Article Text

Abstract
Aim: To determine the size of untreated choroidal melanomas resolved by whole body positron emission tomography fused with computed tomography (PET/CT).
Methods: 50 consecutive patients with untreated choroidal melanomas underwent whole body PET/CT. A functionally fused helical CT scan and 18-fluoro-2-deoxyglucose (FDG) PET scans were employed. The tumours were identified (both quantitatively and qualitatively) and compared with clinical measurements derived from ophthalmoscopic, angiographic, and ultrasonographic imaging. Standardised uptake values (SUV) of more than 2.5 were considered positive.
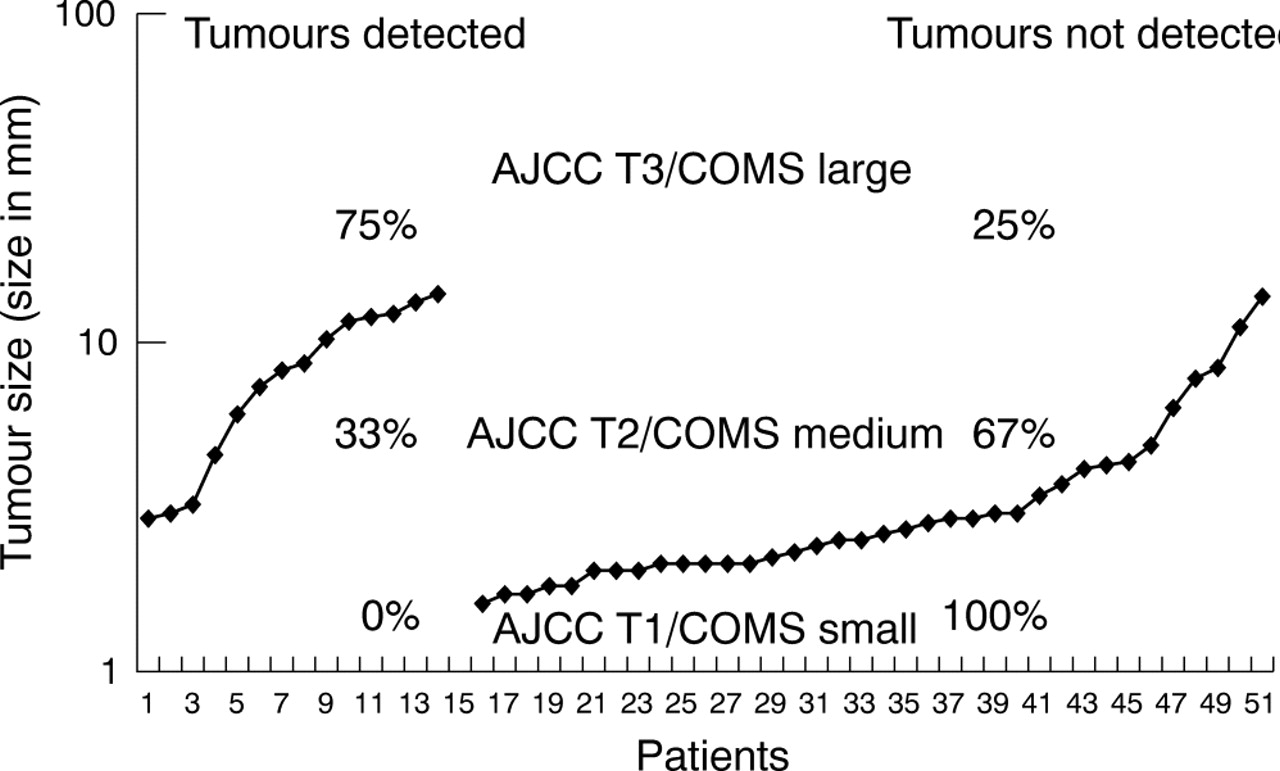
Results: Among the 50 patients with choroidal melanoma, PET/CT scan SUVs of more than 2.5 were noted in 14 (28%) tumours. No AJCC T1 class tumours, 33.3% of T2 melanomas, and 75% of T3 melanomas were physiologically identifiable on PET/CT. With respect to COMS group classifications, no small choroidal tumours, 33% of medium, and 75% of large melanomas were physiologically identifiable. The sole ring melanoma was identifiable on PET/CT imaging. The smallest tumour physiologically identifiable by PET/CT had basal dimensions of 3×5.9 and an apical height of 2.9 mm.
