dose of the drug and its pharmacokinetics. This will help determine optimal drug dosing regimens.89
POTENTIAL FUTURE APPLICATIONS
The UK government has recently announced a plan to increase the number of PET centres in the country for clinical use. The mainstay of clinical application of PET in neurology is likely to be in the domains of epilepsy surgery and neuro-oncology.
Potential future applications include:
-
early diagnosis of brain metastasis; distinguishing local recurrences from radiotherapy induced changes; and detecting malignant transformation of low grade tumours
-
preoperative localisation of seizure foci in potential candidates for epilepsy surgery, especially in those with equivocal MRI findings
-
as an adjunct to clinical diagnosis in atypical cases of parkinsonian syndromes and dementia
-
early and presymptomatic diagnosis of individuals at risk for neurodegenerative disorders such as AD and PD if an effective neuroprotective agent becomes available.
REFERENCES
Footnotes
-
Competing interests: none declared