


Abstract
A congenital abnormal connection between an accessory spleen and a gonad is called splenogonadal fusion. The parent of a 3-y-old boy brought him to King Saud Medical City because he had left scrotal swelling that had begun 1 y previously. 99mTc-sulfur colloid (SC) imaging has superior sensitivity and specificity in targeting the liver, spleen, and bone marrow, in that these are the only organs that 99mTc-SC can visualize. Furthermore, if these tissues appear anywhere other than their usual locations, such as in the case of an accessory spleen, 99mTc-SC imaging can identify them even without biopsy or—in the case of splenogonadal fusion—orchiectomy. In the current case, the patient underwent laparoscopy, the masses were removed, and orchiectomy was avoided. Histopathologic examination confirmed normal splenic tissue, matching the imaging results.
Accessory spleens, which appear when there are deficient mesenchymal buds during development, can arise from the spleen when the gonads descend. The type of accessory spleen that is associated with the gonad is called splenogonadal fusion (SGF) (1).
SGF is also called ectopic scrotal spleen and usually presents before the age of 20 y; appearance in the left testis only is possible in boys younger than 10 y. The male-to-female ratio of SGF is 16:1 (2). Another published case (3) used nuclear medicine to rule out SGF. In the current case, SGF was diagnosed successfully using 99mTc-sulfur colloid (SC) imaging.
CASE REPORT
A 3-y-old boy was brought to King Saud Medical City by his parent because of left scrotal swelling that had first been noticed 1 y previously. Physical examination revealed unusual scrotal swelling that was painless and did not change in size on palpation. There was no history of trauma.
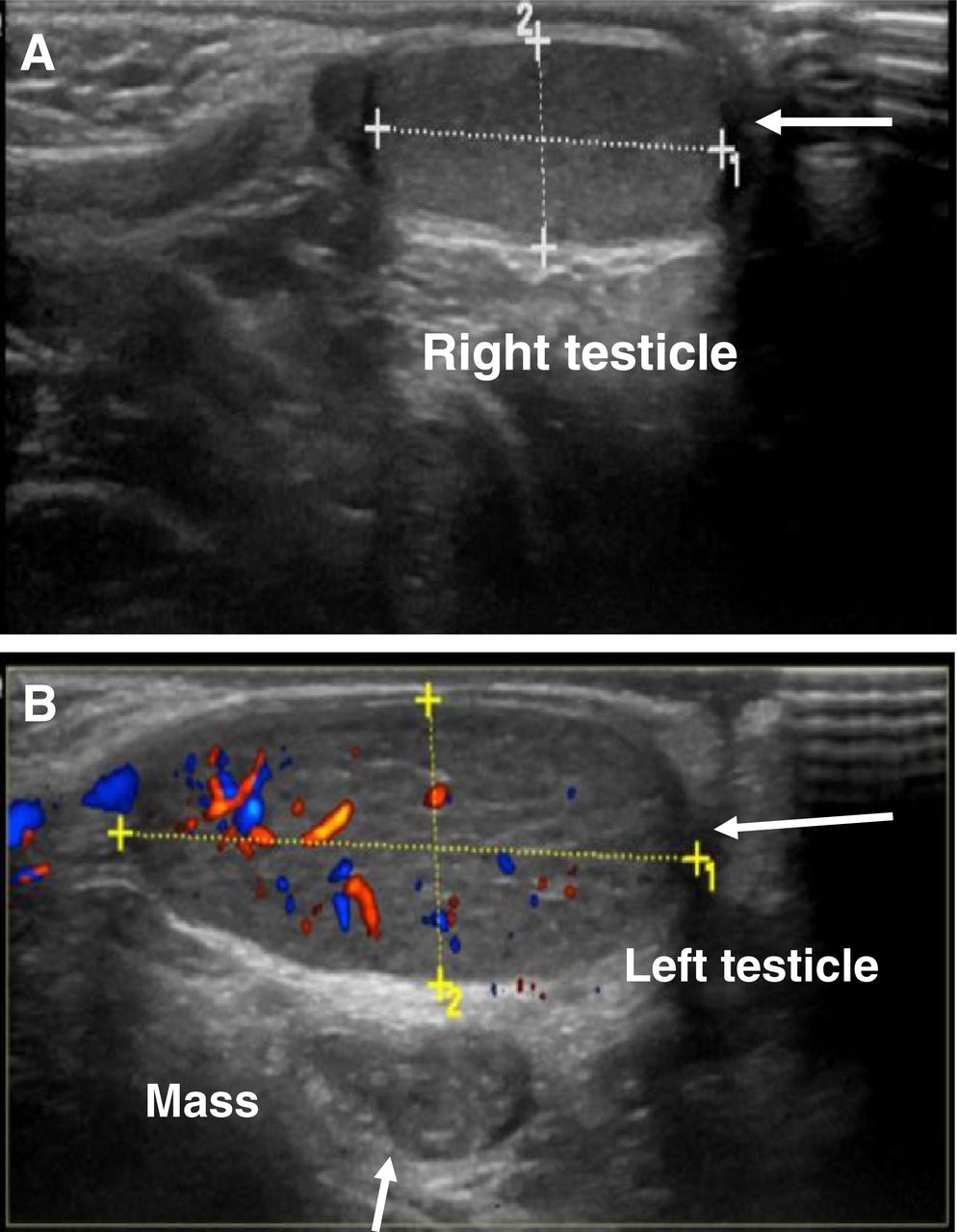
Ultrasound showed both testicles in the scrotum. The right measured 1.8 × 0.7 cm and had normal echogenicity and vascularity (Fig. 1A). The left measured 1.2 × 0.8 cm and also had normal echogenicity and vascularity. However, inseparable from the left testis was a well-defined, oval abnormal area of soft tissue that was of homogeneous echogenicity, measured 3 cm in length by 1.2 cm in