


Abstract
The present study aimed to optimize the injected dose of 18F-FDG in whole-body PET/CT scans and assess its effect on noise-equivalent count rate (NECR) and visual image quality (IQ). Methods: Patients scheduled to undergo 18F-FDG PET/CT were prospectively recruited in the study from January to December 2019, regardless of the indication or underlying disease. Patients were divided into 4 groups and injected with different amounts of 18F-FDG radioactivity per kilogram of body weight (1.85, 3.7, 5.5, and 7.4 MBq/kg). All patients underwent 18F-FDG PET/CT studies, and NECRlocal was calculated by noting the trues rate, total prompts, and randoms rate for each bed position. Whole-body NECRglobal was calculated as the average NECR for all bed positions. IQ was qualitatively assessed for each bed position (IQlocal) and for whole-body PET (IQglobal) by 2 readers using 5-point scores based on prevalence of noise, contrast, and lesion detectability. NECR and IQ were compared among all 4 activity groups. Patients were also subdivided into 4 body-mass-index groups (group I, 15–20 kg/m2; group II, 20.1–25 kg/m2; group III, 25.1–30 kg/m2; and group IV, 30.1–35 kg/m2) for comparison. A P value of less than 0.05 was considered significant. Results: In total, 109 patients underwent 18F-FDG PET/CT studies after injection of different amounts of 18F-FDG radioactivity and a mean uptake time of 62.32 min. The mean NECRglobal and IQglobal for each group were significantly different from other groups (P < 0.05), with NECR and IQ being higher in high-activity groups than in low-activity groups. The overall IQ was acceptable in all patients, even in the lowest-activity group (1.84 MBq/kg). The mean NECRglobal and IQglobal were significantly different in all 4 body-mass-index groups (P < 0.05), except between groups II and III (P > 0.05). NECRlocal and IQlocal correlated moderately (r = 0.64). Conclusion: Optimization of injected 18F-FDG radioactivity from 7.4 MBq/kg (200 μCi/kg) to 1.85 MBq/kg (50 μCi/kg) resulted in acceptable IQ, despite a reduction in NECR.
The burgeoning demand for PET/CT imaging in providing personalized health care has led to a continuous evolution of technology to provide the best image quality (IQ). This evolution has resulted in incorporation of advances such as time-of-flight and point-spread function in reconstruction algorithms to improve the spatial resolution of the PET images (1–4). PET/CT scanners that include time-of-flight and point-spread function aim to get good IQ even with less radioactivity injected into the patient (5,6). Decreasing the dose of injected activity is always a welcome step to reduce exposure of the patient to radiation. However, despite the use of advanced technology, there is a limit below which the administered radioactivity cannot be reduced without increasing the acquisition time to get good IQ. Therefore, the injected dose and acquisition time need to be balanced to achieve diagnostic PET IQ.
PET IQ assessment is an arduous task because of the physics of PET image acquisition. Not all the counts acquired during a PET acquisition are true coincidence counts; random and scatter counts are also included. These random and scatter counts do not reflect the true activity distribution in the body and, thus, deteriorate the PET IQ. Using signal-to-noise ratio as a quantifying parameter for IQ assessment is not very promising, since it takes into account all the prompt counts, including random and scatter counts. However, noise-equivalent count rate (NECR) is the IQ parameter that quantifies the contribution of true counts in total prompts and thus is more representative of IQ. A higher NECR ensures a better signal-to-noise ratio in the patient data (6,7).
NECR has been used routinely as a parameter for comparing the IQ of PET scanners. Its use as a tool for assessing IQ in clinical PET/CT images has been reported for a few years (6–9). There is limited literature on the value of NECR in relation to activity injected per kilogram of body weight and its relation to IQ. The studies computing NECR as an IQ parameter are mostly phantom or simulation studies (10–12). Two retrospective studies have measured NECR in patient populations, and one of these studies has calculated only the regional NECR of the liver (8–9).
According to European Association of Nuclear Medicine guidelines, activity is administered linearly or quadratically with patient weight and acquisition time (13). Keeping a minimum acquisition time of 1 min, and for a patient weight of 45–75 kg, the 18F-FDG dose ranges from 4.07 to 7.03 MBq/kg (110–190 μCi/kg). Other studies have also recommended doses ranging from 5.55 to 7.4 MBq/kg (150–200 μCi/kg) (9–10,14).
