


Abstract
Pakistan is a country with nuclear capability in a region sharing borders with 2 other nuclear powers—that is, India to the east and China to the northeast. This geographic positioning makes the area a nuclear flash point. It is therefore imperative to have commensurate health-care facilities to meet any eventualities. Although Pakistan is trying to improve medical facilities for the people, health-care facilities are already overwhelmed with patients because of the large population of the country. The current study was conducted to evaluate the level of awareness and preparedness of medical responders for nuclear and radiological disasters in public hospitals in the major cities of Pakistan. Methods: A detailed questionnaire covering all aspects of the study was designed and discussed with the people most concerned, including health-care workers in the field of medicine, nuclear sciences, and disaster management in Pakistan. It was adopted on the basis of early studies on the subject, with necessary modifications to fulfill the requirements at Pakistan’s level. Semistructured interviews were also conducted with key personnel of different response agencies in Pakistan. Results: Of 880 surveys, 554 were completed and collected from medical providers in different hospitals across the country. The respondents included doctors, nurses, and medical assistants from emergency and nonemergency departments. They are aware of the catastrophic consequences of nuclear disaster and are willing to respond to these kinds of disasters voluntarily, but they are not satisfied with their level of preparedness and awareness regarding nuclear and radiological disasters. Conclusion: Although medical responders have good educational backgrounds and knowledge in their specific fields and are quite active and energetic in their response to conventional injuries and natural disasters, they feel a dire need to enhance their level of knowledge about and preparedness for unconventional disasters and injuries such as those caused by nuclear or radiological events.
Any disaster can be complicated to handle, but a nuclear disaster requires even more complex management apparatus. We live in a world where nuclear weapon issues are on the front pages of our newspapers on a regular basis. Some people think that nuclear weapons destroy everything in the world, with unimaginable damage to life and infrastructure, whereas others think that they are not much different from conventional weapons. The reality, however, is somewhere between the 2 arguments. Nuclear weapons can cause immense damage and huge losses of life, but the effects are still comprehensible on a human scale. It is also believed that the most destructive technology ever invented by human beings is the nuclear weapon. A conflict anywhere in the world leading to the use of nuclear weapons would bring unavoidable destruction and human suffering. The magnitude of the destruction represented by nuclear weapons is difficult to imagine—a scale of violence that most people would have difficulty rationalizing (1). In both Hiroshima and Nagasaki, 50% of the people within 1.2 km (three quarters of a mile) of the hypocenter died on the day of the explosion, and 80%–100% of those exposed at this distance eventually died from wounds or radiation inflicted by the bomb (2). After the Chernobyl incident, approximately 5 million people in the region may have had excessive radiation exposure, primarily through internal contamination, as such nuclear reactor accidents can release a variety of radioisotopes into the environment (3). If a large-scale nuclear war breaks out, the atmosphere would be contaminated with huge quantities of radioactive pollutants. These pollutants would be injected in the atmosphere through fires in urban and industrial centers, cultivated lands, forests, and grasslands. The combined effect of lack of sunlight, frost, and other adverse meteorologic conditions would add enormously to the already huge problems of the survivors. The presumed effect would be large areas under extreme darkness and reduced crop growth and biospheric productivity (4).
Because of the tense relationship between the nuclear weapon–armed neighboring countries Pakistan and India, there is a chance of nuclear escalation that could lead to catastrophic circumstances not only for the 2 countries but also for the South Asian region. Negative health effects would be gigantic and might exceed the normal handling capability of medical responders in the affected areas. In the case of such a troublesome incident, the demands on the medical system would be vast and overwhelming, all the more so because the nuclear disaster would have destroyed much of the capacity to respond. Furthermore, it is important to assess the patient-handling capability of hospitals and the knowledge of local medical providers about the negative health effects and the procedures to treat patients affected by nuclear contamination. Accumulated evidence about radiation health effects on atomic bomb survivors and other radiation-exposed people have formed the basis for national and international regulations about radiation protection (5).
When health workers have a poor level of preparedness for nuclear disaster, they feel anxiety, which can be reduced by maintaining coordination and cooperation with them (6). If an incident involving nuclear or radiological elements occurs, people are expected to rush toward hospitals. All hospital emergency departments must therefore have a radiological emergency plan, tested through vigorous and regular drills. Under these situations, medical responders should have a clear understanding that patients with conventional injuries must be treated first, followed by those with radiological injuries (7,8). The growing tension between Pakistan and India on the conflict over Jammu and Kashmir can lead to a limited war followed by nuclear conflict between these 2 countries (9). The U.S. Secretary of Defense warned the world about the negative consequences of a nuclear exchange between the 2 countries (10). Modeling of an India–Pakistan regional nuclear war suggests that the burning effects of nuclear disaster would create an extensive level of soot and have considerable negative effects on the climate (11).
It is therefore important for the countries to have a broad and balanced program of preventive and preparedness measures. Such measures require improvements in intelligence and strengthening of emergency-services preparations and the public health system (12). The health consequences of nuclear, biological, and chemical agents have a greater priority than conventional injuries. The response to nuclear, biological, and chemical attack needs greater collaboration between responding agencies and medical professionals. In the event of any nuclear terrorism event, hospitals would be overwhelmed and medical providers unable to handle victims carrying nuclear contamination. The result would be an increase in the number of casualties and spread of contamination (13). Effective strategies, including policy decisions, public education, efficient and elaborate medical preparedness, and interventions, are required to deal with massive nuclear or radiological events (14). Training on handling patients affected by nuclear disaster is becoming an important part of education. The International Atomic Energy Agency has repeatedly asked these countries to prepare their emergency plans and conduct regular training sessions on nuclear emergencies (15).
The level of preparedness for nuclear disaster is not high in the world. After a nuclear emergency, injuries would mainly be thermal burns, trauma, and radiation injuries. All these categories can result in a large number of casualties and may greatly reduce the ability of medical providers to efficiently handle the situation. The medical community is not fully knowledgeable about and prepared to handle casualties carrying nuclear contamination (16). Under the present situation, it is important to enhance understanding at all levels about preparedness for nuclear disaster. The main target of such efforts should be the safety of medical first responders in public hospitals in the major cities of Pakistan. Because these first responders will encounter the threat while facing all odds, it is vital that they be kept educated, motivated, and fully aware of the situation. The goal of the current study was therefore to evaluate their present levels of awareness and preparedness regarding nuclear and radiological disasters.
MATERIALS AND METHODS
Primary data were collected through a detailed questionnaire, which was designed in collaboration with professionals in the fields of medicine, nuclear sciences, and disaster management. The questionnaire was based on early studies on the subject, with modifications to fulfill the requirements at Pakistan’s level (16), and was pretested before it was distributed to medical responders in selected major public hospitals in the capital city from each province in Pakistan. These cities included Islamabad, Rawalpindi, Lahore, Peshawar, Quetta, and Karachi.
The target groups for the questionnaire were doctors, nurses, and medical assistants. The focus was on identifying the concepts and principles of medical responders regarding clinical management of casualties during a nuclear or radiological disaster and the resulting public health emergency.
