


Abstract
Gadolinium is toxic and to avoid its deposition in tissues, it must be chemically bonded with nonmetal ions to facilitate its excretion by the kidneys. High signal intensity in the dentate nucleus (DN) and globus pallidus (GP) on unenhanced T1-weighted MR images has been both morphologically and pathologically linked to gadolinium-based contrast agent (GBCA) retention in the brain. The purpose of this study was to determine whether repeated administrations of GBCA would affect the uptake of 18F-FDG in the DN and GP on PET/CT. Methods: Three hundred seventy-six patients who underwent both contrast-enhanced MR (CE MR) of the brain and PET/CT from January 2004 to October 2015 were identified. Patients with a history of brain irradiation or hepatic or renal disease were excluded. The SUVmax was measured in the DN and GP on the PET/CT scan in patients who had 3–6 successive CE MR brain studies. The SUVmax of the corresponding areas in the control group of patients who had not undergone previous CE MR and who had a normal, unenhanced MR finding of the brain was also measured. A Wilcoxon 2-sample test was used for statistical analysis. Results: Fifteen of 376 (4%) patients (mean age ± SD, 54 ± 18 y; 10 men and 5 women) were included in the subject group, and 15 patients (mean age ± SD, 36 ± 9 y; 11 men and 4 women) were included in the control group. The median DN SUVmax was significantly lower in the subject group than in the control group (5.4 vs. 6.4, respectively; P = 0.021). Similarly, the median GP SUVmax was significantly lower in the subject group than in the control group (8.8 vs. 12.1, respectively; P = 0.003). Conclusion: The median SUVmax in the DN and GP was 16% and 27% lower, respectively, in patients who received GBCAs than in those who had not received GBCAs, possibly related to gadolinium deposition in these areas.
MRI uses nonionizing electromagnetic radiation to diagnose and monitor disease. A major component of MRI is the use of gadolinium-based contrast agents (GBCAs). It is estimated that more than 200 million doses of GBCAs have been administered worldwide (1). Gadolinium is a toxic element and to avoid its deposition in tissues, it is chemically bonded with nonmetal ions to create GBCAs in an effort to facilitate its excretion by the kidneys (2). GBCAs are used at relatively low concentrations (0.1–0.3 mmol/kg), with serious adverse reactions only occurring in about 0.03% of administrations, usually in patients with compromised renal function. One of the more serious complications associated with GBCAs is nephrogenic systemic fibrosis, a potentially life-threatening complication resulting in widespread tissue fibrosis. Nephrogenic systemic fibrosis is widely attributed to gadolinium ions dissociating from their chelating agents and depositing in tissues (3). It has been believed that gadolinium agents were completely expelled from the body in patients with normal renal function; however, recent studies have shown that high signal intensity in the dentate nucleus (DN) and globus pallidus (GP) on unenhanced T1-weighted MR images have been linked to gadolinium retention in the brain (4). Originally it was thought that damage to the blood–brain barrier, renal dysfunction, liver disease, or metabolic disorders were the cause of contrast deposition in the brain; however, recent studies have shown that gadolinium deposits in the brain of patients who have normal renal function and intact blood–brain barriers after multiple contrast administrations (2).
PET coupled with CT is a radiologic modality that uses the administration of radiopharmaceuticals to diagnose and monitor physiologic pathologies. 18F-FDG is a radioactive glucose analog that is commonly used in PET procedures to analyze the metabolic activity of tissue in the body. There are few studies showing a relationship between gadolinium deposition in the brain and the health of the surrounding tissue. The use of PET/CT allows for a comparison of the anatomic regions of gadolinium deposition with the metabolic activity of the same region. Given that intact GBCAs do not cross intact blood–brain barriers of healthy patients, it is not clear whether gadolinium deposition may result in metabolic changes in the brain. The purpose of this pilot study was to determine whether repeated administration of GBCAs affects the uptake of 18F-FDG in the DN and GP on PET/CT.