The present study aimed to optimize the injected dose of 18F-FDG to reduce the effective exposure from whole-body PET/CT scans and to assess the effect of this optimization on NECR and visual IQ assessment.
MATERIALS AND METHODS
Patient Population
This prospective study included 112 patients who were referred for 18F-FDG PET/CT imaging from January to December 2019, regardless of indication. The study was approved by the departmental review board, and written informed consent was obtained from all patients. Those with fasting glucose levels higher than 200 mg/dL and those who had not fasted for at least 4 h were not included. Patients for whom partial extravasation of the 18F-FDG activity was seen on the PET/CT images were excluded, as extravasation affects the quantification of IQ. The patients were divided into 4 groups (groups A–D) depending on the amount of 18F-FDG radioactivity injected per kilogram of body weight. In groups A, B, C, and D, the injected dose was 1.85 MBq/kg (50 μCi/kg), 3.7 MBq/kg (100 μCi/kg), 5.5 MBq/kg (150 μCi/kg), and 7.4 MBq/kg (200 μCi/kg), respectively. Further, the study population was divided into 4 groups (groups I–IV) based on body mass index (BMI) for comparison of the effect of BMI on IQ and NECR. Groups I, II, III, and IV had a BMI of 15–20, 20.1–25, 25.1–30, and 30.1–35 kg/m2, respectively.
PET/CT Imaging
All patients underwent whole-body PET/CT from the base of the skull to the mid thigh using a 3-dimensional time-of-flight–based scanner (Discovery MIDR; GE Healthcare) at 45–75 min after administration of the radioactivity. A helical CT scan using a tube voltage of 120 kVp and a variable tube current (150–350 mA) was acquired craniocaudally, followed by a PET scan in the caudocranial direction, at a rate of 90 s per bed position for group A and 60 s for the remaining 3 groups. The whole-body PET images were reconstructed in a matrix of 192 × 192 using ordered-subset expectation maximization (24 subsets, 2 iterations) and a z-axis gaussian filter of 5.5 mm in full width at half maximum. During the PET acquisition, counts (true counts, total prompts, and randoms) were recorded for each bed position.
Image Analysis
PET IQ was assessed using 2 methods: quantitative and qualitative. Quantitative IQ was assessed by measuring NECR for each bed position (NECRlocal). This measurement was done by taking the ratio of the square of true counts to the sum of true counts, randoms, and scatter counts (total prompts). The unit for NECR was kilocounts per second (kcps). The NECR for the whole-body scan of a patient (NECRglobal) was defined as the mean NECRlocal for all bed positions in a whole-body acquisition.
For the clinical and qualitative IQ analysis, the PET/CT images were transferred to a dedicated review workstation (Advantage Workstation 4.7; GE Healthcare). PET maximum-intensity-projection and transaxial IQ was visually assessed and scored by a nuclear medicine physician and a physicist, each having more than 8 y of experience. The IQ local score (IQlocal) was a 5-point scale assigned to each bed position, where 1 is poor, 2 is bad, 3 is acceptable/average, 4 is good, and 5 is excellent. The IQ global score (IQglobal), which used the same 5-point scale, was assigned to the whole study after assessment of all bed positions and maximum-intensity-projection images. The readers assessed PET IQ subjectively on the basis of prevalence of noise, contrast between different tissues and organs, and lesion detectability.
Statistical Analysis
Quantitative parameters with a normal distribution were expressed using mean and SD. The mean NECRglobal and IQglobal were compared in all 4 groups using independent t testing for each pair of groups. The mean NECRglobal and IQglobal were compared in the 4 BMI groups using independent t testing for each pair of groups. The correlation among NECRglobal, IQglobal, and BMI, as well as among NECRlocal, IQlocal, and BMI, was assessed using the Pearson correlation coefficient. The 2-way multivariate analysis was applied to study to see if there was any interaction between the activity group and the BMI group while evaluating NECRglobal and IQglobal. P values were considered significant if they were less than 0.05.
RESULTS
In total, 112 patients were recruited, of whom 3 were excluded because of partial extravasation of radioactivity. Only 109 patients (38 men, 71 women) in the age group (14–80 y) with a mean age of 49.8 ± 16.1 y were included. Descriptive mean values of injected activity, NECRglobal, IQglobal, BMI, and uptake time in groups A (n = 18), B (n = 30), C (n = 32), and D (n = 29) have been tabulated in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org).
