
Abstract
Purpose
The purpose of the present study was to evaluate whether 2-fluoro[fluorine-18]-2-deoxy-d-glucose (F-18 FDG) positron emission tomography (PET) could differentiate malignant and benign bone lesions and whether obtaining delayed F-18 FDG PET images could improve the accuracy of the technique.
Methods
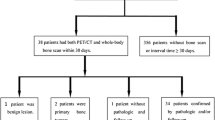
In a prospective study, 67 patients with bone lesions detected by computed tomography (CT) or magnetic resonance imaging were included. Whole body PET/CT imaging was performed at 1 h (early) after the F-18 FDG injection and delayed imaging at 2 h post injection was performed only in the abnormal region. Semiquantitative analysis was performed using maximum standardized uptake value (SUVmax), obtained from early and delayed images (SUVmaxE and SUVmaxD, respectively). The retention index (RI) was calculated according to the equation: RI = (SUVmaxD − SUVmaxE) × 100/SUVmaxE. Histopathology of surgical specimens and follow-up data were used as reference criteria. The SUVmaxE and RI were compared between benign and malignant lesions.
Results
The final diagnoses revealed 53 malignant bone lesions in 37 patients and 45 benign lesions in 30 patients. There were statistically significant differences in the SUVmaxE between the malignant and benign lesions (P = 0.03). The mean SUVmaxE was 6.8 ± 4.7 for malignant lesions and 4.5 ± 3.3 for benign lesions. However, a considerable overlap in the SUVmaxE was observed between some benign and malignant tumors. With a cutoff value of 2.5 for the SUVmaxE, the sensitivity, specificity, and accuracy were 96.0%, 44.0%, and 72.4%, respectively. The positive predictive value (PPV) and negative predictive value (NPV) were 67.1% and 90.9%, respectively. There were significant differences in the RI between the malignant and benign lesions (P = 0.004). But there was overlap between the two groups. The mean RI was 7 ± 11 for the benign lesions and 18 ± 11 for the malignant lesions. When an RI of 10 was used as the cutoff point, the sensitivity, specificity, and accuracy were 90.6%, 76.0%, and 83.7.0%, respectively. The PPV and NPV were 81.4% and 87.1%, respectively.
Conclusions
The results of this study indicate that dual-time point F-18 FDG PET may provide more help in the differentiation of malignant tumors from benign ones.





Similar content being viewed by others


References
Erlemann R. MRI is highly sensitive for the detection of bone marrow abnormalities, cortical destruction or soft tissue tumors adjacent or infiltrating neighboring bones. Eur J Radiol 2006; 58(1): 48–67.
Hillner BE, Siegel BA, Shields AF, et al. Relationship between cancer type and impact of PET and PET/CT on intended management: findings of the National Oncologic PET Registry. J Nucl Med 2008; 49(12): 1928–1935.
Kim SK, Allen-Auerbach M, Goldin J, et al. Accuracy of PET/CT in characterization of solitary pulmonary lesions. J Nucl Med 2007; 48(2): 214–220.
Dimitrakopoulou-Strauss ASL, Heichel T, Wu H, Burger C, Bernd L, Ewerbeck V. The role of quantitative 18F-FDG PET studies for the differentiation of malignant and benign bone lesions. J Nucl Med 2002; 43(4): 510–518.
Kern KA, Brunetti A, Norton JA, et al. Metabolic imaging of human extremity musculoskeletal tumors by PET. J Nucl Med 1988; 29(2): 181–186.
Adler LP, Blair HF, Makley JT, et al. Noninvasive grading of musculoskeletal tumors using PET. J Nucl Med 1991; 32(8): 1508–1512.
Griffeth LK, Dehdashti F, McGuire AH, et al. PET evaluation of soft-tissue masses with fluorine-18 fluoro-2-deoxy-d- glucose. Radiology 1992; 182(1): 185–194.
Dehdashti FSB, Griffeth LK, Fusselman MJ, Trask DD, McGuire AH. Benign versus malignant intraosseous lesions: discrimination by means of PET with 2-[F-18]fluoro-2-deoxy-d-glucose. Radiology 1996; 200(1): 243–247.
Aoki J, Watanabe H, Shinozaki T, et al. FDG PET of primary benign and malignant bone tumors: standardized uptake value in 52 lesions. Radiology 2001; 219(3): 774–777.
Kole AC, Nieweg OE, Hoekstra HJ, van Horn JR, Koops HS, Vaalburg W. Fluorine-18-fluorodeoxyglucose assessment of glucose metabolism in bone tumors. J Nucl Med 1998; 39(5): 810–815.
Schulte M, Brecht-Krauss D, Heymer B, et al. Grading of tumors and tumorlike lesions of bone: evaluation by FDG PET. J Nucl Med 2000; 41(10): 1695–1701.
Zhuang H, Pourdehnad M, Lambright ES, et al. Dual time point 18F-FDG PET imaging for differentiating malignant from inflammatory processes. J Nucl Med 2001; 42(9): 1412–1417.
