
Abstract
Purpose
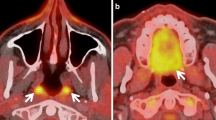
To retrospectively determine whether increased/asymmetric FDG uptake on PET without a correlating morphological lesion on fully diagnostic CT indicates the development of a head and neck malignancy.
Methods
In 590 patients (mean age 55.4 ± 13.3 years) without a head and neck malignancy/inflammation FDG uptake was measured at (a) Waldeyer’s ring, (b) the oral floor, (c) the larynx, and (d) the thyroid gland, and rated as absent (group A), present (group B), symmetric (group B1) or asymmetric (group B2). Differences between groups A and B and between B1 and B2 were tested for significance with the U-test (p < 0.05). An average follow-up of about 2.5 years (mean 29.5 ± 13.9 months) served as the reference period to determine whether patients developed a head and neck malignancy.
Results
Of the 590 patients, 235 (40%) showed no evidence of enhanced FDG uptake in any investigated site, and 355 (60%) showed qualitatively elevated FDG uptake in at least one site. FDG uptake values (SUVmax, mean±SD) for Waldeyer’s ring were 3.0 ± 0.89 in group A (n = 326), 4.5 ± 2.18 in group B (n = 264; p < 0.01), 5.4 ± 3.35 in group B1 (n = 177), and 4.1 ± 1.7 in group B2 (n = 87; p < 0.01). Values for the oral floor were 2.8 ± 0.74 in group A (n = 362), 4.7 ± 2.55 in group B (n = 228; p < 0.01), 4.4 ± 3.39 in group B1 (n = 130), and 5.1 ± 2.69 in group B2 (n = 98, p = 0.01). Values for the larynx were 2.8 ± 0.76 in group A (n = 353), 4.2 ± 2.05 in group B (n = 237; p < 0.01), 4.0 ± 2.02 in group B1 (n = 165), and 4.6 ± 2.8 in group B2 (n = 72; p = 0.027). Values for the thyroid were 2.4 ± 0.63 in group A (n = 404), 3.0 ± 1.01 in group B (n = 186; p < 0.01), 2.6 ± 0.39 in group B1 (n = 130), and 4.0 ± 1.24 in group B2 (n = 56; p < 0.01). One patient developed a palatine tonsil carcinoma (group B1, SUVmax 3.2), and one patient developed an oral floor carcinoma (group B1, SUVmax 3.7).
Conclusion
Elevated/asymmetric head and neck FDG accumulation without a correlating morphological lesion can frequently be found and does not predict cancer development. In populations in which goitre is endemic, FDG uptake by the thyroid is common and not associated with thyroid cancer.





Similar content being viewed by others


References
Pentenero M, Cistaro A, Brusa M, Ferraris MM, Pezzuto C, Carnino R, et al. Accuracy of 18F-FDG-PET/CT for staging of oral squamous cell carcinoma. Head Neck. 2008;30:1488–96.
Chen YK, Su CT, Chi KH, Cheng RH, Wang SC, Hsu CH. Utility of 18F-FDG PET/CT uptake patterns in Waldeyer’s ring for differentiating benign from malignant lesions in lateral pharyngeal recess of nasopharynx. J Nucl Med. 2007;48:8–14.
Cook GJ, Maisey MN, Fogelman I. Normal variants, artefacts and interpretative pitfalls in PET imaging with 18-fluoro-2-deoxyglucose and carbon-11 methionine. Eur J Nucl Med. 1999;26:1363–78. doi: 10.1007/s002590050597.
Nakamoto Y, Tatsumi M, Hammoud D, Cohade C, Osman MM, Wahl RL. Normal FDG distribution patterns in the head and neck: PET/CT evaluation. Radiology 2005;234:879–85. doi: 10.1148/radiol.2343030301.
Kostakoglu L, Hardoff R, Mirtcheva R, Goldsmith SJ. PET-CT fusion imaging in differentiating physiologic from pathologic FDG uptake. Radiographics 2004;24:1411–31. doi: 10.1148/rg.245035725.
Rosenbaum SJ, Lind T, Antoch G, Bockisch A. False-positive FDG PET uptake – the role of PET/CT. Eur Radiol 2006;16:1054–65. doi: 10.1007/s00330-005-0088-y.