Comparison of NECRglobal and IQglobal in Different Activity Groups
NECRglobal and IQglobal showed a statistically significant difference (P < 0.05) among all 4 activity groups, with group D showing highest NECRglobal and IQglobal scores and group A showing the lowest NECRglobal and IQglobal scores. The mean IQglobal score in group A was 3, denoting an overall acceptable IQ, even in the lowest-activity group. No study was reported as having bad or poor IQ in any group.
Correlation of IQ Scores and BMI
The correlation coefficient between NECRglobal and IQglobal was 0.47 (P < 0.05), and the correlation of NECRglobal and IQglobal with BMI was negative, at r = −0.46 and −0.40 (P < 0.05), respectively. NECRlocal and IQlocal were moderately correlated with each other, having a correlation coefficient of r = 0.64 (P < 0.05). No significant correlation was found between NECRlocal and BMI or between IQlocal score and BMI (Fig. 1).
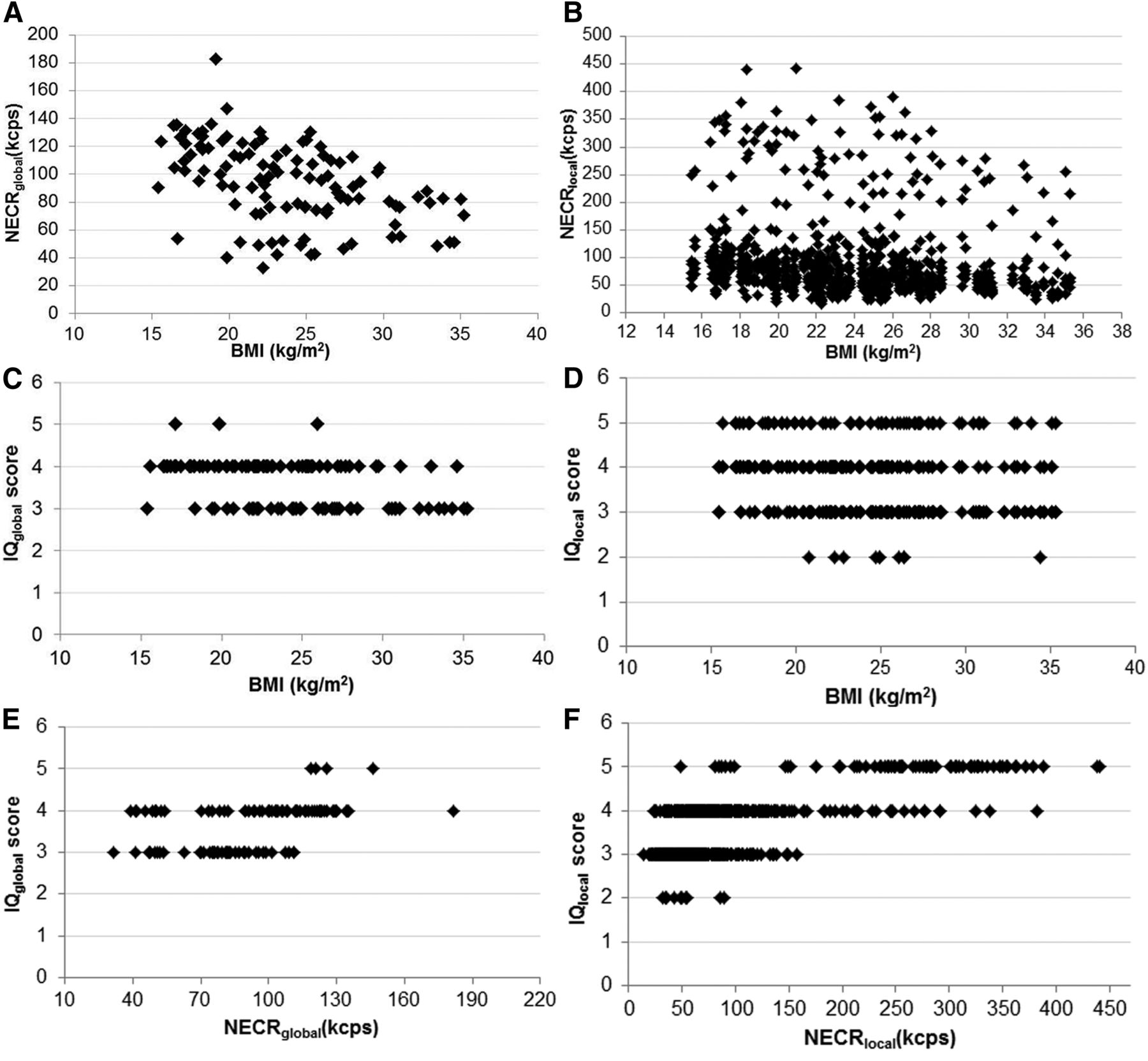
Variation in value of NECRglobal with BMI (A), NECRlocal with BMI (B), IQglobal score with BMI (C), IQlocal score with BMI (D), IQglobal score with NECRglobal (E), and IQlocal score with NECRlocal (F).