Lan XL, Zhang YX, Wu ZJ, Jia Q, Wei H, Gao ZR. The value of dual time point 18F-FDG PET imaging for the differentiation between malignant and benign lesions. Clinical radiology 2008; 63(7): 756–764.
Matthies A, Hickeson M, Cuchiara A, Alavi A. Dual time point 18F-FDG PET for the evaluation of pulmonary nodules. J Nucl Med 2002; 43(7): 871–875.
Ma S-Y, See L-C, Lai C-H, et al. Delayed 18F-FDG PET for detection of paraaortic lymph node metastases in cervical cancer patients. J Nucl Med 2003; 44(11): 1775–1783.
Mavi A, Urhan M, Yu JQ, et al. Dual time point 18F-FDG PET imaging detects breast cancer with high sensitivity and correlates well with histologic subtypes. J Nucl Med 2006; 47(9): 1440–1446.
Xiu Y, Bhutani C, Dhurairaj T, et al. Dual-time point FDG PET imaging in the evaluation of pulmonary nodules with minimally increased metabolic activity. Clin Nucl Med 2007; 32(2): 101–105.
Sahlmann CO, Siefker U, Lehmann K, Meller J. Dual time point 2-[18F]fluoro-2′-deoxyglucose positron emission tomography in chronic bacterial osteomyelitis. Nucl Med Commun 2004; 25(8): 819–823.
Daisuke U, Shinya S, Masanori I, et al. Added value of SPECT/CT fusion in assessing suspected bone metastasis: comparison with scintigraphy alone and nonfused scintigraphy and CT. Radiology 2005; 238(11): 264–271.
Shin DS, Shon OJ, Han DS, Choi JH, Chun KA, Cho IH. The clinical efficacy of 18F-FDG-PET/CT in benign and malignant musculoskeletal tumors. Ann Nucl Med 2008; 22(7): 603–609.
Aoki J, Endo K, Watanabe H, Shinozaki T, Yanagawa T, Ahmed AR, et al. FDG-PET for evaluating musculoskeletal tumors. J Orthop Sci 2003; 8(3): 435–441.
Feldman F, Heertum RV, Manus C. 18FDG PET scanning of benign and malignant musculoskeletal lesions. Skeletal Radiol 2003; 32: 201–208.
Meszaros K, Lang CH, Bagby GJ, Spitzer JJ. Contribution of different organs to increased glucose consumption after endotoxin administration. J Biol Chem 1987; 262(23): 10965–10970.
Strobel K, Bode B, Lardinois D, Exner U. PET-positive fibrous dysplasia—a potentially misleading incidental finding in a patient with intimal sarcoma of the pulmonary artery. Skeletal Radiology 2007; 36: 24–28.
Conill C, Setoain X, Colomo L, et al. Diagnostic efficacy of bone scintigraphy, magnetic resonance imaging, and positron emission tomography in bone metastases of myxoid liposarcoma. J Magn Reson Imaging 2008; 27(3): 625–628.
Goo JM, Im J-G, Do K-H, et al. Pulmonary tuberculoma evaluated by means of FDG PET: findings in 10 cases. Radiology 2000; 216(1): 117–121.
Knight SB, Delbeke D, Stewart JR, Sandler MP. Evaluation of pulmonary lesions with FDG-PET: comparison of findings in patients with and without a history of prior malignancy. Chest 1996; 109(4): 982–988.
Bredella MA, Essary B, Torriani M, Ouellette HA, Palmer WE. Use of FDG-PET in differentiating benign from malignant compression fractures. Skeletal Radiol 2008; 37(5): 405–413.
Hustinx R, Smith RJ, Benard F, Rosenthal DI, Machtay M, Farber LA, et al. Dual time point fluorine-18 fluorodeoxyglucose positron emission tomography: a potential method to differentiate malignancy from inflammation and normal tissue in the head and neck. Eur J Nucl Med 1999; 26(10): 1345–1348.
Yoshihiro N, Yuka Y, Naruhide K, Shinya I, Yasuhiro S, Ohkawa M. Dual-time-point FDG-PET for evaluation of lymph node metastasis in patients with non-small-cell lung cancer. Ann Nucl Med 2008; 22: 245–250.
Hamada K, Tomita Y, Ueda T, et al. Evaluation of delayed 18F-FDG PET in differential diagnosis for malignant soft-tissue tumors. Ann Nucl Med 2006; 20(10): 671–675.
Strobel K, Exner UE, Stumpe KD, Hany TF, Bode B, Mende K, et al. The additional value of CT images interpretation in the differential diagnosis of benign vs. malignant primary bone lesions with 18F-FDG-PET/CT. Eur J Nucl Med Mol Imaging 2008; 35(11): 2000–2008.
Acknowledgments
We thank BioMed Proofreading for assistance in editing the manuscript. We also thank Luyi Zhou, Ph.D., for biostatistical assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tian, R., Su, M., Tian, Y. et al. Dual-time point PET/CT with F-18 FDG for the differentiation of malignant and benign bone lesions. Skeletal Radiol 38, 451–458 (2009). https://doi.org/10.1007/s00256-008-0643-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-008-0643-0