Conclusion: Though PET/CT was found to be capable of physiologically identifying certain medium (T2) and most large sized (T3) choroidal melanomas, physiological imaging was not completely dependent upon tumour size. Functionally fused PET/CT localised the tumours within the eye and assessed their physiological activity.
- AJCC, American Joint Cancer Committee
- BGO, bismuth germanate
- COMS, Collaborative Ocular Melanoma Study
- CT, computed tomography
- FDG, 18-fluoro-2-deoxyglucose
- MRI, magnetic resonance imaging
- PET, positron emission tomography
- SUV, standardised uptake values
- PET
- CT
- choroidal
- uveal
- melanoma
- size
- imaging
- AJCC, American Joint Cancer Committee
- BGO, bismuth germanate
- COMS, Collaborative Ocular Melanoma Study
- CT, computed tomography
- FDG, 18-fluoro-2-deoxyglucose
- MRI, magnetic resonance imaging
- PET, positron emission tomography
- SUV, standardised uptake values
- PET
- CT
- choroidal
- uveal
- melanoma
- size
- imaging
Statistics from Altmetric.com
- AJCC, American Joint Cancer Committee
- BGO, bismuth germanate
- COMS, Collaborative Ocular Melanoma Study
- CT, computed tomography
- FDG, 18-fluoro-2-deoxyglucose
- MRI, magnetic resonance imaging
- PET, positron emission tomography
- SUV, standardised uptake values
- PET
- CT
- choroidal
- uveal
- melanoma
- size
- imaging
- AJCC, American Joint Cancer Committee
- BGO, bismuth germanate
- COMS, Collaborative Ocular Melanoma Study
- CT, computed tomography
- FDG, 18-fluoro-2-deoxyglucose
- MRI, magnetic resonance imaging
- PET, positron emission tomography
- SUV, standardised uptake values
- PET
- CT
- choroidal
- uveal
- melanoma
- size
- imaging
Cancer cells require a great deal of sugar (glucose) for metabolism and growth. Positron emission tomography/computed tomography (PET/CT) scanning utilises a radioactive form of glucose, called 18-fluoro-2-deoxyglucose (FDG) that accumulates within malignant cells because of their high rate of metabolism. The FDG injected patient is imaged on the whole body PET scanner in an effort to reveal tumours that may have been overlooked or difficult to characterise (as benign or malignant) by conventional computed tomography (CT), x ray, or magnetic resonance imaging (MRI).
The CT portion of a PET/CT provides detailed information about the location, size, and shape of tumours but offers less information that can be used to differentiate between cancerous and normal structures (compared to PET). The dual modality, PET/CT scanner fuses an image that puts form and function on the same diagnostic page.
Choroidal melanomas are the most common primary intraocular cancer in adults.1 The Collaborative Ocular Melanoma Study (COMS) group and others have concluded that indirect ophthalmoscopy, combined with ophthalmic ultrasonography and fluorescein angiography, can yield a diagnostic accuracy rate greater than 99%.2 However, strict selection criteria (patient and tumour specific) for COMS eligibility were based on size and. secondly, on appearance, shape, location, internal ultrasonic reflectivity, and angiographic evidence of tumour leakage.2 Though exhaustive, the diagnostic criteria employed by COMS did not include physiological imaging.2
The importance of early detection of malignant melanoma cannot be understated.3–7 Mathematical studies of tumour doubling time and the COMS small tumour trial suggest that metastasis from choroidal melanomas can occur while a small tumour is being observed as a “suspicious choroidal naevus.”4,5 Since COMS found that largest tumour dimension is significantly correlated with the risk of metastasis, it is reasonable to assume that a physiological assessment of tumour metabolism could help differentiate between suspicious choroidal naevi and small choroidal melanomas before growth.2,3
In the last few years PET/CT has emerged as a new imaging modality for the detection and staging of cancer.8 Our study evaluates the efficacy of FDG-PET/CT imaging for the detection of primary choroidal melanomas, to assess their physiological activity and its relationship to tumour size.