Comparison of NECRglobal and IQglobal in Different BMI Groups
The variation in mean NECRglobal and IQglobal for the different BMI groups within each activity group is shown in Supplemental Figure 1. The mean NECRglobal and IQglobal were significantly different in all 4 BMI groups (P < 0.05), except between groups II and III (P > 0.05).
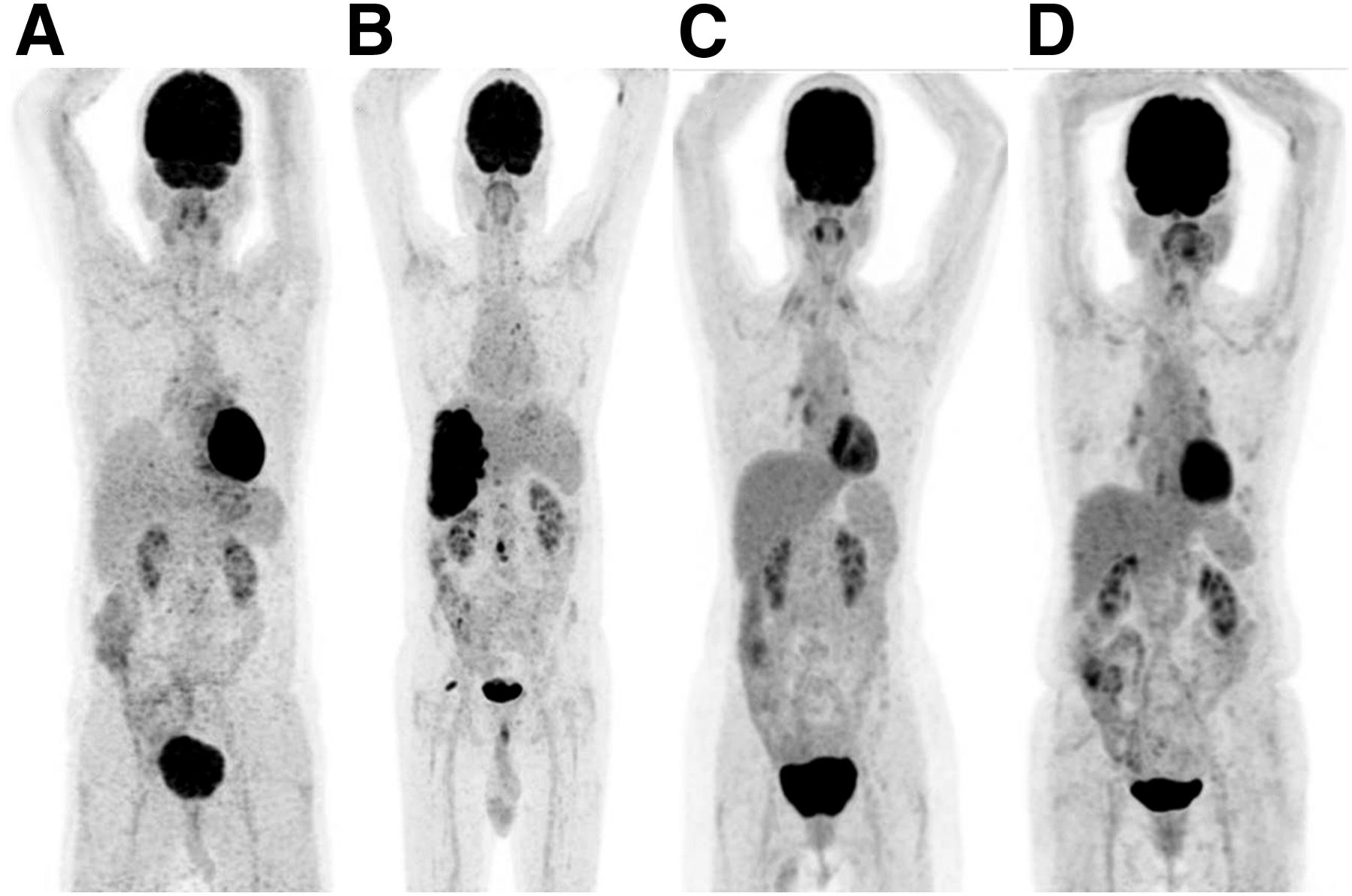
The difference in visual IQ in patients with similar BMIs but injected with different amounts of radioactivity can be seen in Figures 2 and 3.

