


Abstract
The emergence of PET and MRI as a hybrid modality has generated widespread interest in the technology and techniques. Although adoption and use are unlikely to be as expansive as for PET and CT hybrid systems, PET/MRI is an important modality that requires broad insight for nuclear medicine professions generally and deeper insight for those engaged in PET/MRI practice. This article provides insight into the considerations and challenges associated with establishing a PET/MRI facility. Each clinical site will present unique requisites for establishing a PET/MRI facility, and indeed, each PET/MRI vendor will have specific site requirements. Nonetheless, this article provides general insight into common considerations but should not be considered exhaustive. Here, development of the facility, staffing of the facility, and implications of both radiation and MRI safety are considered from the context of facility design. Given that the nature of PET is well established among the readership of this journal, the article provides an emphasis on MRI factors. This article is the first in a 4-part integrated series sponsored by the PET/MR and Publication Committees of the Society of Nuclear Medicine and Molecular Imaging–Technologist Section. In the subsequent 3 parts, PET/MRI will be explored on the basis of technology principles (part 2), protocols and procedures (part 3), and applications and clinical cases (part 4).
PET fused with simultaneously obtained MRI was established to fill the demand for high-contrast tissue information gained from the MRI with molecular imaging data provided by the PET. Conventionally, the exquisite molecular-level insights of PET have been combined in hybrid devices with the high resolution of CT. This approach provides both accurate anatomic localization and the opportunity for accurate attenuation correction of the PET data. Although dose reduction strategies have been implemented in both PET and CT, the combined PET/CT scanner remains hindered by high radiation doses to the patient. Furthermore, the nature of imaging is such that the imaging in PET/CT is sequential in nature rather than simultaneous. The value of PET/MRI is the substitution of the high-resolution CT data (excellent for hard structures and lung tissue) with the high-contrast detail, lack of ionizing radiation, and multiple sequences of the MRI data (excellent for soft structures) (1). Furthermore, PET/MRI allows for simultaneous imaging protocols that reduce motion artifacts and misregistration but confronts the challenges associated with attenuation correction (1,2). Although PET/CT remains the equipment of choice for many clinical scenarios, there are several clinical scenarios that are particularly suited to PET/MRI, such as pediatric patients and soft-tissue tumors. The technology will be detailed in part 2 of this series, and the protocols and clinical use will be covered in parts 3 and 4, respectively. There are 3 main aspects to establishing a PET/MRI facility: engineering, which is associated with facility design, siting, and both radiofrequency and radiation shielding; safety, which is associated with signage, facility access, and workflow; and staff, which is associated with qualifications, training, and capability.
ENGINEERING FACTORS
PET/MRI Facility
Unlike a PET/CT site, establishing a PET/MRI facility is not well documented in the literature (3,4). Building a PET/CT program within an existing nuclear medicine practice is relatively seamless if the space requirements exist and the fundamental planning considerations are uniform (albeit thicker shielding and dedicated uptake rooms). Regardless of the presence of an MRI unit, the radioactive materials license must be added to the authorized user of the practice or amended to include 511-keV emitters. Conversely, the safety requirements of an MRI facility provide restrictions on how and where the PET/MRI system should be installed (5,6). It is essential to properly plan the facility’s layout in consideration of the typically 3-T superconducting magnets.
If the planned PET/MRI facility is not colocated with an existing nuclear medicine facility, planning needs to accommodate the scanner requirements, radiopharmacy or hot laboratory, uptake rooms, and waiting rooms, as well as the appropriate building permits, local and regional health department clearances, and licenses. Establishing a hot laboratory has been previously detailed (7), and the regulatory requirements have been outlined through the Nuclear Regulatory Commission (8). These requirements include the direction of the facility’s radiation safety officer in overall radiation safety design.
Site Development
One of the first considerations in developing a PET/MRI facility is to determine where to place the system, and this will depend on the type of system being installed. Developing a PET/MRI facility should accommodate the workflow the facility anticipates and should be guided by a “working from the outside in” approach. As with any site installation or major equipment upgrade in radiology and nuclear medicine, coordination and planning require engagement of an internal contractor and architect project team. Suitability testing of the environment is essential, including vibration suitability and magnetic homogeneity. For example, the metal associated with moving elevators can produce artifacts. Equipment vendors generally provide checklists that include such items as permits, clear access to the magnet room free of hazards, cooled water supply, power supplies, and other vendor specifications. Site preparation is essential and more detailed than for the installation of PET or PET/CT. There are several basic steps associated with establishing a PET/MRI facility: site selection, design and construction contracts, site evaluation, planning and design drawings, procurement of permits, construction, and then system delivery, installation, training and commissioning. It is important to keep in mind that, for PET/MRI, a stepwise plan requires the integration of radiation shielding and planning by a qualified radiation health physicist. This step is essential because the radiation management plan may impact site suitability or site location for the PET/MRI installation; a suitable MRI site may not be suitable for PET/MRI, and likewise, a suitable PET/CT site may not be suitable for PET/MRI.