Besides the questionnaire, semistructured interviews were conducted with departmental heads and experts in related services, such as the Rescue 1122 Emergency Service, the National Disaster Management Authority (NDMA), and the National Health Emergency Preparedness and Response Network (NHEPRN). To varying degrees and at various levels, these people have an impact on the decision-making process. Interviews of these individuals were subject to their relevancy and relativity to the study, their availability, and their accessibility to the researcher and were conducted by visiting them in their offices and departments.
The collected data were evaluated and interpreted through direct and structured techniques.
RESULTS
The results of this study are summarized in Table 1. Of 880 questionnaires distributed, 554 (62.9%) were completed correctly, 76 (8.6%) were incomplete and not included in the results, and 250 (28.4%) were not returned.
Summary of Findings
Demographics
The demographic distribution maintained an almost equal representation among doctors, nurses, and medical assistants, at 36%, 35%, and 29%, respectively. Almost half the respondents (48%) were young, between 20 and 30 y of age, whereas 45% were between 30 and 40 y and were found to be more experienced and educated in their fields. Almost half the respondents (51%) were graduates, 6% held diplomas in medical emergency management, 22% were undergraduates, and 21% had postgraduate qualifications.
It was found that 24% of respondents were from Karachi, 24% from Lahore, 20% from Peshawar, 12% from Quetta, and 20% from Islamabad and Rawalpindi (Fig. 1).
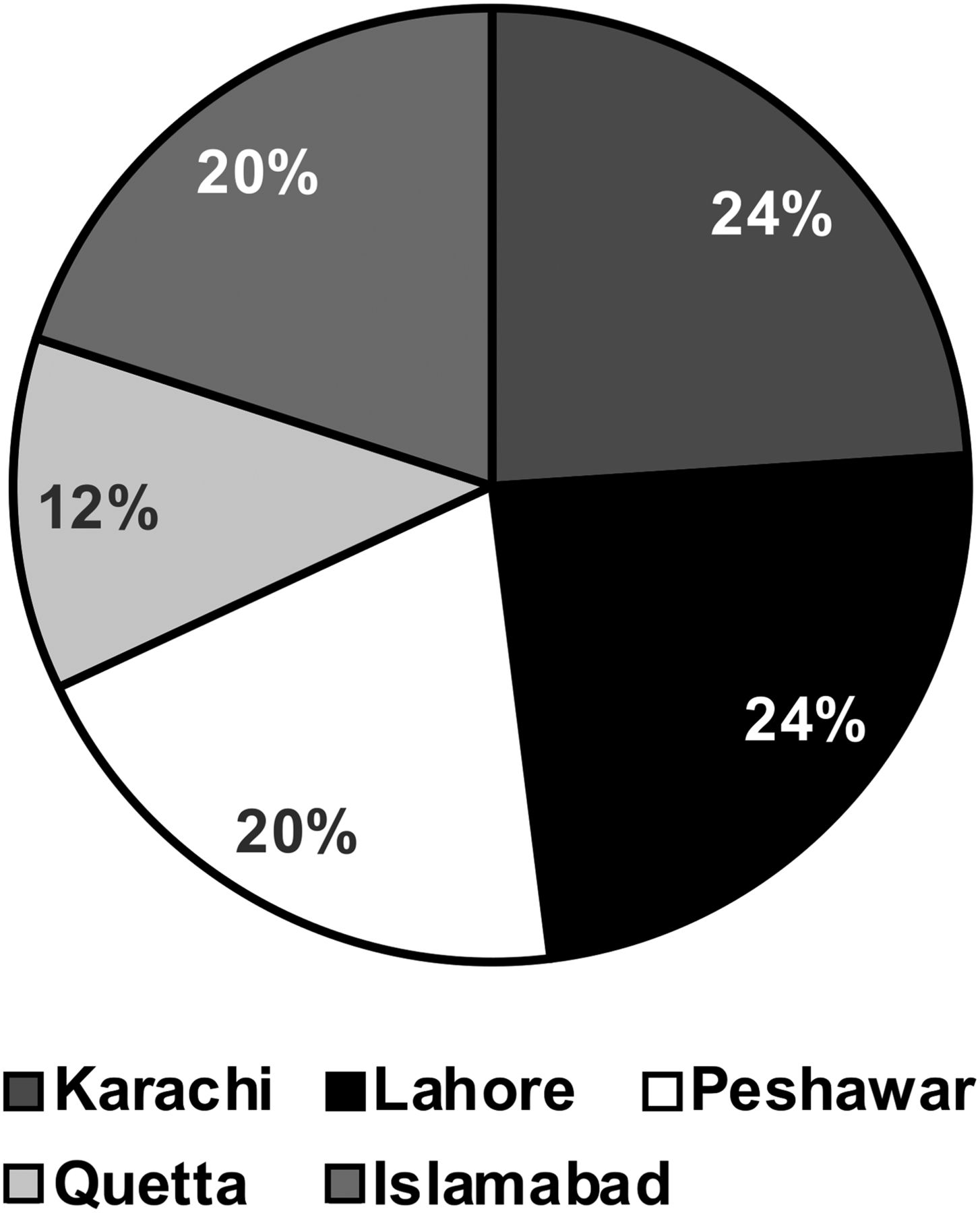
Participation of responders from different cities.
Knowledge About Nuclear and Radiological Decontamination
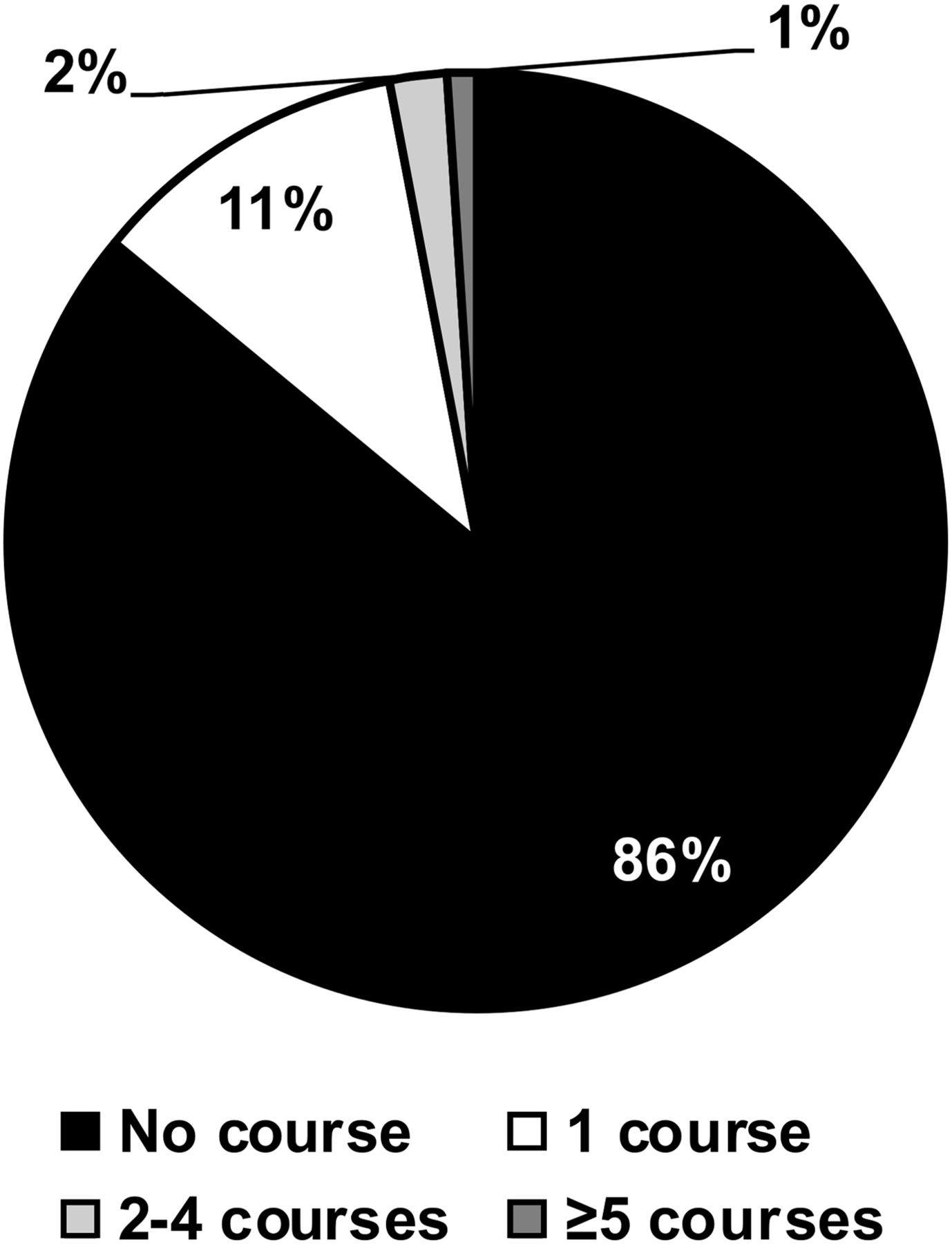
Regarding the number of educational courses taken with specific nuclear or radiological content, 86% of respondents had never taken a course on nuclear emergency management, 11% had taken 1 course, 2% had taken 2–4 courses, and 1% had taken 5 or more courses (Fig. 2).