MATERIALS AND METHODS
All patients’ records included in this study were obtained from our institution. The Saint Louis University Hospital Institutional Review Board approved this retrospective study, and the requirement to obtain informed consent was waived. All data were handled in compliance with the Health Insurance Portability and Accountability Act of 1996.
MRI
Patients who underwent at least 1 contrast-enhanced MR (CE MR) and 1 PET/CT from January 2004 to October 2015 were identified. Patients who underwent 3–6 CE MR (of which at least 2 were brain studies) scans were then selected for the subject pool. The first CE MR of the brain was used to establish a baseline and the last CE MR of the brain was used for comparison. The brain MR images were acquired according to the institution’s protocol. The images were obtained on either a 1.5-T Siemens MAGNETOM Aera or a 3-T Philips Achieva. The brand of GBCA administered was not a factor in patient selection or exclusion. Patients with a history of brain irradiation or hepatic or renal disease were excluded from the study because these conditions can affect gadolinium deposition. Patients with known brain tumors or lesions were also excluded. The control group consisted of patients who had never undergone a CE MR and had a normal unenhanced MR finding of the brain.
PET/CT
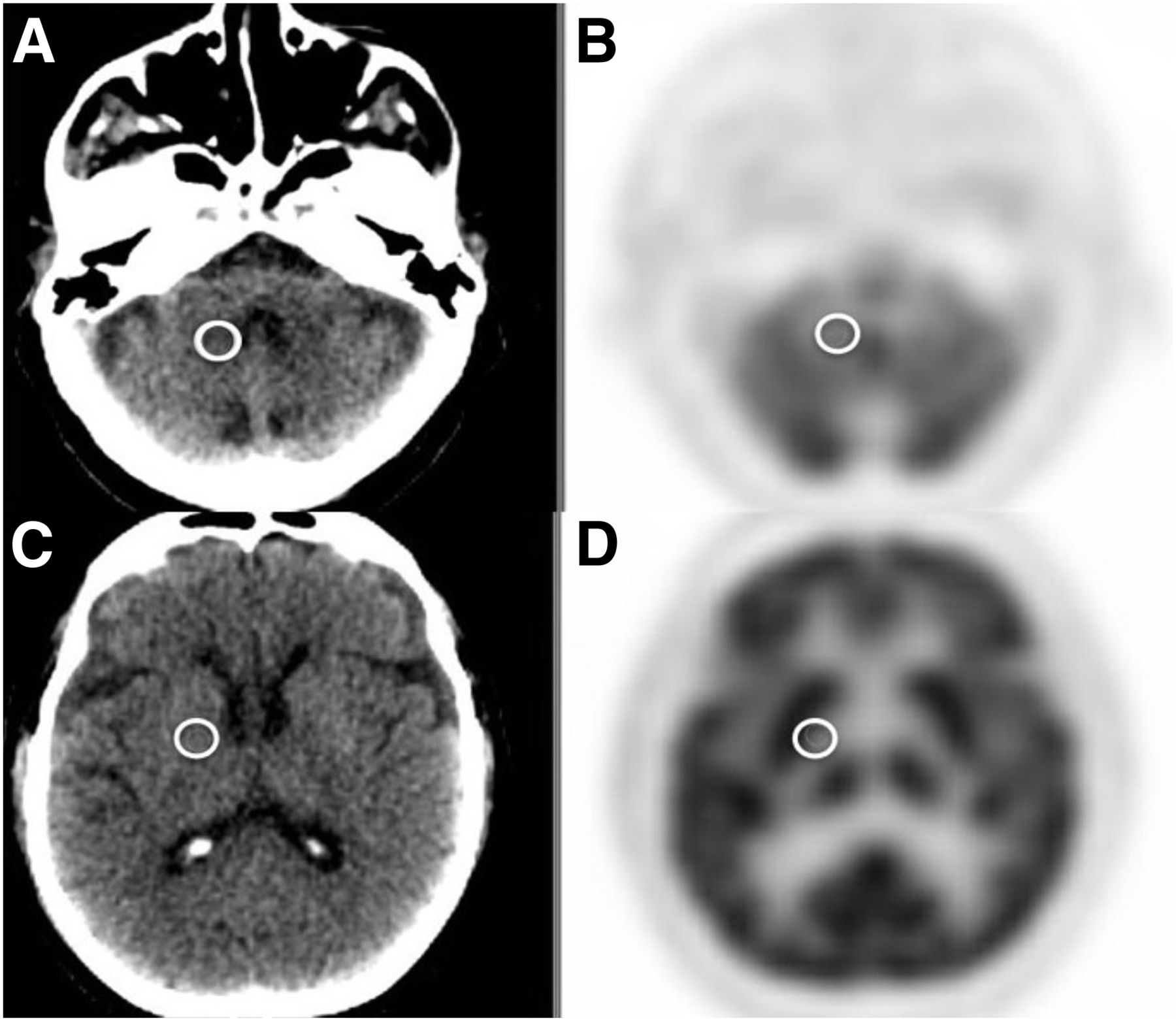
For the patient to qualify for the study, the PET/CT used for analysis had to be completed after the last CE MR used for analysis. After the administration of 18F-FDG, the PET/CT study was performed on a Philips Gemini Time of Flight system. Images for patients in the subject group were acquired using the institution’s protocol for whole-body acquisitions, whereas images for those in the control group were acquired as part of a dedicated brain acquisition. 18F-FDG doses were calculated on the basis of weight at 5.18 MBq/kg (0.14 mCi/kg), with a maximum dose of 555 MBq (15 mCi), and administered intravenously using a butterfly needle; imaging was performed after an uptake time of 60 min. A fasting blood glucose level of less than 150 mg/dL was required before injection. Regions of interest (ROIs) were drawn on the PET images around the DN and GP for each patient, and the SUVmax was recorded. ROIs were first drawn by a certified nuclear medicine technologist from the research team and then verified by a board-certified nuclear medicine physician who also holds certification as a neuroradiologist (fellowship-trained). The CT portion of the PET/CT was used to locate the anatomic regions in the brain (Fig. 1).
