
Abstract
Purpose
The aim of this study was to evaluate whether the acquisition of delayed images could improve the detectability of liver pathological uptakes.
Materials and methods
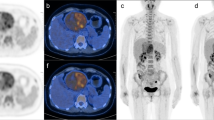
Ninety-five consecutive patients with suspected liver metastases underwent a dual-phase positron emission tomography (PET) scan. All patients underwent a whole-body PET/computed tomography (CT) scan (PET-1) acquired 1 h post [18F]fluorodeoxyglucose (FDG) injection, and a liver PET/CT scan [that is, one or two fields of view (FOV) of the upper abdomen; PET-2] acquired 2 h postinjection. In all cases, image reconstruction was performed as 3D reconstruction algorithm Fourier rebinning (FORE) iterative, FOV 50 cm, image matrix size 128×128. Both studies were evaluated qualitatively and semiquantitatively [background standard uptake values (SUV)mean of the liver, lesion SUVmax and SUVmean and ratio SUVmean lesion/background).
Results
Thirty-seven of 95 patients (38.9%) presented liver lesions at both PET-1 and PET-2 exams, whereas there were two (2.2%) only at PET-2. Eighty-one liver lesions were identified at both PET studies, whereas there were nine (11.1%) only at PET-2. Furthermore, at PET-2, we had a statistically significant reduction of SUVmean background values (p<0.001, Wilcoxon test) and a concomitant increase of SUVmean lesion values (p<0.001, Wilcoxon test), ratio lesion to background (p<0.001, Wilcoxon test).
Conclusions
Acquisition of delayed images improved the hepatic detection of pathological FDG uptake.
Riassunto
Obiettivo
Scopo di questo studio è stato quello di valutare se in pazienti con sospette secondarietà epatiche, la riacquisizione di immagini, 2 ore dopo la somministrazione del radiofarmaco (tardiva), comporta un miglioramento della sensibilità dell’esame PET.
Materiali e metodi
Sono stati inclusi 95 pazienti consecutivi con sospette metastasi epatiche. Tutti hanno eseguito esame PET/TC total body 1 ora dopo la somministrazione di FDG (PET-1). In tutti i casi, 2 ore dopo l’iniezione, è stata eseguita una seconda acquisizione mirata sull’addome superiore (PET-2). La ricostruzione delle immagini è stata eseguita con algoritmo 3D FORE iterativo (FOV 50 cm, dimensione della matrice 128×128). Entrambi gli esami sono stati valutati qualitativamente e semi-quantitativamente (SUVmedio fondo del fegato, SUVmax e SUVmedio della lesione e rapporto SUVmedio lesione/fondo).
Risultati
Trentasette dei 95 pazienti (38,9%) hanno presentato anomale iperfissazioni di radiofarmaco a livello epatico in entrambi gli esami PET; 2 pazienti (2,2%) sono risultati positivi solo in PET-2. Entrambi gli esami hanno messo in evidenza 81 lesioni epatiche, mentre altre 9 (11,1%) sono state evidenziate solo con l’esame PET-2. Inoltre in PET-2 si notava una riduzione significativa del SUVmedio del fondo (p<0,001, Wilcoxon test) ed un contemporaneo aumento del SUVmedio della lesione (p<0,001, Wilcoxon test) e del rapporto lesione/fondo (p<0,001, Wilcoxon test).
Conclusioni
La riacquisizione tardiva di immagini PET aumenta la capacità dell’esame PET di identificare fissazioni patologiche di FDG a livello epatico.