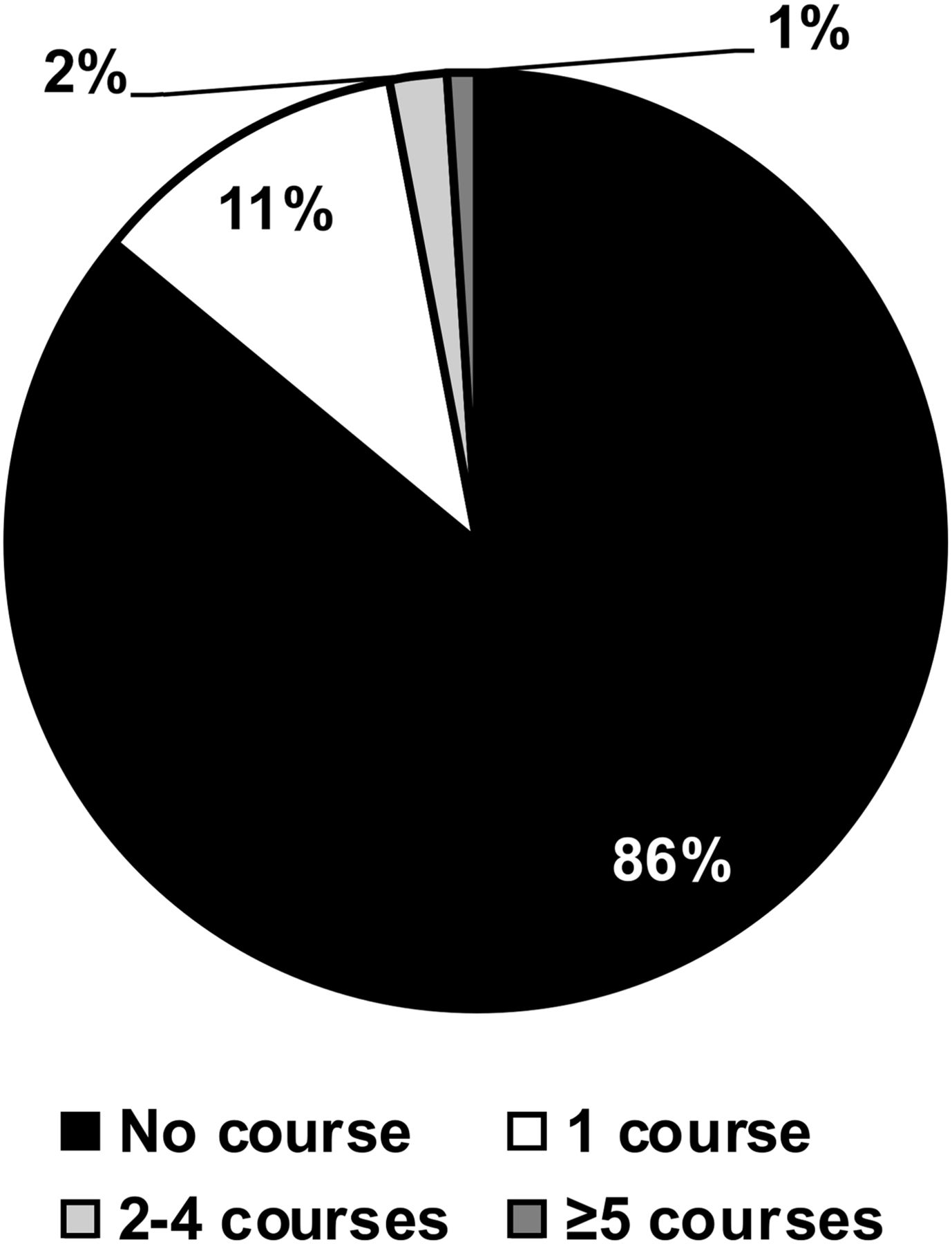
Number of educational courses taken by medical responders on nuclear or radiological management of patients.
Seventy-six percent of respondents knew the symptoms of acute radiation syndrome. Half (50%) were aware of the different levels of personal protective equipment, and most (87%) were aware of the requirement for and importance of decontamination of patients arriving at hospitals after a nuclear or radiological disaster.
Regarding the type of decontamination they would prefer to do on affected people before starting medical treatment, 47% of respondents preferred removal of the patient’s clothing as a decontamination option, and 35% favored the use of a decontamination solution on the patient. The option of rinsing the patient with water was favored by 13%. However, 5% felt no need for decontamination and that the patient should be treated as a normal case (Fig. 3).