METHODS AND MATERIALS
Patients
Since August of 2003, 50 consecutive patients with choroidal melanomas were evaluated by PET/CT before treatment (table 1). All patients had a clinical diagnosis confirmed by ophthalmoscopy, fluorescein angiography, and ophthalmic ultrasonography. Their initial metastatic investigation included liver function tests (γ-glutamyl transpeptidase, aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, bilirubin), a chest x ray and whole body FDG-PET/CT imaging. Informed consent and health insurance portability and accountability act (HIPAA) forms were obtained before treatment.
Patients with uveal melanomas
PET/CT protocol
PET/CT imaging required that patients refrain from eating a carbohydrate based dinner the previous night and to fast 4–6 hours before injection of 18-FDG. This diminished physiological glucose utilisation and reduced insulin serum levels to baseline. The normal fasting glucose level was optimally less than 110 mg/dl, but the acceptable range was 80 mg/dl to 160 mg/dl. The full body PET/CT scan began at the top of the head and ended at the bottom of the feet. The CT portion (General Electric Discovery ST, Piscataway, NJ, USA) with BGO (bismuth germanate) crystal consisted of a multi-detector helical CT scanner. The imaging parameters were 80–140 kV, 40–80 mA, 0.8 s per CT rotation, and a table speed of 33.75 mm/rotation. The CT slice thickness was 3.75 mm with an image interval of 3.27 mm. The CT acquisition came before the PET emission acquisition, and the acquisition time was dependent on the dose of FDG and ranged from 19 seconds to 27 seconds. FDG was injected with a target dose of a 5 mCi (range 10 mCi to 20 mCi). The dose was calculated by (weight in kilograms × target dose in mCi)/70 kg. The FDG was injected via an intravenous line, followed by 10 ml of normal saline. Imaging began within 45 minutes of injection and ended no later than 1.5 hours after injection.
The resolution of the PET scan was 4 mm. The transmission time at each bed position was 2–3 minutes. Eight to nine bed positions were used. After each bed position, a 512 cm × 512 cm CT matrix was converted to a 128 cm × 128 cm matrix that was fed into to the PET scan. The PET scan reconstructed the images on the fly and utilised the CT scan to correct for attenuation. Then, Xeleris (General Electric software, Piscataway, NJ, USA), a computer software, was used to fuse and display the PET and CT images to produce the final image. The images were graded positive when tracer uptake of 2.5 SUV (standardised maximum uptake value) or more was observed in comparison with the surrounding structures. The SUVMAX was calculated for each site using the conventional formula using body weight normalisation:

RESULTS
Fifty patients (22 males and 28 females) with a mean age of 64 years (range 39–95) and a clinical diagnosis of choroidal melanoma underwent full body PET/CT scans (table 1). Our study included 27 melanomas of the left eye and 23 melanomas of the right. One of the melanomas was classified as a ring melanoma, and of the 49 remaining, the mean width, length, and height of the uveal melanomas were 11.16 mm (range 5–19), 9.87 mm (range 3–19.1), and 4.78 mm (range 1.6–14), respectively.