18F-FDG PET maximum-intensity-projection images of 4 different patients having approximately the same BMI (20.00 kg/m2). (A) Administered activity: 1.85 MBq/kg (50 μCi/kg); NECRglobal, 50.55 kcps; IQglobal score, 3. (B) Administered activity: 3.7 MBq/kg (100 μCi/kg); NECRglobal, 77.78 kcps; IQglobal score, 4. (C) Administered activity: 5.5 MBq/kg (150 μCi/kg); NECRglobal, 90.23 kcps; IQglobal score, 4. (D) Administered activity: 7.4 MBq/kg (200 μCi/kg); NECRglobal, 146.30 kcps; IQglobal score, 5.

18F-FDG PET maximum-intensity-projection images of 4 different patients having approximately the same BMI (25.00 kg/m2). (A) Administered activity, 1.85 MBq/kg (50 μCi/kg); NECRglobal, 48.25 kcps; IQglobal score, 3. (B) Administered activity, 3.7 MBq/kg (100 μCi/kg); NECRglobal, 75.72 kcps; IQglobal score, 3. (C) Administered activity, 5.5 MBq/kg (150 μCi/kg); NECRglobal, 129.54 kcps; IQglobal score, 4. (D) Administered activity, 7.4 MBq/kg (200 μCi/kg); NECRglobal, 122.94 kcps; IQglobal score, 4.
Interaction Effect Between Activity Group and BMI Group on IQ Parameters
The 2-way multivariate analysis showed no statistically significant interaction effect between activity group and BMI group on either NECRglobal or IQglobal (F12,190 = 1.631, P = 0.086; Wilks λ = 0.822).
DISCUSSION
In any type of nuclear medicine procedure, dose optimization is a major concern because it aims to minimize exposure of patients and staff to radiation while preserving IQ. The amount of activity administered to the patient can be reduced according to the as-low-as-reasonably-achievable principle. However, a reduction in administered activity can compromise IQ if the resultant counts are insufficient. An increase in administered activity in PET (beyond a certain level) also degrades IQ, since random counts also increase. Optimization of the administered dose and IQ is essential for 18F-FDG PET/CT studies. The impetus behind the rapid evolution of PET instrumentation and reconstruction algorithms is to minimize the activity injected into patients as much as possible while maintaining diagnostic IQ. Use of improved scintillator crystals such as lutetium-yttrium oxyorthosilicate and incorporation of techniques such as time-of-flight and point-spread function in reconstruction algorithms have made this minimization feasible by improving spatial resolution, increasing image contrast, and decreasing noise in the image.
NECR has been used as a quantitative PET IQ parameter either in phantom studies or in simulation studies (10–12). Only a few studies have used it as an analysis parameter in patient studies. Chang et al. studied the effect of injected dose and BMI on NECR, but they computed NECR for only 1 bed position, with liver (8). Queiroz et al. also assessed clinical IQ and compared it with NECR measurements in a patient population (9). NECR can be used as an objective measure of the IQ of a PET system. A higher NECR is expected to ensure a good signal-to-noise ratio and less noise in the reconstructed images. In the present study, NECR along with visual IQ assessment was used to assess IQ for 18F-FDG PET images acquired using different weight-based doses.