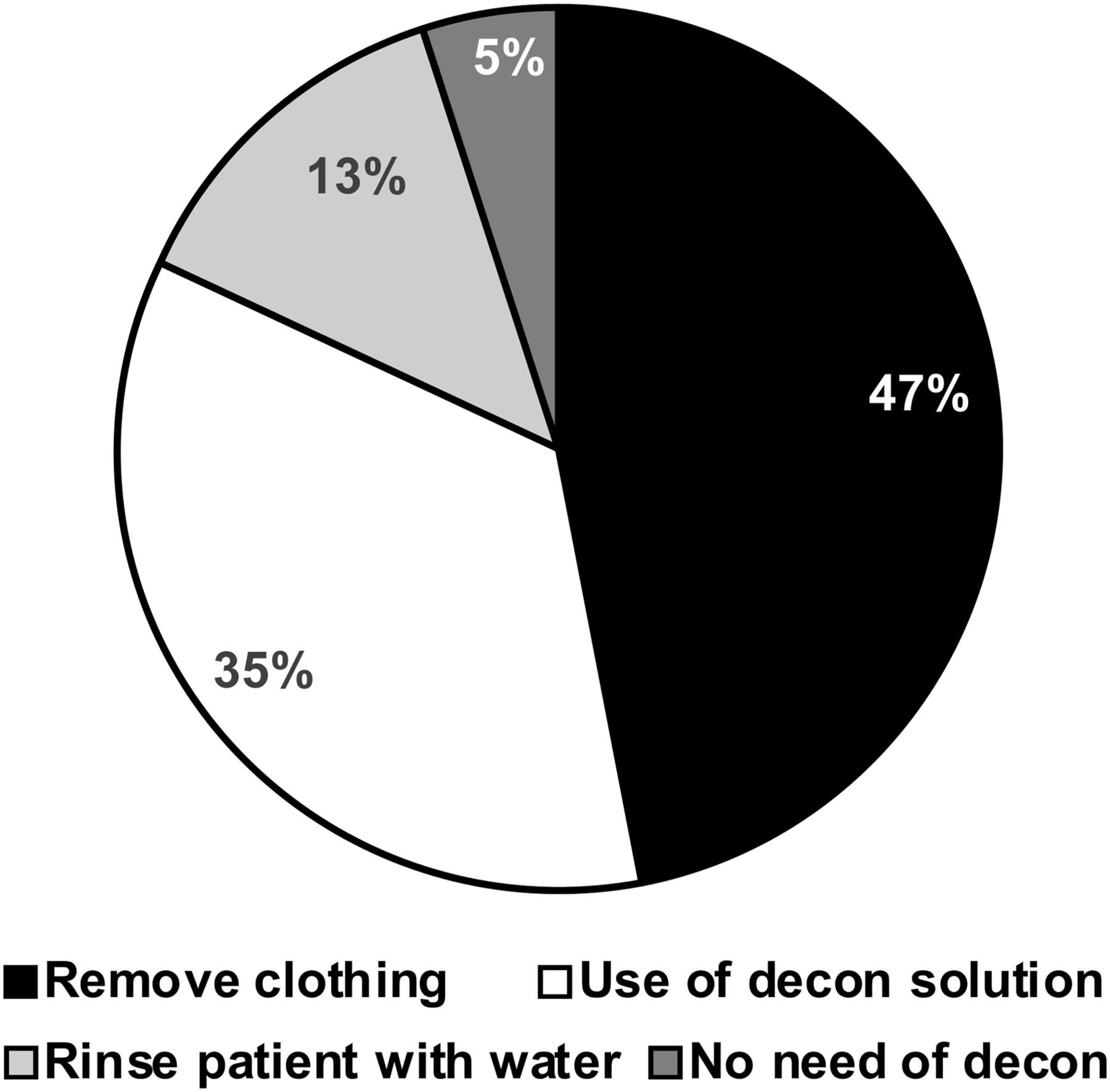
Level of knowledge of medical responders on nuclear or radiological decontamination (decon).
Knowledge About the Effects of Nuclear and Radiological Incidents
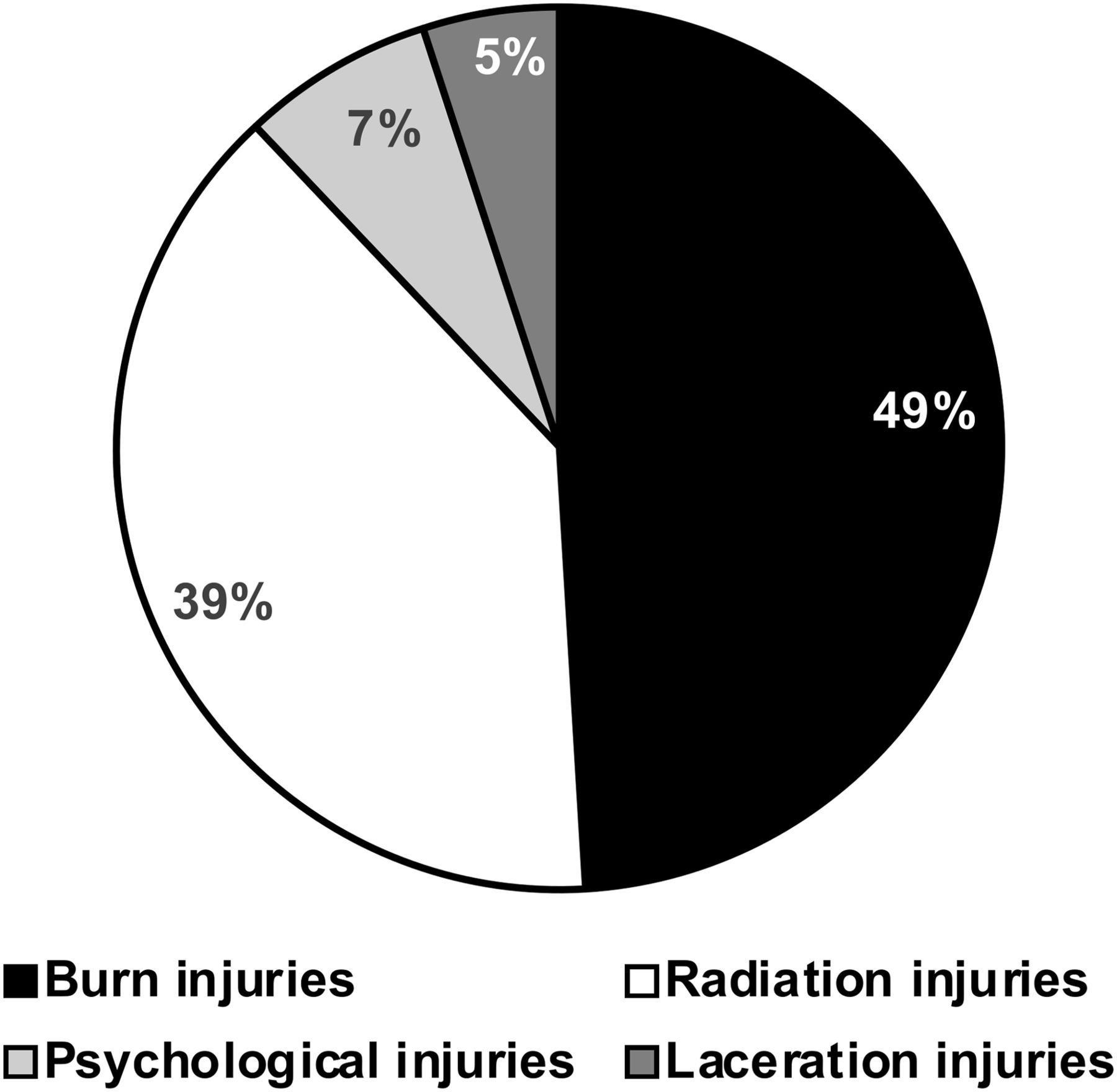
To learn how aware medical responders are of the types of injuries after a nuclear detonation, we gave them different options to choose from based on injury severity. Burn injuries were selected as the most dominant and severe (49%), followed by radiation injuries (39%), psychological injuries (7%), and laceration (scratch) injuries (5%) (Fig. 4).