Strauss LG. Fluorine-18 deoxyglucose and false-positive results: a major problem in the diagnostics of oncological patients. Eur J Nucl Med 1996;23:1409–15. doi: 10.1007/BF01367602.
Stahl A, Dzewas B, Schwaiger M, Weber WA. Excretion of FDG into saliva and its significance for PET imaging. Nuklearmedizin 2002;41:214–6.
Wong RJ. Current status of FDG-PET for head and neck cancer. J Surg Oncol 2008;97:649–52. doi: 10.1002/jso.21018.
Del Rocio Estrada-Sanchez G, Altamirano-Ley J, Ochoa-Carrillo FJ. Normal variants and frequent pitfalls with (18)FDG PET/CT study. Cir Cir. 2007;75:491–7.
Blodgett TM, Fukui MB, Snyderman CH, Branstetter BF 4th, McCook BM, Townsend DW, et al. Combined PET-CT in the head and neck: part 1. Physiologic, altered physiologic, and artifactual FDG uptake. Radiographics 2005;25:897–912. doi: 10.1148/rg.254035156.
Blodgett TM, Meltzer CC, Townsend DW. PET/CT: form and function. Radiology 2007;242:360–85. doi: 10.1148/radiol.2422051113.
Antoch G, Saoudi N, Kuehl H, Dahmen G, Mueller SP, Beyer T, et al. Accuracy of whole-body dual-modality fluorine-18-2-fluoro-2-deoxy-D-glucose positron emission tomography and computed tomography (FDG-PET/CT) for tumor staging in solid tumors: comparison with CT and PET. J Clin Oncol 2004;22:4357–68. doi: 10.1200/JCO.2004.08.120.
Antoch G, Vogt FM, Bockisch A, Ruehm SG. Whole-body tumor staging: MRI or FDG-PET/CT? Radiologe 2004;44:882–8. doi: 10.1007/s00117-004-1093-x.
Antoch G, Vogt FM, Freudenberg LS, Nazaradeh F, Goehde SC, Barkhausen J, et al. Whole-body dual-modality PET/CT and whole-body MRI for tumor staging in oncology. JAMA 2003;290:3199–206. doi: 10.1001/jama.290.24.3199.
Stahl A, Stollfuss J, Ott K, Wieder H, Fink U, Schwaiger M, et al. FDG PET and CT in locally advanced adenocarcinomas of the distal oesophagus. Clinical relevance of a discordant PET finding. Nuklearmedizin 2005;44:249–55.
Kapoor V, Fukui MB, McCook BM. Role of 18FFDG PET/CT in the treatment of head and neck cancers: principles, technique, normal distribution, and initial staging. AJR Am J Roentgenol 2005;184:579–87.
Kapoor V, Fukui MB, McCook BM. Role of 18FFDG PET/CT in the treatment of head and neck cancers: posttherapy evaluation and pitfalls. AJR Am J Roentgenol 2005;184:589–97.
Ng SH, Chan SC, Yen TC, Chang JT, Liao CT, Ko SF, et al. Staging of untreated nasopharyngeal carcinoma with PET/CT: comparison with conventional imaging work-up. Eur J Nucl Med Mol Imaging 2008;36:12–22.
Ha PK, Hdeib A, Goldenberg D, Jacene H, Patel P, Koch W, et al. The role of positron emission tomography and computed tomography fusion in the management of early-stage and advanced-stage primary head and neck squamous cell carcinoma. Arch Otolaryngol Head Neck Surg 2006;132:12–6. doi: 10.1001/archotol.132.1.12.
Schoder H, Yeung HW, Gonen M, Kraus D, Larson SM. Head and neck cancer: clinical usefulness and accuracy of PET/CT image fusion. Radiology 2004;231:65–72. doi: 10.1148/radiol.2311030271.
Abouzied MM, Crawford ES, Nabi HA. 18F-FDG imaging: pitfalls and artifacts. J Nucl Med Technol 2005;33:145–55.