The analysis of PET/CT scans showed tumour uptake in 14 (28%) patients. There were seven males, seven females, and their mean age was 70 years (range 54–95). The mean width of the lesions identified by PET/CT, excluding the ring melanoma, was 14.7 mm (range 5.9–19), the mean length was 13.2 mm (range 3–19.1), and the mean height was 8.1 mm (range 2.9–14). The PET/CT detected none of the American Joint Committee on Cancer (AJCC) T1 staged melanomas (table 2). The PET/CT detected 33% of the AJCC T2 tumours and 75% of the AJCC T3 tumours. No small choroidal tumours (fig 1) as classified by COMS were detected by PET/CT (table 2). Thirty three per cent of medium sized melanomas (fig 2) and 75% of large tumour (fig 3) PET/CT scans showed tumour uptake (figs 4 and 5). The smallest tumour detected by PET/CT imaging was 3×5.9 mm in base and 2.9 mm in height.
PET/CT detection of uveal melanoma (AJCC/COMS classification)

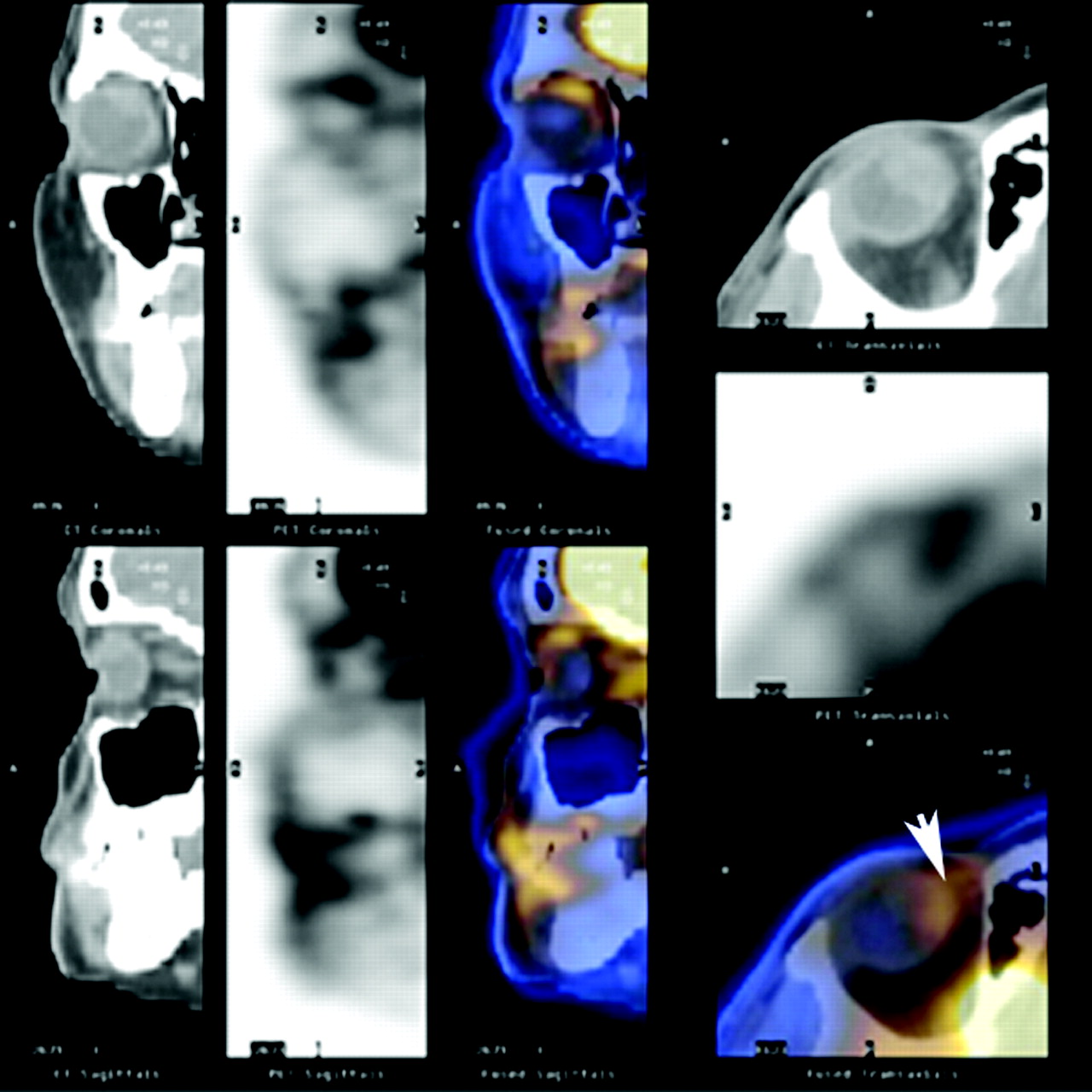
Patient 20. PET/CT image of a patient with an AJCC-T1 (COMS small) 9.1×9.5×2 mm choroidal melanoma (arrow at tumour location). No FDG uptake was detected on PET and CT could not visualise the small tumour in the right eye.