Shielding
Shielding is an essential design requirement to contain and exclude. That is, shielding must be able to restrict both the magnetic field and radiation emission to the scanning room at the same time as preventing external electromagnetic signals or radiation from penetrating the room and creating interference. To that end, lead shielding in the walls is required for the scanner room, the uptake rooms, and the radiopharmacy.
To maintain a homogeneous magnetic field and restrict the magnetic field to the scanning room, it is essential to introduce radiofrequency shielding to all 6 sides of the scanning room. The primary concern with any magnet installation is the limits of the 5-G line (0.5 mT), in that this perimeter is the last point of safety as the magnet is approached and magnetic field strength increases. The 5-G line is the minimum safe distance of patients with a pacemaker and implantable cardioverter defibrillator devices (Fig. 1, left) because these devices are likely to be compromised by the static magnetic field (9). To prevent accidental introduction into the 5-G line, the perimeter is constrained within the technologist-only accessible doorway leading to the magnet room. As per vendor specifications, if a secure doorway is not possible then another barrier must be placed, for instance, a metal-detecting automatically operated gate. Figure 1 (right) provides an example of a secure door with signage, warning signs, and an automatically triggered ferromagnetic detector. An additional recommended safety measure is the installation of a ferromagnetic detector at the magnet doorway. As an additional level of safety, a ferromagnetic detector system could also be placed at the entrance to the restricted zone (zone 2 or zone 3 screening point).

On the left is secure MRI doorway with ferromagnetic detector and 5-G line demarcated by floor color change and roof lighting. On the right is example of secure PET/MRI door with zone 4 signage, wall-mounted ferromagnetic detector, and pregnancy sign. (Courtesy of New York–Presbyterian Cornell Weill Medical Center and Memorial Sloan Kettering Cancer Center.)
At the 1-G (0.1 mT) limit, the magnetic field can affect electronic equipment that is not intended to function within the fringe field, such as computer monitors. Today, manufacturers have created contrast injectors, patient-monitoring devices, and medicine pumps that function appropriately within the 5-G line, but a computer monitor will suffer deleterious effects in a 1-G field. Magnetism, similarly to radioactivity, is not linear and transmits in all directions. Figure 2 illustrates the influence of magnetism in a typical department design, including the fringe fields and impact on the surrounding environment. These representations are before the room being supported with fringe-field containment, more commonly known as radiofrequency shielding. The magnetic field strength at the foot of a fully retracted imaging table reaches greater than 200 G, and the center of the bore surpasses 2,000 G. A nuclear medicine scanner will be affected by as low as 0.5 G. The complexities of how the PET imaging equipment avoids this phenomenon will be detailed in part 2 of this series. For PET/MRI itself, the walls have 4 layers of shielding, with the outer layer being lead for radiation shielding, followed by steel for magnetic shielding, and then air for acoustic shielding. The inner shielding is copper for radiofrequency shielding.

Typical PET/MRI footprint with gauss lines for 200 G (blue); 100 G (solid red); 50, 10, and 5 G (all dashed red); and 3 and 1 G (dashed green).
Facility Layout
An MRI facility is based on 4 safety zones developed by the American College of Radiology as depicted in Figure 3. It should be kept in mind that a PET/MRI facility will have additional radiation zones associated with waiting rooms, uptake rooms, and the radiopharmacy. This approach to partitioning the facility prevents the accidental introduction of unsafe metals or unauthorized staff, patients, or members of the general public into the MRI room. MRI zoning can be thought of as a multilevel filtration system, with the end goal of all metal having been removed and all implants, devices, and equipment having been cleared for the appropriate magnetic strength. All properly established MRI facilities label the rooms by both the zone number and the name of the zone. This extends to PET/MRI facilities. Besides providing a degree of radiation safety, these zones are also an effective means for infection control (10).