Cook GJ, Fogelman I, Maisey MN. Normal physiological and benign pathological variants of 18-fluoro-2-deoxyglucose positron-emission tomography scanning: potential for error in interpretation. Semin Nucl Med 1996;26:308–14. doi: 10.1016/S0001-2998(96)80006-7.
Basu S, Houseni M, Alavi A. Significance of incidental fluorodeoxyglucose uptake in the parotid glands and its impact on patient management. Nucl Med Commun 2008;29:367–73.
Antoch G, Kuehl H, Kanja J, Lauenstein TC, Schneemann H, Hauth E, et al. Dual-modality PET/CT scanning with negative oral contrast agent to avoid artifacts: introduction and evaluation. Radiology 2004;230:879–85. doi: 10.1148/radiol.2303021287.
Beyer T, Antoch G, Blodgett T, Freudenberg LF, Akhurst T, Mueller S. Dual-modality PET/CT imaging: the effect of respiratory motion on combined image quality in clinical oncology. Eur J Nucl Med Mol Imaging 2003;30:588–96.
Wong WL, Gibson D, Sanghera B, Goodchild K, Saunders M. Evaluation of normal FDG uptake in palatine tonsil and its potential value for detecting occult head and neck cancers: a PET CT study. Nucl Med Commun 2007;28:675–80. doi: 10.1097/MNM.0b013e32829152b1.
Goerres GW, Hany TF, Kamel E, von Schulthess GK, Buck A. Head and neck imaging with PET and PET/CT: artefacts from dental metallic implants. Eur J Nucl Med Mol Imaging 2002;29:367–70. doi: 10.1007/s00259-001-0721-1.
Kamel EM, Burger C, Buck A, von Schulthess GK, Goerres GW. Impact of metallic dental implants on CT-based attenuation correction in a combined PET/CT scanner. Eur Radiol 2003;13:724–8.
Schoder H, Yeung HW. Positron emission imaging of head and neck cancer, including thyroid carcinoma. Semin Nucl Med 2004;34:180–97. doi: 10.1053/j.semnuclmed.2004.03.004.
Macapinlac HA. FDG-PET in head and neck, and thyroid cancer. Chang Gung Med J 2005;28:284–95.
Pfannenberg AC, Aschoff P, Brechtel K, Muller M, Bares R, Paulsen F, et al. Low dose non-enhanced CT versus standard dose contrast-enhanced CT in combined PET/CT protocols for staging and therapy planning in non-small cell lung cancer. Eur J Nucl Med Mol Imaging 2007;34:36–44. doi: 10.1007/s00259-006-0186-3.
Syed R, Bomanji JB, Nagabhushan N, Hughes S, Kayani I, Groves A, et al. Impact of combined (18)F-FDG PET/CT in head and neck tumours. Br J Cancer 2005;92:1046–50. doi: 10.1038/sj.bjc.6602464.
Pfannenberg AC, Aschoff P, Brechtel K, Muller M, Klein M, Bares R, et al. Value of contrast-enhanced multiphase CT in combined PET/CT protocols for oncological imaging. Br J Radiol 2007;80:437–45. doi: 10.1259/bjr/34082277.
Antoch G, Forsting M. How much CT does PET/CT need? Nuklearmedizin 2004;43:141–2.
Antoch G, Freudenberg LS, Beyer T, Bockisch A, Debatin JF. To enhance or not to enhance? 18F-FDG and CT contrast agents in dual-modality 18F-FDG PET/CT. J Nucl Med 2004;45(Suppl 1):56S–65S.
Jackson RS, Schlarman TC, Hubble WL, Osman MM. Prevalence and patterns of physiologic muscle uptake detected with whole-body 18F-FDG PET. J Nucl Med Technol 2006;34:29–33.
Kawabe J, Okamura T, Shakudo M, Koyama K, Sakamoto H, Ohachi Y, et al. Physiological FDG uptake in the palatine tonsils. Ann Nucl Med 2001;15:297–300. doi: 10.1007/BF02987850.
Barrington SF, Maisey MN. Skeletal muscle uptake of fluorine-18-FDG: effect of oral diazepam. J Nucl Med 1996;37:1127–9.
Kubota R, Yamada S, Kubota K, Ishiwata K, Tamahashi N, Ido T. Intratumoral distribution of fluorine-18-fluorodeoxyglucose in vivo: high accumulation in macrophages and granulation tissues studied by microautoradiography. J Nucl Med 1992;33:1972–80.