Patient 6. An AJCC–T2 (COMS medium) 13.8×14×7.3 mm choroidal melanoma was detected on PET/CT imaging in the right eye (arrow). There was increased FDG uptake and CT localised the uveal tumour.

Patient 9. PET/CT imaging detected an AJCC–T3 (COMS large) 14×16×11.5 mm choroidal melanoma (COMS/AJCC) in the left eye (arrow).
PET/CT detection of ocular melanoma.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PET/CT detection of ocular melanoma.
DISCUSSION
With the introduction of positron emission tomography in the 1960s, and its growing importance in clinical practice within the past decade, various studies addressed the question whether PET imaging can be used to diagnose and stage malignant choroidal melanomas. A prospective study by Spraul et al concluded that FDG-PET alone was not a sensitive procedure for the diagnosis of choroidal melanomas since only two out of their four cases were visualised.9 Similarly, PET alone detected three of 12 uveal melanomas in one study and another reported only seven of 20.10,11 However, in the past few years, the PET/CT fusion scanners are helping bring molecular imaging to the forefront of cancer diagnosis.12 A modern PET/CT scanner combines the metabolic/physiological findings of PET with the anatomic localisation/characterisation of CT.
PET/CT increases the accuracy and confidence in judging whether a tumour is malignant.13 This has been shown for colorectal cancer as well as primary head and neck malignancies.14,15 In addition, PET/CT has eliminated the need for a full dose diagnostic CT to correlate inconclusive findings demonstrated by PET alone.15 In addition, examination times have been reduced by 30% (compared to conventional PET imaging) because PET attenuation correction can now be based on the CT data. This eliminates the need for separate transmission scanning.15 Compared with PET alone, PET/CT is also superior because it anatomically locates the melanoma and thereby increases the confidence that it is the tumour that is being characterised by FDG uptake.
In our study, neither AJCC-T1 uveal tumours nor small COMS choroidal melanomas were identified by PET/CT. Therefore, it is unlikely that PET/CT can be used to differentiate between small choroidal melanomas and suspicious choroidal naevi (at this time). Furthermore, 63% of T2 tumours and 69% of small choroidal tumours (that went undetected) were larger than the 4 mm resolution of our scanner. This suggests that high metabolic activity was integral to making a tumour identifiable. PET/CT was most effective in detecting the physiological activity of AJCC-T3 and large choroidal melanomas. Age, sex, or tumour location did not appear to affect SUV value.
This study did not examine if the metabolic activity revealed by PET/CT correlated with tumour metastasis. This study did not find PET/CT to be a more accurate method to diagnose intraocular choroidal melanoma (compared to standard clinical evaluations). This study clearly demonstrated that current FDG-PET/CT technology can reveal metabolic activity of choroidal melanomas, that there appears to be significant variability among melanomas of different sizes, and that further research will define the role of PET/CT in ophthalmic oncology.
REFERENCES
Footnotes
-
This research was supported by The EyeCare Foundation, Inc, and Research to Prevent Blindness, New York, NY, USA
-
Competing interests: none declared