Example of signage used to demarcate MRI zones. Color coding can be used on floor plans and emergency exit plans for first responders, and color-coded floor tape and door trim can be used to help identify zones.
Zone 1 represents the area outside the facility at the entrance to the waiting or reception area and is accessible to the general public. By extension, this is the same area in a PET/MRI department. Zone 1 is the point at which the patient makes first contact with MRI staff, who provide the patient with standard MRI documentation relating to the exam (e.g., information relating to what to expect during the MRI procedure or the risks associated with gadolinium-based contrast agents), and paperwork and consent are completed here. The most important form for the MRI patient is the MRI screening form, which will be discussed in detail in part 3 of this series. For this article, it is essential that the reader understand that the form is to be reviewed by all staff who contact the patient, beginning with the front desk personnel, who can advise the patient or alert the nursing and technologist staff to information that the patient provided on the form. Zone 3 is the control room, to which access is restricted. Access needs to be controlled by an effective means that can be differentiated by both approved and nonapproved personnel. Zone 4 is the magnet room, where access is tightly restricted, including through signage and physical barriers. Zones 3 and 4, like zone 1, are the same for MRI as for PET/MRI.
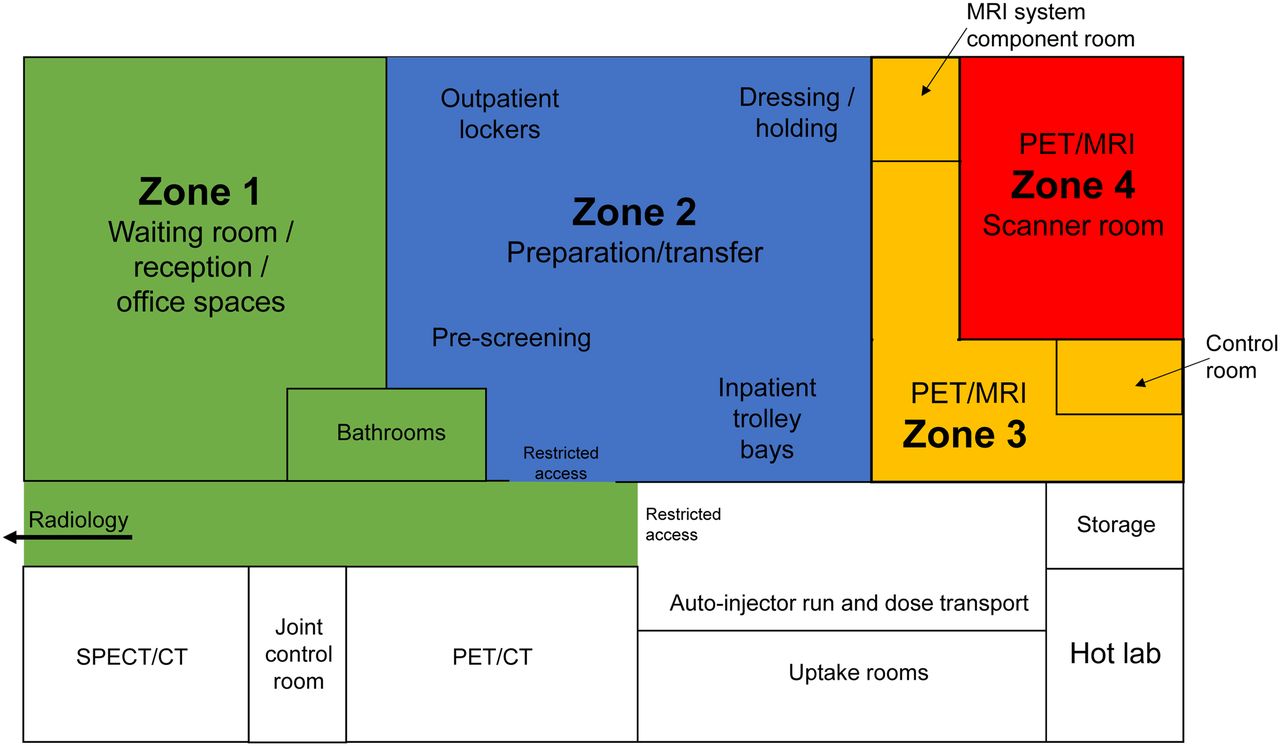
Zone 2 might be thought of as the most important. Zone 2 is the area between zone 1 and zones 3 and 4. Patients or others move through zone 2 to either the control room or the magnet room under the direct supervision of MRI-trained staff. In PET/MRI, zone 2 might also include the PET patient waiting area, radioactive toilets, and uptake rooms. The radiopharmacy or hot laboratory is then the only part of a PET/MRI department not covered under the 4 zone system, but clearly, restricted access as for zone 3 applies. Nonetheless, given the complexity of magnet fields and radiation exposure in a PET/MRI facility, these zones can be translated into an MRI floor plan (Fig. 4). Zone 2 includes the patient dressing area and the inpatient curtain bay area. Zone 2 is the point where the screening form is completed with the patient, where patients can ask additional questions, and in some cases where screening with a handheld or pillar-type metal detector takes place (11). Additionally, all non-MRI staff are screened in zone 2 by performing the same activities as patients, completing the MRI safety form and placing into lockers all metal objects, including pagers, mobile phones, pens, keys, wallets, paper clips, identification badges, stethoscopes, and similar objects.