Level of knowledge of medical responders on types of injuries after nuclear or radiological incidents.
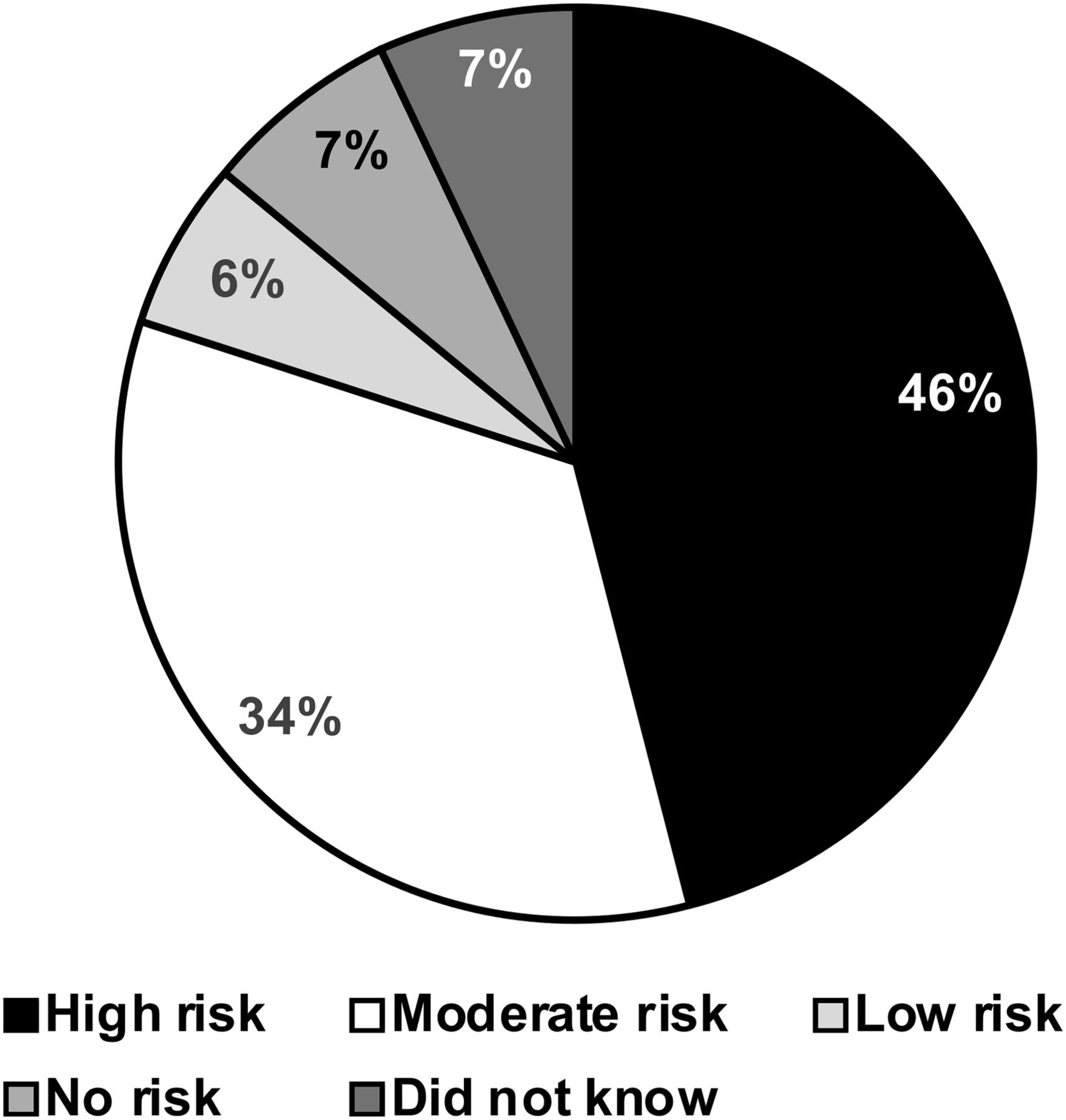
After a nuclear incident, victims may be contaminated with radioisotopes that are harmful to other individuals caring for them. Respondents were asked to estimate their own risk of exposure to nuclear contamination while handling such patients; 46% thought their exposure would be high, 34% moderate, 6% low, and 7% nil. Seven percent were not clear about their possible level of exposure (Fig. 5).
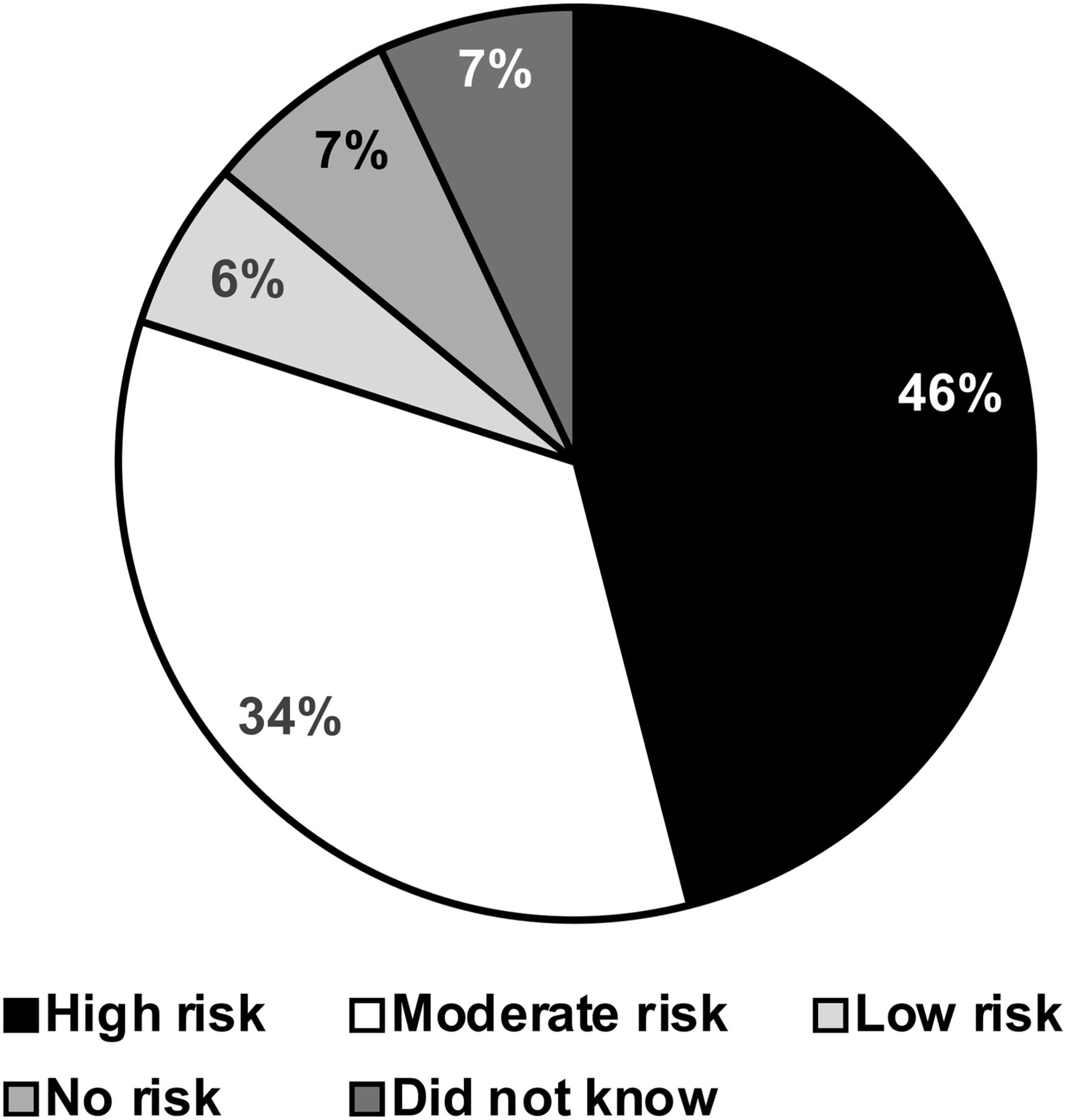
Level of knowledge of medical responders on risks of self-contamination while handling contaminated patients.