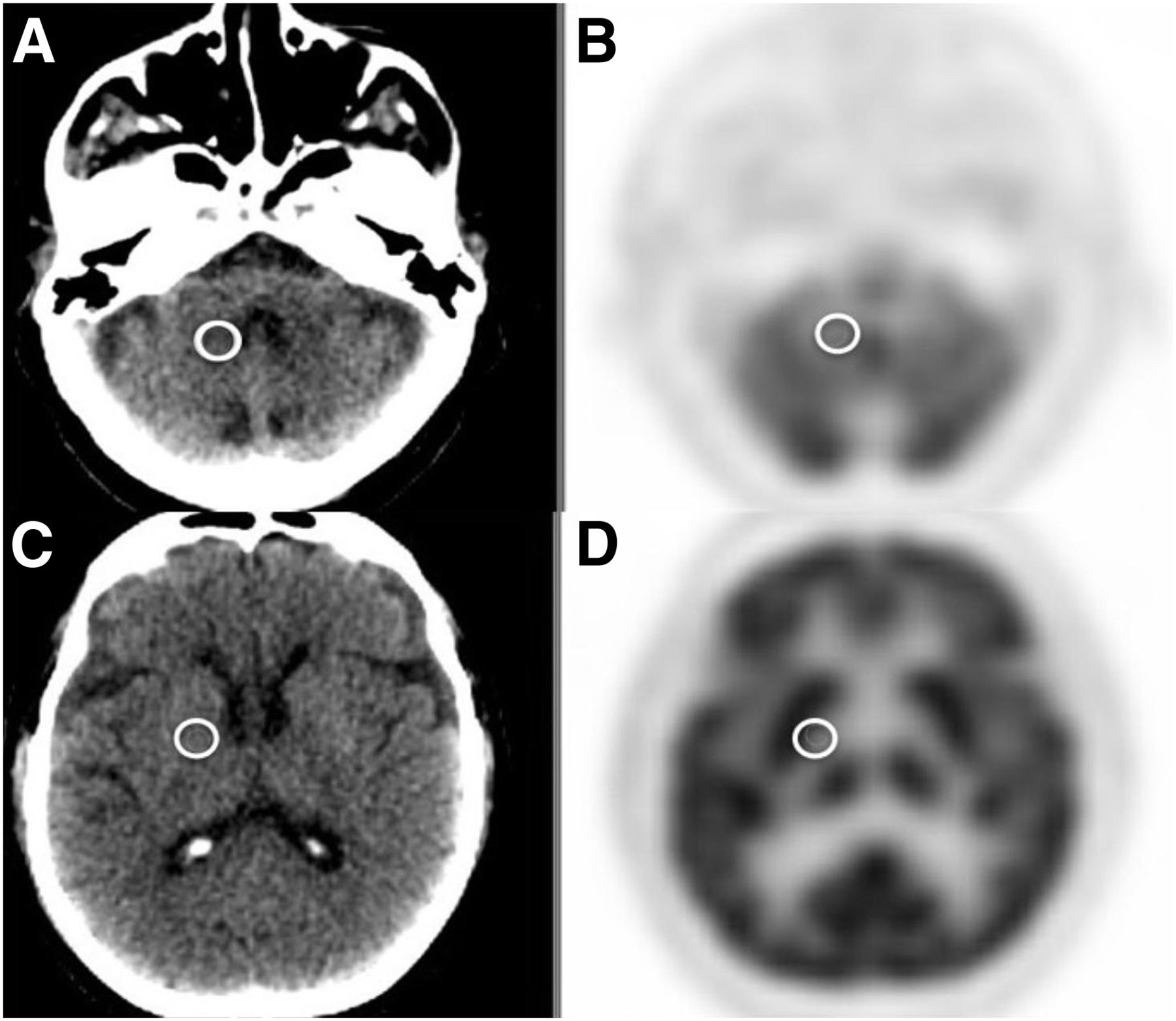
CT (A and C) and PET (B and D) images of 84-y-old man with history of scalp melanoma. White circles represent ROI analyses drawn around DN (A and B) and GP (C and D).
Data Analysis
Because of the small sample size in the subject and control groups, and an assumption of a nonnormal distribution of data, the Wilcoxon 2-sample nonparametric test was chosen to compare the median SUVmax from the DN and GP between each group. All statistical analyses were conducted using the Statistical Analysis System (SAS) software (version 9.4; SAS).
RESULTS
Three hundred seventy-six patients who underwent both a CE MR and a PET/CT scan from January 2004 to October 2015 were identified. Fifteen of 376 (4%) patients (mean age ± SD, 54 ± 18 y; 10 men and 5 women) were included in the subject group, and 15 patients (mean age ± SD, 36 ± 9 y; 11 men and 4 women) were included in the control group.
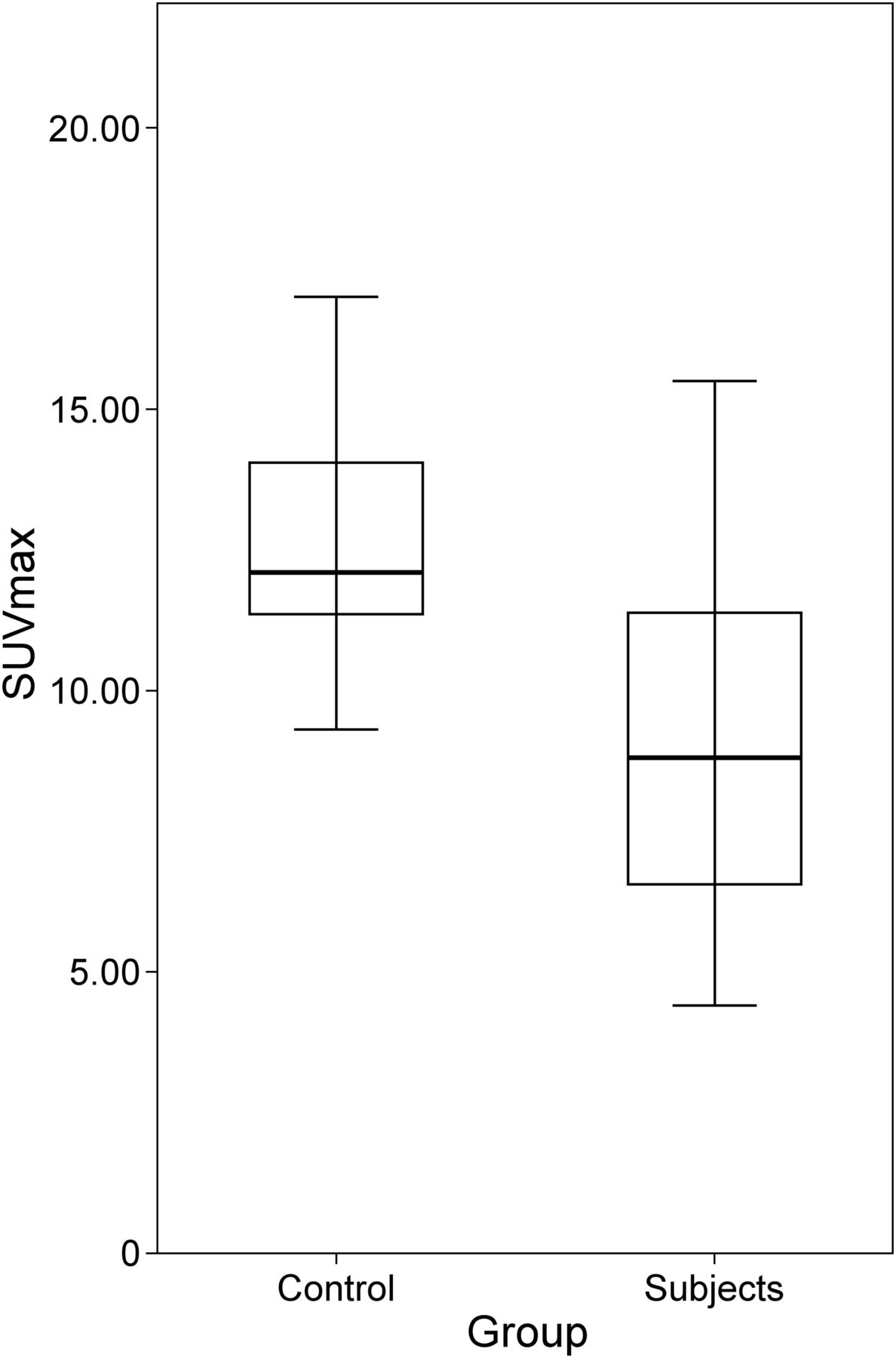