diameter, and was adjacent to a feeding vessel (Fig. 1B). No obvious calcification was seen, and there was no evidence of a hydrocele or enlarged lymph nodes. The imaging differential diagnosis included an underlying testicular neoplasm, and 99mTc-SC imaging was performed to diagnose SGF.
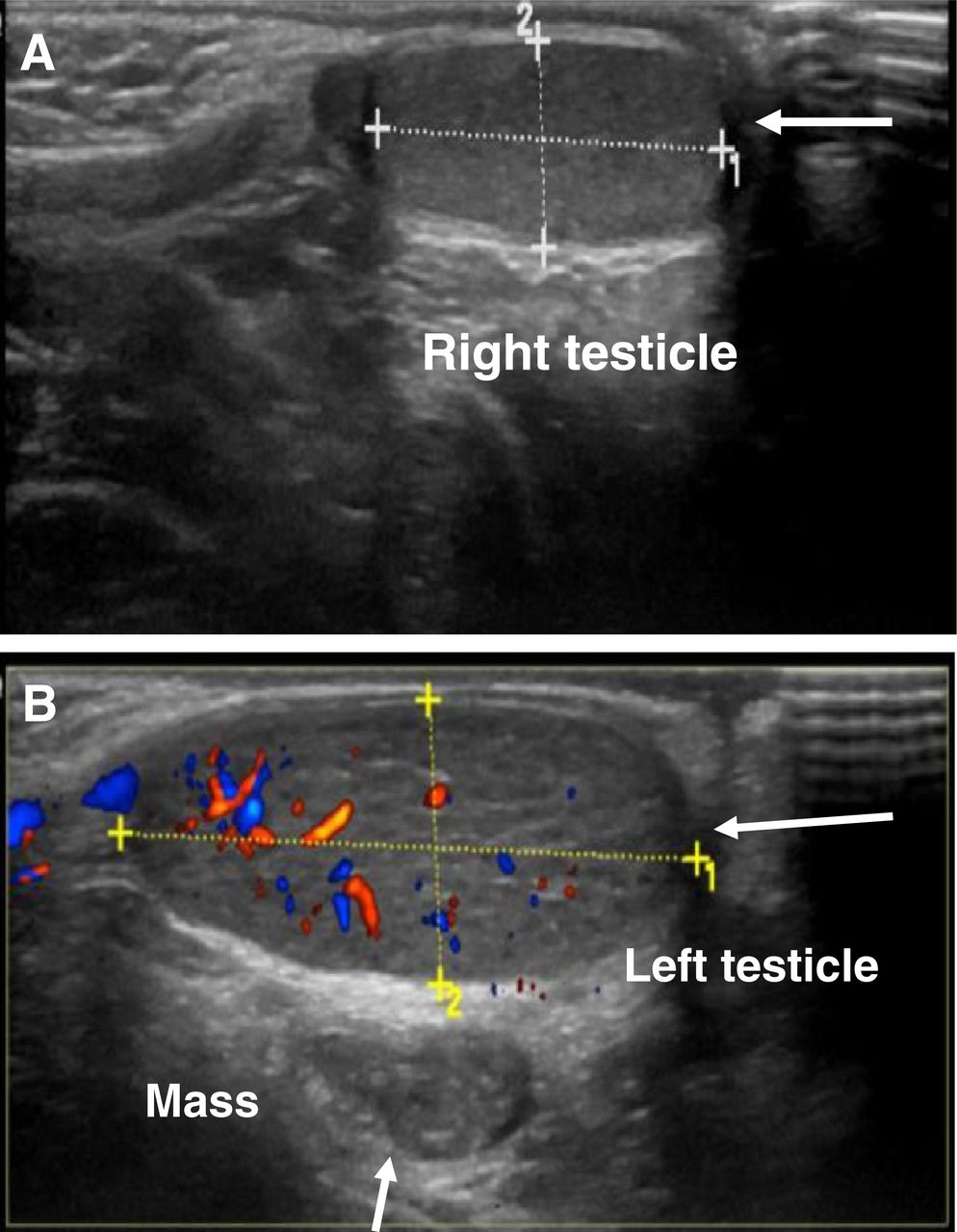
Ultrasound of scrotum. (A) Right testicle (arrow) measures 1.8 × 0.7 cm and shows normal echogenicity and vascularity. (B) Left testicle (horizontal arrow) measures 1.2 × 0.8 cm and shows normal echogenicity and vascularity. Well-defined, oval abnormal soft-tissue mass (vertical arrow) inseparable from left testis shows homogeneous echogenicity, measures 3 × 1.2 cm, and is adjacent to feeding vessel.

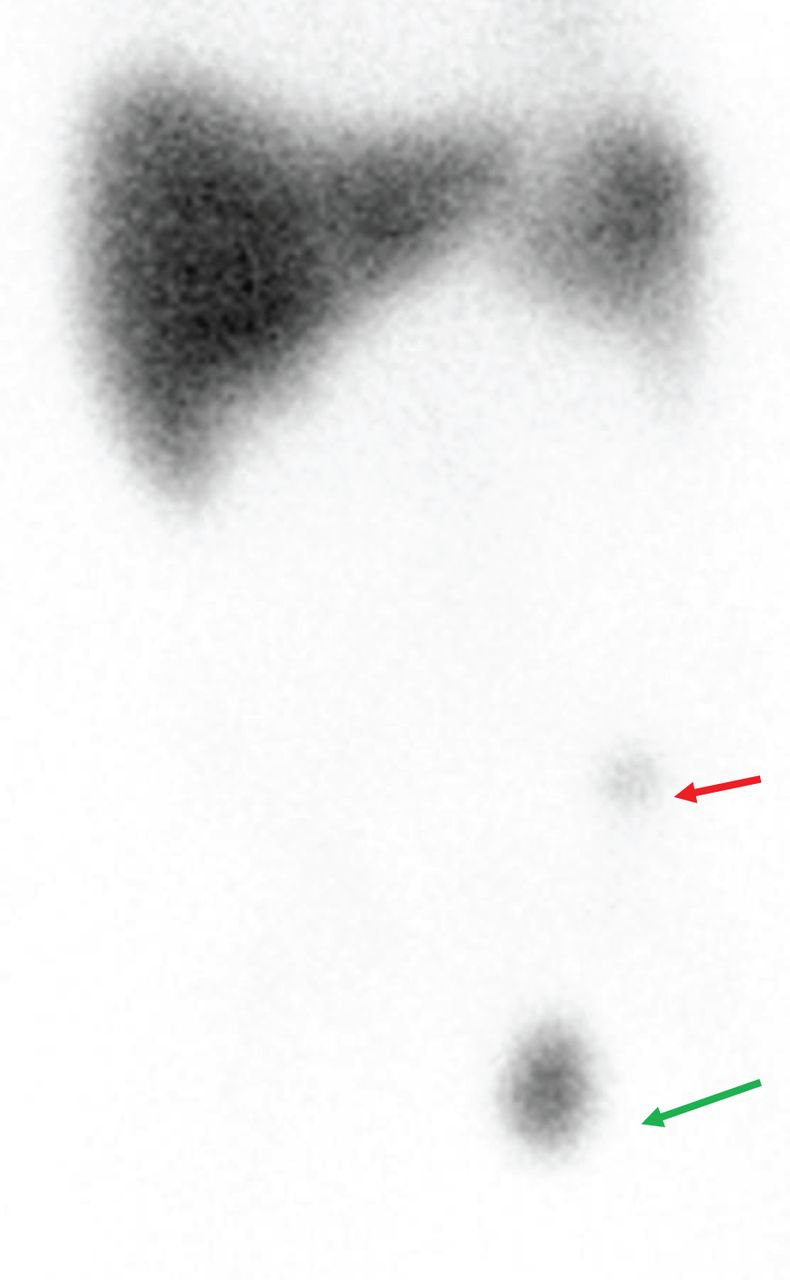
99mTc-SC image. Anterior planar view of abdomen and pelvis shows normal biodistribution of tracer, with 2 abnormal focal areas of uptake. One (green arrow) is more intense than the other, is in scrotum, measures about 2 × 2 cm, and matches mass noted on previous ultrasound. The other (red arrow) is in anterior part of left iliac fossa.