The mean NECRglobal for all patients (n = 109) in our study was 92.57 kcps. This is lower than the mean NECRglobal computed by Queiroz et al. in their study (n = 75, NECR 106.4 kcps) (9). Also, the mean NECRglobal calculated in patients segregated according to BMI was 91.5, 85.25, 88.5, and 63.22 kcps in groups I, II, III, and IV, respectively, in the present study, as compared with 133.04, 112.49, 102.34, and 86.79 kcps, respectively, in their study. The decreased mean value in the present study can be explained by inclusion of an even lower-activity group of 1.85 MBq/kg (50 μCi/kg) in our study. A trend for NECR to increase with decreasing BMI was observed in our study, except for groups II and III, for which there was no statistically significant difference in the mean values. A similar trend was observed in the study by Queiroz et al. The value of NECR calculated in the present study cannot be compared with that computed in the study by Chang et al., as they calculated the NECR for only 1 bed position, liver, whereas we calculated it for each bed position and then averaged the values (8).
Though many studies have compared NECR with visual assessment, no study, to our knowledge, has compared NECR and visual assessment in patient groups injected with different amounts of activity per kilogram of body weight. The quantitative and qualitative IQ analysis in our study showed a significant difference in patient groups injected with different activities. The mean NECRglobal and IQglobal were highest for the group injected with 7.4 MBq/kg (200 μCi/kg) and lowest for the group injected with 1.85 MBq/kg (50 μCi/kg), as shown in Supplemental Table 1. However, in a similar study, Chang et al. compared the local NECR for liver and found no statistically significant change when the injected activity was increased from 296–444 MBq (8–12 mCi) to 555–740 MBq (15–20 mCi) (8). The difference in findings between the 2 studies can be explained by use of a higher range of activities in their study than in ours (89.91–463.24 MBq [2.43–12.52 mCi]).
Queiroz et al. showed that patient NECR and the respective IQ correlated strongly with each other and negatively with BMI (9). They also found a significant positive correlation between IQlocal and NECRlocal. A similar moderately significant correlation between IQlocal and NECRlocal was observed in the present study. NECRglobal also correlated with IQglobal, and both these parameters had a negative correlation with BMI; however, the correlation was weak. One possible explanation can be use of a discrete score in our study, unlike the continuous score used by Queiroz et al. (9).
Several studies have been done to optimize 18F-FDG activity in order to achieve good IQ. In a study by Geismar et al., the authors concluded that an optimal 18F-FDG dose of 4 MBq/kg can be used only in patients with a BMI of 22 kg/m2 or less; a dose of 5 MBq/kg was needed to obtain good IQ in patients with a BMI of more than 22 kg/m2 (15). A similar study by Everaert et al. determined an 18F-FDG activity of at least 8 MBq/kg (200 μCi/kg) to be an optimized dose, at 2–3 min per bed position, for obtaining good IQ for lutetium oxyorthosilicate PET/CT scanners (14). However, in the present study, in the group with the second lowest activity—that is, 3.7 MBq/kg—as well as for the highest-BMI patient (35.28 kg/m2), and with an acquisition time of 1 min per bed position, diagnostic IQ was maintained. A comparable optimized dose of 3.8 MBq/kg has been given by Queiroz et al., but their study was retrospective and not supported by any patient images (9). The feasibility of reducing the injected activity to 1.85 MBq/kg (50 μCi/kg) was investigated in a group of 18 patients by increasing the acquisition time from 60 s to 90 s per bed position. Though the NECR was comparatively reduced, acceptable diagnostic IQ could be achieved in this group as well, even for patients having a BMI of as high as 34.64 kg/m2.
For all 109 patients in the present study, with an administered activity from 1.85 to 7.4 MBq/kg body in different groups, the IQ score was at least 3. This implies that the IQ was acceptable to excellent in patients with different BMIs. An 18F-FDG activity of at least 1.85 MBq/kg was considered optimal for obtaining acceptable IQ in patients undergoing whole-body 18F-FDG PET/CT using an imaging time of 60–90 s per bed position, depending on the administered activity. In the future, PET scanners with even faster crystals, coupled with silicon-based photomultiplier tubes aiming to enhance system sensitivity and spatial resolution, can pave the way for use of an even lower administered radioactivity.
CONCLUSION
Optimization of the injected 18F-FDG radioactivity from 7.4 MBq/kg (200 μCi/kg) to 1.85 MBq/kg (50 μCi/kg) resulted in excellent to acceptable IQ in all patients. Administration of a low radiotracer activity (1.85 MBq/kg) can achieve an acceptable PET IQ while reducing exposure of patients to radiation.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Sep. 4, 2020.
REFERENCES
- Received for publication May 26, 2020.
- Accepted for publication July 22, 2020.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.