Scadding GK. Immunology of the tonsil: a review. J R Soc Med 1990;83:104–7.
Paik JY, Lee KH, Choe YS, Choi Y, Kim BT. Augmented 18F-FDG uptake in activated monocytes occurs during the priming process and involves tyrosine kinases and protein kinase C. J Nucl Med 2004;45:124–8.
Babior BM. The respiratory burst of phagocytes. J Clin Invest 1984;73:599–601. doi: 10.1172/JCI111249.
Wang Y, Chiu E, Rosenberg J, Gambhir SS. Standardized uptake value atlas: characterization of physiological 2-deoxy-2-[18F]fluoro-D-glucose uptake in normal tissues. Mol Imaging Biol 2007;9:83–90. doi:10.1007/s11307-006-0075-y.
Zincirkeser S, Sahin E, Halac M, Sager S. Standardized uptake values of normal organs on 18F-fluorodeoxyglucose positron emission tomography and computed tomography imaging. J Int Med Res 2007;35:231–6.
Lalla RV, Sonis ST, Peterson DE. Management of oral mucositis in patients who have cancer. Dent Clin North Am 2008;52:61–77. doi: 10.1016/j.cden.2007.10.002.
Kang KW, Kim SK, Kang HS, Lee ES, Sim JS, Lee IG, et al. Prevalence and risk of cancer of focal thyroid incidentaloma identified by 18F-fluorodeoxyglucose positron emission tomography for metastasis evaluation and cancer screening in healthy subjects. J Clin Endocrinol Metab 2003;88:4100–4. doi: 10.1210/jc.2003-030465.
Mikosch P, Wurtz FG, Gallowitsch HJ, Kresnik E, Lind P. F-18-FDG-PET in a patient with Hashimoto’s thyroiditis and MALT lymphoma recurrence of the thyroid. Wien Med Wochenschr 2003;153:89–92. doi: 10.1046/j.1563-258X.2003.02007.x.
Rohren EM. Intense FDG uptake in a benign Hurthle cell adenoma. Clin Nucl Med 2004;29:664–6. doi: 10.1097/00003072-200410000-00021.
King DL, Stack BC Jr, Spring PM, Walker R, Bodenner DL. Incidence of thyroid carcinoma in fluorodeoxyglucose positron emission tomography-positive thyroid incidentalomas. Otolaryngol Head Neck Surg 2007;137:400–4. doi: 10.1016/j.otohns.2007.02.037.
Kurata S, Ishibashi M, Hiromatsu Y, Kaida H, Miyake I, Uchida M, et al. Diffuse and diffuse-plus-focal uptake in the thyroid gland identified by using FDG-PET: prevalence of thyroid cancer and Hashimoto’s thyroiditis. Ann Nucl Med 2007;21:325–30. doi: 10.1007/s12149-007-0030-2.
Kim TY, Kim WB, Ryu JS, Gong G, Hong SJ, Shong YK. 18F-fluorodeoxyglucose uptake in thyroid from positron emission tomogram (PET) for evaluation in cancer patients: high prevalence of malignancy in thyroid PET incidentaloma. Laryngoscope 2005;115:1074–8. doi: 10.1097/01.MLG.0000163098.01398.79.
Donta TS, Smoker WR. Head and neck cancer: carcinoma of unknown primary. Top Magn Reson Imaging 2007;18:281–92. doi:10.1097/RMR.0b0113e3181570c6c.
Revel MP, Merlin A, Peyrard S, Triki R, Couchon S, Chatellier G, et al. Software volumetric evaluation of doubling times for differentiating benign versus malignant pulmonary nodules. AJR Am J Roentgenol 2006;187:135–42. doi: 10.2214/AJR.05.1228.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Heusner, T.A., Hahn, S., Hamami, M.E. et al. Incidental head and neck 18F-FDG uptake on PET/CT without corresponding morphological lesion: early predictor of cancer development?. Eur J Nucl Med Mol Imaging 36, 1397–1406 (2009). https://doi.org/10.1007/s00259-009-1113-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-009-1113-1