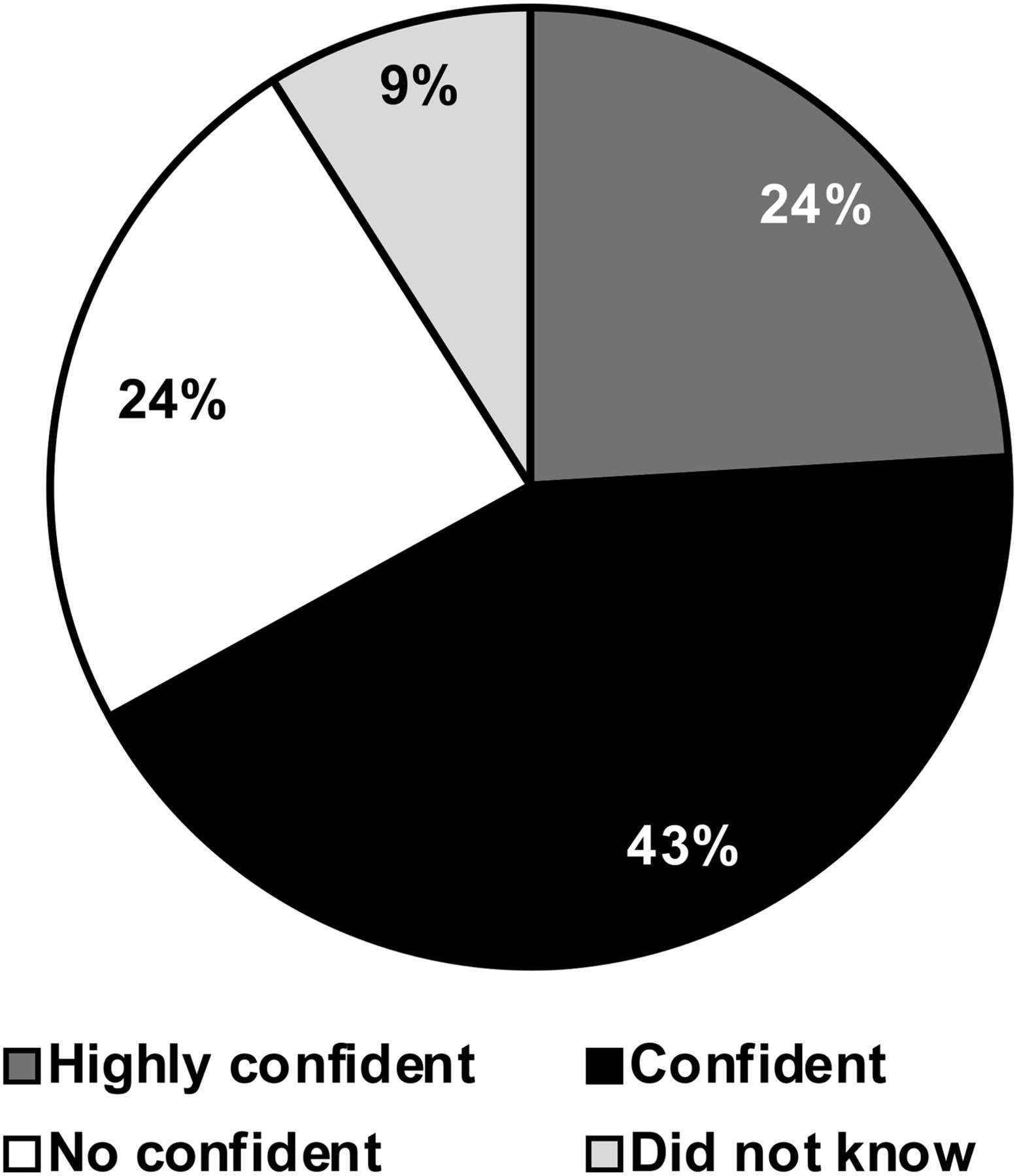
On the basis of their educational qualifications, the nature of their duties, and the number of continuing education courses they had taken, respondents were asked about their level of confidence in handling patients carrying nuclear contamination; 43% felt confident, 24% highly confident, and 24% not confident. Nine percent were not able to estimate their level of confidence (Fig. 6).