The results of the Wilcoxon 2-sample test indicate that the median DN SUVmax was significantly lower in the subject group than in the control group (5.4 vs. 6.4, respectively; z = 2.035, 1-tailed P = 0.021). Similarly, the median GP SUVmax was significantly lower in the subject group than in the control group (8.8 vs. 12.1, respectively; z = 2.717, P = 0.003). Additional analysis was performed to investigate an interaction effect from age or sex, but no significant interaction effect was found. A summary of the findings is presented in Table 1, and group median comparisons are presented in Figures 2 and 3.
Comparison of 25th Percentile, Median, 75th Percentile, and 1-Tailed P Values from DN and GP for Control and Subject Groups

Box plot of SUVmax in DN for controls and subjects. Median difference between groups is significant (P = 0.021).

Box plot of SUVmax in GP for controls and subjects. Median difference between groups is significant (P = 0.003).
DISCUSSION
GBCAs are a crucial element in diagnosing disease in MRI. Other studies have proven that gadolinium is dissociating from GBCAs and depositing in the DN and GP. Our study intended to evaluate the potential impact of gadolinium deposits on brain metabolic activity as detected by 18F-FDG PET/CT. Because 18F-FDG uptake corresponds to the metabolism of tissue, decreased uptake could imply decreased metabolism.