Schematic of typical department design incorporating PET/MRI highlighting color-coded zones. Noncolored zones are specific to nuclear medicine and will have radiation-based restrictions.
Room Layout
Suggested room dimensions vary among vendors, but facility planners should add approximately 30% to the minimum space requirements to accommodate MRI coils, MRI phantoms, a power injector, a cardiac monitor, anesthesia equipment, positioning and mobilization devices, linens and patient comfort items, and space to allow free movement of multiple staff. The typical design should have ready access to the radiopharmacy and the injection or uptake rooms while being isolated from other electromagnetically sensitive equipment (Fig. 4). The design should consider restricting access to zones 2, 3, and 4 and the radiation zones.
SAFETY FACTORS
MRI
When planning a PET/MRI facility, one needs to accommodate the general safety considerations for a standard MRI system. These include the magnetic fringe field and static magnetic field discussed previously. The inner 3 layers of shielding help mitigate some of these safety issues. The radiofrequency shielding (inner layer) typically uses copper to prevent interference within the PET/MRI suite from external electromagnetic sources. The steel shielding contains the magnetic fringe field within the suite. MRI produces airborne and structural noise. The air layer of shielding helps to reduce the noise produced by the MRI scanner, but with noise in the range of 80–120 dBA (equivalent to a jackhammer), planning is essential to minimize the impact of MRI on noise-sensitive equipment or hospital functions. Other than the air layer in the shielding layers, the door and ceiling material should offer acoustic attenuation, ducting between the connecting rooms should be minimized, and the suite should be buffered from adjacent noise-sensitive areas. Structural noise can be reduced during planning with the inclusion of isolation joints or elastomeric elements. Despite the planning, ear protection is mandatory during procedures for patients. MRI scanners are particularly susceptible to vibration, including levels lower than are detectable by humans. Vibration may be associated with internal footfalls (people walking in the area) and building elevators, external road traffic, building works, and rail traffic or may be intrinsic and associated with scanner-generated vibration. Planning requires a rigorous vibration survey to allow an optimal floor design that includes vibration isolation pads. MRI also produces safety concerns associated with a potential helium quench. The helium venting system must comprise components functionally robust under helium gas temperatures (12°K or −260°C). Furthermore, the design needs to accommodate the 1,000-N forces (helium exit, expansion on evaporation) expected during a quench. The exit to the environment needs to be positioned so as to be inaccessible to people (e.g., 5 m above walking access) and should not be located near operating windows or air intakes. Regardless of the design, clear signage should be used.
PET
Over and above the safety issues typical for designing an MRI facility, the addition of PET to the PET/MRI hybrid system adds a layer of complexity to safety. The primary issue relates to ionizing radiation, which is not a consideration for standard MRI. Shielding the scanning room and radiopharmacy is an obvious requirement, but use of secondary waiting rooms to keep radioactive patients separated from others, uptake rooms, and separate bathroom facilities should also be part of planning considerations. The outer layer of shielding of a PET/MRI suite is typically lead to attenuate radiation. This layer functions in both directions, shielding the outside environment from the patient and protecting the PET system from external radioactive interference. In many cases, this design will need to accommodate the presence or absence of existing nuclear medicine facilities.