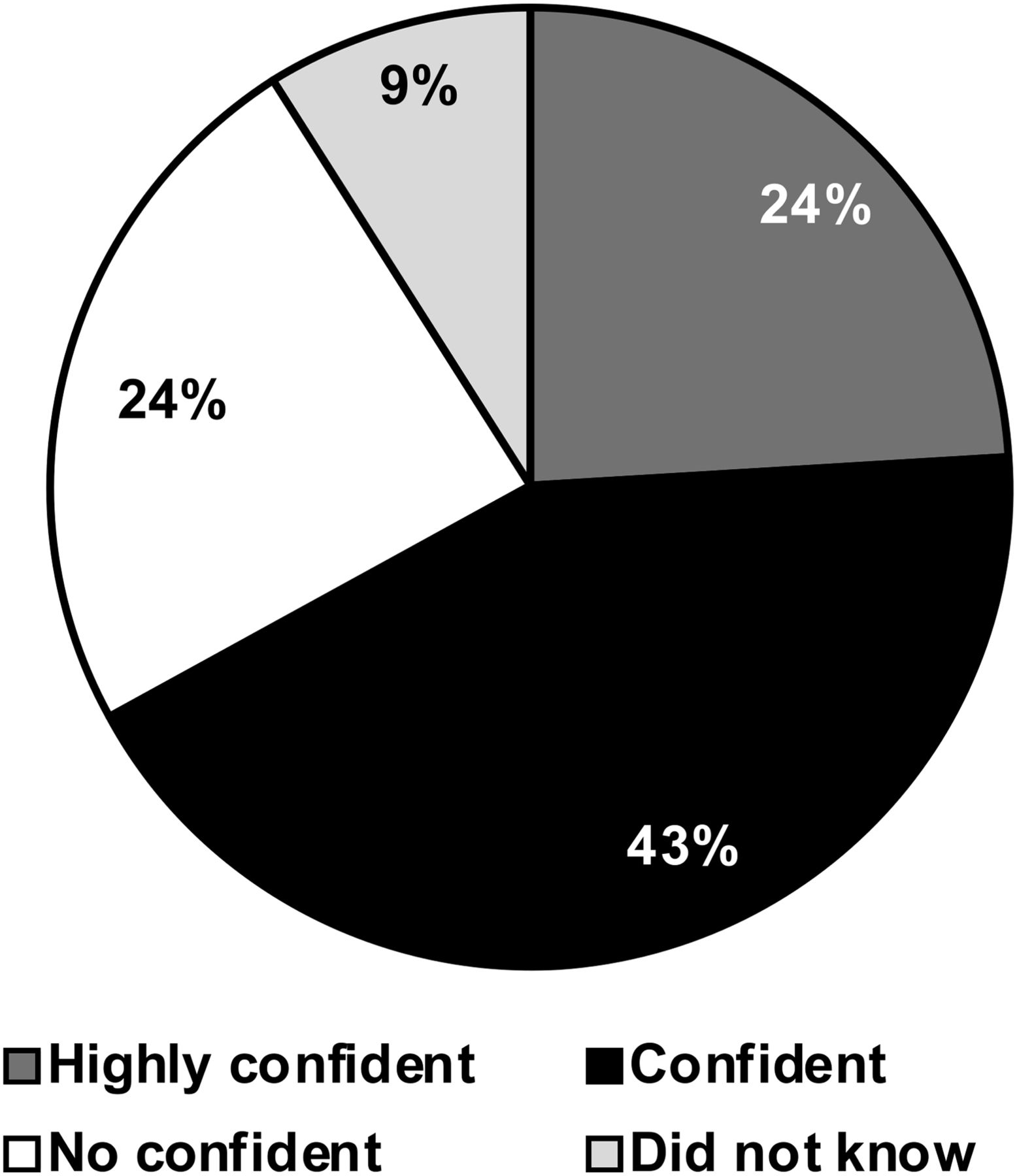
Level of confidence among medical responders in handling nuclear or radiological contaminated patients.
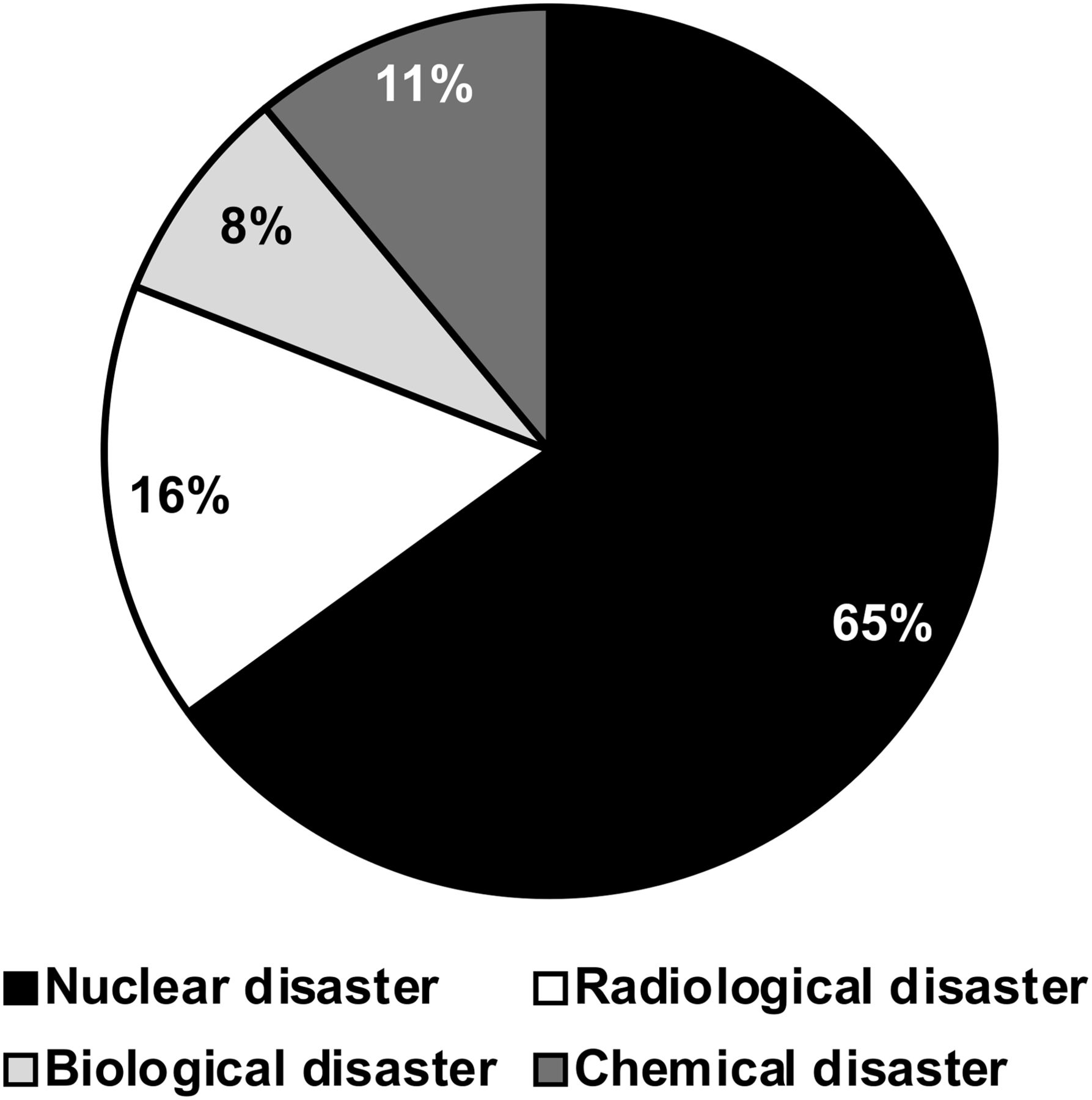
Respondents were also asked about their basic knowledge of the relative severity of chemical, biological, radiological, and nuclear disasters. Most (60%) thought nuclear disaster to be the most catastrophic event, followed by radiological disaster (26%), biological disaster (10%), and chemical disaster (4%). They were further asked to rank these 4 types of disaster on the basis of the level of difficulty in handling them. The highest ranking was given to nuclear disaster (65%), followed by radiological disaster (16%), chemical disaster (11%), and biological disaster (8%) (Fig. 7).

Ranking of disasters with respect to difficulty in handling by medical responders.
The survey revealed that 83% of respondents were aware of the medical effects of nuclear and radiological disasters on the human body, and 60% had studied the medical effects of the nuclear bomb attack on the people of Hiroshima and Nagasaki. However, only 22% were trained to handle contaminated patients.
Willingness to Manage Contaminated Patients
When asked about their willingness to treat patients after a nuclear incident, even if not trained in this field, 80% of respondents were willing. When asked about their willingness to volunteer on an emergency response team to treat contaminated casualties in the area of the disaster, 90% were willing. When asked about their willingness to continue treating patients at their workplace after a nuclear or radiological emergency in the area, 79% were willing.