The DN and GP are separate regions of the motor cortices of the brain. The DN is part of the deep cerebellar nucleus and is the located most laterally. The lateral hemispheres of the cerebellar cortex are connected to the cerebellum through the DN. The DN also has a connection through the superior peduncle to the ventral lateral nucleus of the thalamus, which relays to the cerebral motor cortex (5). If the DN is exhibiting reduced 18F-FDG uptake, the deposited gadolinium could be reducing the function of the cells in the DN. This could lead to reduced cerebral motor output, because the DN connects regions of motor function in the brain. The GP is part of the basal ganglia and is included in the extrapyramidal system. The extrapyramidal system is considered part of the motor system and is thought to affect muscle tone, posture, and voluntary movement (6). If the GP exhibits decreased 18F-FDG uptake as a result of gadolinium deposition, this could lead to decreased control of muscle tone and voluntary movement. Compared with our control group, our subject group showed decreases in metabolic activity (as measured by SUVmax) of 16% and 27% in the DN and GP, respectively.
When comparing 18F-FDG uptake in the DN and GP between subject and control groups, we measured and reported SUVmax rather than SUVmean. Previous research has indicated that SUVmax is becoming the more commonly reported measurement of radiopharmaceutical uptake on PET studies (7) because of the significant reproducibility of the SUVmax measurement and negligible effect that small spatial shifts in ROI placement have on the maximum value within the ROI.
Our study is not without limitations. First, this study has a limited sample size. Although we started with over 350 patients, we were able to use only 15 patients for our subject group because of our extensive exclusionary criteria. To eliminate as many extraneous factors as possible, our patients had to be free of renal disease, liver disease, brain lesions or tumors, and brain irradiation. They also had to have multiple GBCA administrations and brain MR acquisitions and undergo an 18F-FDG PET/CT after their CE MR studies. Second, a limitation of the control group is that the patients were not age-matched to the subject group. The mean age of the subject group (54 ± 18 y) was higher than the mean age of the control group (36 ± 9 y). Future studies would have subjects in both groups be sex- and age-matched to control for these variables. As for other differences between the patient groups, the control group patients had no history of cancer whereas the subject group consisted of some patients who had cancer and some who did not; however, those patients who had brain tumors or lesions were excluded from the subject group in an attempt to control for that factor.
Third, the PET/CT acquisition protocol differed between groups. The subject group underwent whole-body PET/CT per the standard protocol at our institution. The control group underwent dedicated brain PET/CT per another research protocol. As a result, the PET scan time per bed position for the brain differed between groups. A final limitation of this study is that we could only qualitatively state that our subjects had gadolinium deposition in the DN and GP, using evidence stated by peer-reviewed research that gadolinium has been shown to deposit in these regions of the brain. In future studies, the amount of gadolinium deposition could be quantitatively measured.
Although our study suggests that gadolinium may cross intact blood–brain barriers and affect 18F-FDG uptake in the DN and GP, our study does not evaluate or limit itself to a specific type (linear, macrocyclic, ionic, and nonionic) or brand of contrast. All of our patients received multiple types and brands of GBCA for their examinations. Further studies need to be done to explore the types and brands of GBCAs individually to determine varying rates of gadolinium deposition. In an ideal setting, a useful approach would be to use the same patient for the control and subject group. The subject would undergo 18F-FDG PET/CT before any GBCA administration, followed by a series of brain MR studies and GBCA administrations, and finally another 18F-FDG PET/CT scan at the end. In this approach, the patient could serve as his or her own baseline, and we could better track progression of gadolinium deposition and its effects on brain metabolism.
CONCLUSION
The median SUVmax in the DN and GP was 16% and 27% lower, respectively, in patients who received GBCAs than in patients who did not receive GBCAs. This could be related to gadolinium deposition in these areas. Future research should focus on prospectively validating these results using appropriate age- and sex-matched controls.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 10, 2016.
REFERENCES
- Received for publication July 11, 2016.
- Accepted for publication October 31, 2016.





{kind=link}
{kind=link}
{kind=link}