Similar content being viewed by others
References/Bibliografia
Pelosi E, Messa C, Sironi S et al (2004) Value of integrated PET/CT for lesion localisation in cancer patients: a comparative study. Eur J Nucl Med Mol Imaging 31: 932–939
Erasmus JJ, McAdams HP, Patz EFJr et al (1998) Evaluation of primary pulmonary carcinoid tumors using FDG PET. AJR Am J Roentgenol 170:1369–1373
Higashi K, Ueda Y, Seki H et al (1998) Fluorine-18-FDG PET imaging is negative in bronchioloalveolar lung carcinoma. J Nucl Med 39:1016–1020
Jana S, Blaufox MD (2006) Nuclear medicine studies of the prostate, testes, and bladder. Semin Nucl Med 36:51–72
Talbot JN, Gutman F, Fartoux L et al (2006) PET/CT in patients with hepatocellular carcinoma using [(18)F]fluorocholine: preliminary comparison with [(18)F]FDG PET/CT. Eur J Nucl Med Mol Imaging 33:1285–1289
Lindholm P, Minn H, Leskinen-Kallio S et al (1993) Influence of the blood glucose concentration on FDG uptake in cancer-a PET study. J Nucl Med 34:1–6
Bettinardi V, Danna M, Savi A et al (2004) Performance evaluation of the new whole-body PET/CT scanner: Discovery ST. Eur J Nucl Med Mol Imaging 31:867–881
Surti S, Karp JS (2004) Imaging characteristics of a 3-dimensional GSO whole-body PET camera. J Nucl Med 45:1040–1049
Brambilla M, Secco C, Dominietto M et al (2005) Performance characteristics obtained for a new 3-dimensional lutetium oxyorthosilicate-based wholebody PET/CT scanner with the National Electrical Manufacturers Association NU 2-2001 standard. J Nucl Med 46:2083–2091
Cook GJ, Fogelman I, Maisey MN (1996) Normal physiological and benign pathological variants of 18-fluoro-2-deoxyglucose positron-emission tomography scanning: potential for error in interpretation. Semin Nucl Med 26:308–314
Boucher L, Rodrigue S, Lecomte R, Benard F (2004) Respiratory gating for 3-dimensional PET of the thorax: feasibility and initial results. J Nucl Med 45:214–219
Ruers TJ, Langenhoff BS, Neeleman N et al (2002) Value of positron emission tomography with [18F] fluorodeoxyglucose in patients with colorectal liver metastases: a prospective study. J Clin Oncol 20:388–395
Nehmeh SA, Erdi YE, Pan T et al (2004) Four-dimensional (4D) PET/CT imaging of the thorax. Med Phys 31:3179–3186
Slosman DO, Quinodoz M, Willi JP (2005) Breath-hold PET/CT imaging: clinical value in thoracic and upper abdominal investigations. Eur J Nucl Med Mol Imaging 32(Suppl 1):S80
Kubota K, Itoh M, Ozaki K et al (2001) Advantage of delayed whole-body FDG-PET imaging for tumor detection. Eur J Nucl Med 28:696–703
Lowe VJ, DeLong DM, Hoffman JM, Coleman RE (1995) Optimum scanning protocol for FDG-PET evaluation of pulmonary malignancy. J Nucl Med 36:883–887
Fischman AJ, Alpert NM (1993) FDGPET in oncology: there’s more to it than looking at pictures. J Nucl Med 34:6–11
Hustinx R, Smith RJ, Benard F et al (1999) Dual time point fluorine-18 fluorodeoxyglucose positron emission tomography: a potential method to differentiate malignancy from inflammation and normal tissue in the head and neck. Eur J Nucl Med 26:1345–1348
Matthies A, Hickeson M, Cuchiara A, Alavi A (2002) Dual time point 18F-FDG PET for the evaluation of pulmonary nodules. J Nucl Med 43:871–875
Koyama K, Okamura T, Kawabe J et al (2002) The usefulness of 18F-FDG PET images obtained 2 hours after intravenous injection in liver tumor. Ann Nucl Med 16:169–176
Higashi T, Saga T, Nakamoto Y et al (2003) Diagnosis of pancreatic cancer using fluorine-18 fluorodeoxyglucose positron emission tomography (FDG PET): usefulness and limitations in “clinical reality”. Ann Nucl Med 17:261–279
Torizuka T, Tamaki N, Inokuma T et al (1995) In vivo assessment of glucose metabolism in hepatocellular carcinoma with FDG-PET. J Nucl Med 36:1811–1817
Nishiyama Y, Yamamoto Y, Monden T et al (2005) Evaluation of delayed additional FDG PET imaging in patients with pancreatic tumour. Nucl Med Comm 26:895–901
Gallagher BM, Fowler JS, Gutterson NI et al (1978) Metabolic trapping as a principle of radiopharmaceutical design: some factors resposible for the biodistribution of [18F] 2-deoxy-2-fluoro-D-glucose. J Nucl Med 19:1154–1161
Okazumi S, Isono K, Enomoto K et al (1992) Evaluation of liver tumors using fluorine-18-fluorodeoxyglucose PET: characterization of tumor and assessment of effect of treatment. J Nucl Med 33:333–339
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Arena, V., Skanjeti, A., Casoni, R. et al. Dual-phase FDG-PET: delayed acquisition improves hepatic detectability of pathological uptake. Radiol med 113, 875–886 (2008). https://doi.org/10.1007/s11547-008-0287-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-008-0287-0