Familiarity with Disaster Management System in Pakistan
Respondents were asked about their familiarity with the different emergency response agencies and authorities working in Pakistan. Fifty-six percent were aware of the response teams in the country or province, and 49% were aware of the role and tasks of the NDMA. When asked which agency would respond first to give medical assistance in the event of a nuclear disaster or emergency, respondents gave the highest ranking to the military (39%), followed by the Rescue 1122 Emergency Service (23%), the NDMA and provincial disaster management authority (22%), and the Edhi Foundation and Chhipa Association (16%). When further asked which disaster response team would act as the first responder after a nuclear or radiological disaster in Pakistan, respondents gave the highest ranking to the military (48%), followed by the Rescue 1122 Emergency Service (29%), the NDMA (19%), and international organizations (4%). Only 12% of respondents served on the disaster and emergency response teams in Pakistan.
Semistructured Interviews
In addition to the questionnaire part of the study, semistructured interviews were conducted with the NDMA, the Rescue 1122 Emergency Service, and the NHEPRN to learn the capability of each to effectively respond to nuclear and radiological events.
NDMA
The NDMA is the main response agency in Pakistan, tasked with responding to any kind of disaster. At the federal level, the NDMA acts as the implementing, coordinating, and monitoring body for disaster management. The provincial disaster management authority works as the main responder at the provincial level and also assists at the district level. One interview revealed that although the NDMA is striving diligently to implement, coordinate, and monitor disaster-management activities nationwide, the level of preparedness for nuclear and radiological disasters is not high. The main emphasis of this authority is on managing natural disasters. Because nuclear and radiological disasters are not common, preparedness for such is limited to only a few dedicated organizations and agencies.
Rescue 1122 Emergency Service
The Rescue 1122 Emergency Service helps communities with such issues as medical emergencies, fires, bombings, building collapses, traffic accidents, drownings, flood relief operations, and landslides. The interview revealed that rescuers do not have basic knowledge of nuclear and radiological disasters and do not know how to respond to them. With their present level of awareness and training, the rescuers will become victims to the radiation and nuclear contamination in the area, if they choose to respond first.
NHEPRN
The survey found that the NHEPRN, which has a goal of establishing a network among the various agencies responding to health emergencies, does not have any contingency plans to counter the health effects of a nuclear or radiological disaster. Although the NHEPRN also conducts training on basic and emergency life support skills, it does not have effective communication channels to respond to a health emergency resulting from nuclear or radiological disaster.
DISCUSSION
Because nuclear disasters are not common in the world, not much emphasis is placed on enhancing the level of preparedness, awareness, and training. Emergency services and disaster response teams are more inclined to prepare for forms of disaster that are more common in their area (e.g., earthquakes, floods, cyclones, fires, and traffic accidents).
The survey revealed that respondents were interested in learning more about nuclear disasters, as they thought such an event could happen in their region. Most respondents were young and responded efficiently with great enthusiasm and interest. Almost half had graduate degrees in medical or related fields and were quite aware of the importance of the geographic location of Pakistan and the chance of nuclear escalation in the region. A good number of respondents had postgraduate degrees and generated helpful discussion on the importance of enhancing the level of preparedness among medical responders and response agencies for nuclear and radiological disasters.
The respondents were from both the emergency department and nonemergency hospital departments; 85% had not taken any educational courses on nuclear and radiological safety or treatment of contaminated patients. Courses in this field are not common, and only a very few people were qualified, moderately, to handle patients after such a disaster. This level of training and knowledge may lead to dangerous consequences, as medical responders themselves may become victims after a nuclear disaster, compromising the already overstretched health-care system. Not much emphasis is given to training medical personnel to treat casualties from nuclear and radiological events. Although many respondents were aware of the signs and symptoms of acute radiation syndrome, they were not confident about treating such patients. Most respondents who had received basic training were uncertain about their ability to respond effectively in the time of need, mostly because of a lack of practical training and refresher courses. Over time, the limited theoretic knowledge on handling patients after nuclear incidents will diminish further. Around 50% of respondents were aware of the different levels of personal protective equipment. Most knew the importance of patient decontamination and its significance after a nuclear disaster; however, knowledge about the procedures for using personal protective equipment under such circumstances is not sufficient because little emphasis is placed on the use of this type of equipment, potentially resulting in self-contamination of medical personnel.
Respondents had a good basic understanding of the different types of possible injuries resulting from a nuclear detonation. Most respondents (46%) thought their chance of becoming contaminated from affected people was high.
The study also found that 43% of the respondents felt confident about handling contaminated patients effectively but could not explain the reason for their confidence. Most people who felt confident about handling nuclear disasters were not well trained. Their high level of patriotism and commitment to their profession brought them their confidence. One might surmise that overconfidence about handling patients with nuclear contamination can result in self-contamination as well. Knowledge and level of awareness were also compared among 4 types of unconventional disaster: chemical, biological, radiological, and nuclear. Most respondents (60%) thought that a nuclear event would be most disastrous in terms of physical damage and human fatalities. Twenty-two percent of respondents were found to be trained to some level. Many would volunteer to treat patients if required after any nuclear contingency. They also would volunteer to become part of any emergency team after a local nuclear or radiological incident. Most were willing to continue treating contaminated people at their workplace after a nuclear incident, even at the risk of their own lives. History shows that the people of Pakistan are highly resilient against various types of disasters and emergencies and manage to handle them effectively. This resilience is a tribute to their high level of patriotism and commitment. The present study also found that medical providers are willing to volunteer their services in a time of need.
Most respondents were aware of the different disaster response teams and agencies in Pakistan. Thirty-nine percent were of the view that the first medical response after a nuclear disaster would be given by the military, and almost half (48%) thought that the military would be the first responder after such an eventuality. These results indicate the important role of the military, which for many decades has volunteered to help with all types of disasters. The Kashmir earthquake of 2005 is a recent example (17). One reason for successful rescue operations after that earthquake was the efficient role of the military and the high level of coordination between civil and military establishments in providing humanitarian assistance to the area (18). Most respondents to the survey had never been on a disaster or emergency response team. Because our study focused on the awareness and preparedness of only medical first responders, the capabilities of the military in this context are not discussed here.
CONCLUSION
The complex nature of today’s disasters, particularly regarding weapons of mass destruction, have increased the need for a multidisciplinary medical response. Nuclear and radiological disasters have enormous medical and public health consequences. Medical responders in Pakistan are not appropriately trained for such events and are therefore not confident about handling disasters of such a high magnitude, despite a high level of motivation and dedication. The Pakistan military, being the most disciplined organization in the country, responds first in all kinds of disasters. But the major responsibility should be borne by the different response agencies, which seem to be more inclined toward handling recurring disasters. The level of knowledge and the handling capability of these agencies against nuclear disaster should be enhanced to enable an effective response. For this purpose, as a start, the medical first responders may be encouraged and incentivized to complete World Health Organization online courses. Moreover, national health authorities may seek policy advice and technical support from the World Health Organization on preparedness, response, recovery, and long-term follow-up of populations.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 30, 2020.
REFERENCES
- Received for publication July 4, 2020.
- Accepted for publication October 28, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}