The patient was injected with 92.5 MBq (2.5 mCi) of 99mTc-SC. First, a static image over the anterior and posterior abdomen was obtained for 10 min. Afterward, SPECT/CT was performed over the same region, using a 360° rotation, a 128 × 128 matrix, and a rate of 30 s per frame.
The liver was found to be in its normal anatomic location and to measure 11 × 10.5 cm, with adequate, homogeneously distributed tracer uptake throughout. The spleen, in its normal anatomic location, was visualized as well. It measured about 7 × 5 cm. The images also showed 2 abnormal focal areas of uptake (Fig. 2). The more intense of these was in the scrotum (anterior to the left testicle), measured about 2 × 2 cm, and matched the mass noted on the previous ultrasound (Fig. 1). The mass was hyperdense, compared with the normal density of the testis. The second focus of abnormal uptake was smaller (∼1 cm of diameter) and less active, was in the anterior part of the left iliac fossa between the abdominal wall and the urinary bladder, and was highly suggestive of accessory spleen tissue. The imaging report concluded that the study gave a strong impression of SGF, with a small accessory spleen in the left iliac fossa and left testicle.
After these diagnostic tests, the patient underwent left laparoscopy with excision of the splenules in both the testis and the abdomen. The area was approached through an inguinal incision. Both specimens were sent for histopathologic examination, which found that they represented splenic tissue with no significant pathologic change.
DISCUSSION
SGF is an unusual medical disorder that presents from birth. This congenital malformation appears as splenic tissue in the gonad (4). Historically, SGF was first mentioned in 1913, by Sneath, a demonstrator of anatomy at the University of Manchester (5). There are 2 types of SGF, depending on whether the spleen and gonad are connected or unconnected (4). SGF is reported mostly in children and presents as an abnormal mass in the testicle. The first step to diagnosing SGF is the physical examination: the patient presents with pain in the left testis and swelling in the left scrotum. Ultrasound, CT, and MRI will show an abnormal mass in such cases.