Signage
Signage plays an important role in a PET/MRI facility, ensuring adherence to health department and Nuclear Regulatory Commission codes. Included is nuclear medicine signage relating to radioactive materials, hot zones, restricted zones, bathroom facilities, waiting areas, and pregnancy status. Signage also includes MRI signage relating to the 4 MRI zones (zone 1, or general public area outside the MRI environment; zone 2, or path patients are brought through for their procedure between zones 1 and 4; zone 3, or control room; and zone 4, or magnet room), and warning signs such as “Magnet Always On,” “Do Not Enter,” and “Authorized Personnel Only.” These should be displayed according to the recommendations of national authorities such as the American College of Radiology and the Joint Commission on Accreditation of Health Care Organizations. For PET/MRI, the MRI zones also afford the opportunity to develop radiation-safety restricted-access zones, especially radiopharmacy and scanner rooms.
STAFFING FACTORS
PET/MRI is essentially a new modality, and it is relevant to consider the type of personnel involved in a facility that combines PET and MRI, most notably because of the unique radiation and MRI safety considerations (2,12,13). The requirements for an MRI facility are based on staff and patient restrictions through MRI safety education. Implementation of a thorough MRI safety program is based on a multitiered approach, beginning with the front-desk staff, the MRI safety officer, the physician on duty, the nursing staff, and the final checkpoint: the imaging technologist who performs the final screening. This is necessary to ensure that the patient is free of unsafe implants, that conditional implants are imaged appropriately at the correct magnetic field strength and heating parameters, and that the patient is free of personal items, medication patches, and external devices, such as cardiac monitors, temperature probes, and unsafe electrocardiography leads. This is not an inclusive list, and an MRI facility should consult its MRI safety officer for a complete list of all unsafe devices or patient adjuncts. Not all sites will have a designated MRI safety officer, but all sites should have staff who assume the role and responsibilities. It is essential to understand the importance of, and responsibilities for, MRI safety in each department.
The requirements of a PET facility are focused on radiation shielding and on a radiopharmacy or secure area where radiopharmaceuticals can be stored. Personnel involved in all aspects of handling, administering, cleaning, assessing, and maintaining radiation safety must be properly trained to perform such tasks. The ideal personnel with training inclusive of these tasks is the nuclear medicine technologist (NMT), who is registered and, in many regions, licensed to perform these functions. Staff who lack NMT training and registration but continue to perform these functions are working outside the scope of their licensure.
PET/CT confronts similar challenges. In many departments, a patient and the PET/CT equipment are managed by 2 staff members: a qualified NMT (PET) and a qualified radiographer (CT). The opportunity for dual qualification is attractive for both employer and employee. Practices vary globally, but some radiographers have undertaken additional training to be registered or licensed to perform PET. In some instances, an NMT can receive additional training to perform diagnostic CT. Both radiographers and NMTs are well suited to receive the additional training in MRI. Given that NMTs are already qualified for PET, it is a simpler process for an NMT to train in MRI than for a radiographer to train in both MRI and PET. Regardless of who is trained, it is essential that all PET/MRI staff be well trained in the safety aspects of both PET and MRI, including radiopharmaceuticals and contrast agents. Specifically, all staff must be equipped to respond to a health emergency in the patient, a fire emergency, a helium quench, a radiofrequency burn, a projectile risk, a contrast reaction, radiation area surveys and spills, patient contamination, and security threats within the constraints of a PET/MRI facility. Although safety training and procedural training for PET/MRI staff are critical, it is also important to provide appropriate training for all staff working in or near the PET/MRI facility. This training includes safety training for maintenance staff, janitorial staff, administrative staff, and orderlies.
CONCLUSION
Hybrid imaging with PET/MRI has an important role in patient management, and this role will be explored in more detail in part 4 of this series. Success with PET/MRI requires careful planning for facility siting and design to overcome the challenges and safety considerations posed by each modality individually or in combination. Specific design features of PET/MRI will be detailed in part 2 of this series. The synergistic relationship evident in PET/MRI affords an opportunity for integration into broader patient management (e.g., radiation therapy and surgery), and this potential needs consideration in department planning. Managing the establishment of a PET/MRI facility with respect to engineering, safety, and staffing requires careful, proactive, and holistic PET/MRI facility design.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 15, 2021.
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than June 2024. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
REFERENCES
- Received for publication December 2, 2020.
- Accepted for publication February 6, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- PET-MRI for evaluation of response to radiochemotherapy in patients with locally advanced cervical cancer
- PET-MRI for evaluation of response to radiochemotherapy in patients with locally advanced cervical cancer
- PET/MRI, Part 4: Clinical Applications
- PET/MRI, Part 2: Technologic Principles
- Virtually Celebrating the Advances of Nuclear Medicine and Molecular Imaging: 2021