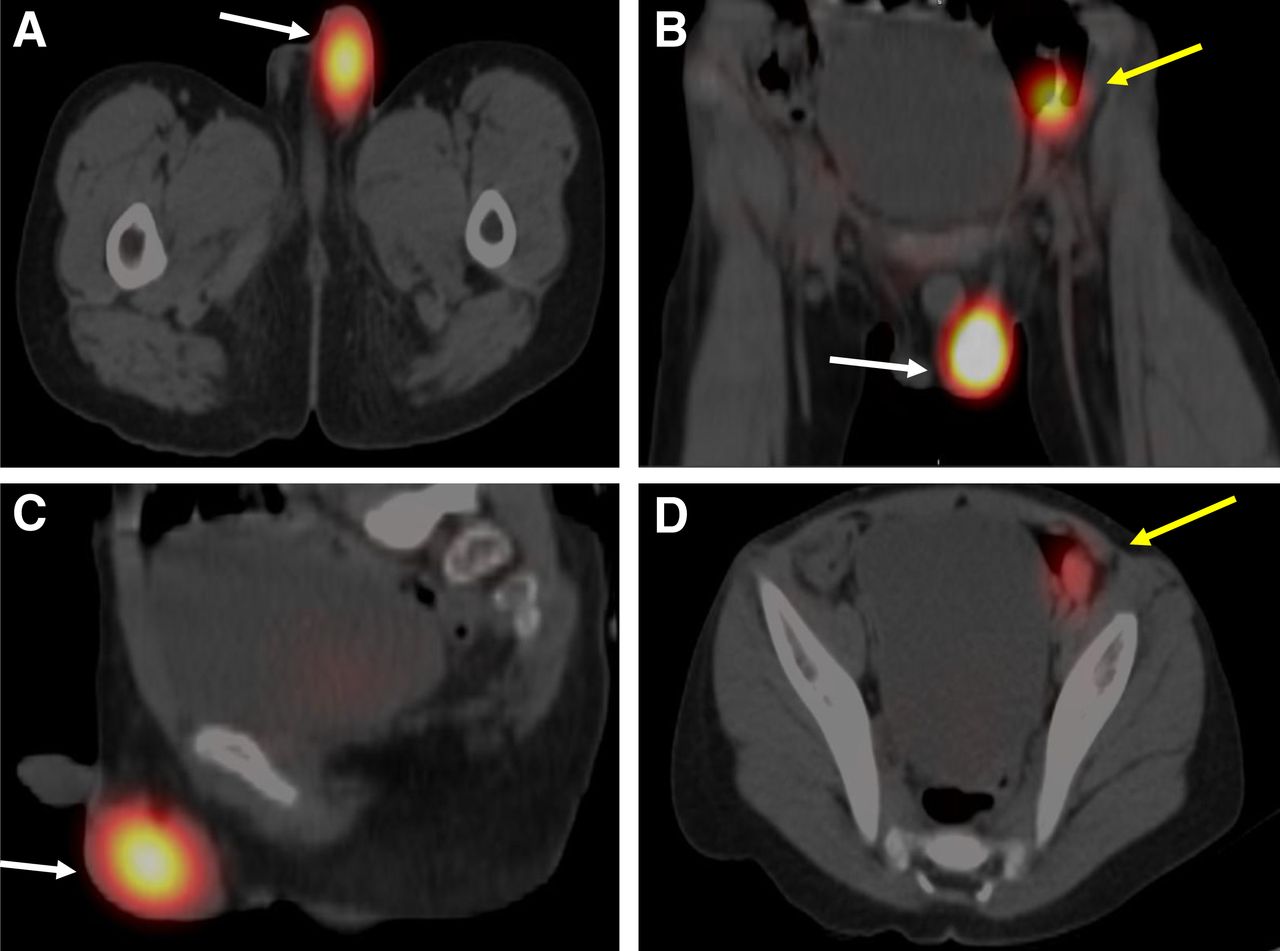
In the current case, ultrasound, MRI, and CT revealed a discrete hemiscrotal soft-tissue mass inseparable from the left testis but failed to characterize the mass. 99mTc-SC imaging is a noninvasive modality capable of detecting ectopic functioning splenic tissue and, in this case, helped to characterize the scrotal mass and diagnose SGF noninvasively (Fig. 3).

(A–C) 99mTc-SC SPECT/CT images showing 2 abnormal focal areas of uptake (white arrows) in axial (A), coronal (B), and sagittal (C) views and a second, less active focus (yellow arrow). (D) Axial SPECT/CT image showing that the less active focus (yellow arrow) is smaller (∼1 cm in diameter) than the other focus and is in anterior part of left iliac fossa between abdominal wall and urinary bladder; as such, it is highly suggestive of accessory spleen tissue.
Although our literature review indicated that few cases of SGF have been diagnosed with 99mTc-SC (3), we decided to send our patient to the nuclear medicine department for 99mTc-SC imaging to rule out SGF because this modality has a superior ability to differentiate between the distinctive tissues in such cases, on the basis of the percentage of the radiotracer distributed in the body. About 92% of 99mTc-SC bonds with the cells of the reticuloendothelial system. In other words, if the 99mTc-SC is prepared in the proper way in the hot lab and is imaged using the proper protocol, it will concentrate in only 3 organs: the liver, the spleen, and the bone marrow. In the current case, we saw high tracer uptake in the liver and spleen (Fig. 2), but the rest of the body had no tracer uptake except for the 2 foci of abnormally high uptake that turned out to be accessory spleens.
CONCLUSION
99mTc-SC imaging helps to diagnose SGF noninvasively and has a potential role in the evaluation of testicular masses.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online November 08, 2021.
- Received for publication March 6, 2021.
- Revision received July 20, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.