


Abstract
The human epidermal growth factor 2 (HER2)–overexpressing (HER2-positive [HER2+]) gastric (GC) and gastroesophageal junction adenocarcinomas (GEJC) are felt to represent a more aggressive form of disease, which may correlate to increased metabolic activity. Whether tumor SUVmax measured by 18F-FDG PET/CT could be a preoperative parameter used to predict HER2 status of GC/GEJC is unknown. Methods: Pathology reports of HER2+ GC/GEJC biopsies and resections from 31 patients were reviewed and compared with HER2-negative (HER2−) cases distributed evenly over the same time period. We analyzed their SUVmax intensity and then compared the HER2 status and SUVmax parameters and their association with survival. Results: After matching for age and sex, there was no difference in SUVmax between HER2+ and HER2− cases (9.7 and 8.4, respectively; P = 0.6). No difference was seen between HER2+ and HER2− cases in tumor histology (81% and 57% intestinal type, respectively; P = 0.11), size (2.6 and 3.8 cm, respectively; P = 0.12), differentiation (47% and 68% poorly differentiated, respectively; P = 0.06), or presence of lymph node metastasis (60% and 40%, respectively; P = 0.3). Although there was no difference in survival demonstrated by HER2+ and HER2− cases, there was a significant difference in survival between SUVmax above (12.2 mo) and below (30 mo) the median SUVmax (6.6, P = 0.01). Conclusion: Our study shows that SUVmax is not associated with HER2 status of GC/GEJC. Independent of HER2 overexpression, patients with a high SUVmax demonstrate a worse overall survival, suggesting that metabolic signature is a better predictor of biologic tumor aggressiveness than its histologic signature.
Gastric cancer represents the fifth most common carcinoma worldwide and is also highly prevalent in the United States (1,2). It often presents at an advanced stage, and appropriate diagnosis and treatment decisions follow a time-sensitive course. Human epidermal growth factor-2 (HER2, also known as ERB2) is a tyrosine kinase member of the epidermal growth factor receptor family, known for its key role in driving oncogenesis in numerous human cancers including breast and gastric carcinoma (1–3). One intervention that has shown to increase progression-free and overall survival in patients with HER2-overexpressing (HER-positive [HER2+]) gastric and gastroesophageal junction carcinoma (GC/GEJC) is the addition of trastuzumab to a standard adjuvant chemotherapy protocol (3). Addition of targeted anti-HER2 therapy using this recombinant monoclonal antibody to standard chemotherapy has become the standard of treatment in advanced HER2+ GC/GEJC (4). For these reasons, established clinical recommendations include a turnaround time for HER2 assessment studies (immunohistochemistry and fluorescence in situ hybridization) of no longer than 5 d (5). Adjunct biomarkers of GC/GEJC that could lead to earlier diagnosis, prognosis, and personalization of therapy could potentially decrease mortality.
Pretreatment 18F-FDG PET/CT studies are used for staging purposes for several human cancers. This list includes carcinomas of breast, colon, esophagus, head and neck, and lung as well as lymphomas and melanoma (6). The amount of 18F-FDG uptake reflects a tissue’s level of metabolic activity, reported semiquantitatively as the SUVmax. The SUVmax level (or metabolic signature) correlates with the metabolic activity of the particular tissue or target lesion. Several authors have suggested that HER2+ GC/GEJCs represent a more aggressive form of disease and portend a worse prognosis (7–9). However, HER2+ status in GC/GEJC has not yet been correlated with this metabolic signature.
The objective of this study was to assess the predictive role of SUVmax for HER2 expression in cases of GC/GEJC. In addition, we compared the ability of cancer SUVmax and HER2 status to predict mortality. In doing so, we tested the comparative abilities of imaging and pathology in assessing tumor aggressiveness in a cohort of GC/GEJC patients.
MATERIALS AND METHODS
The institutional review board (or equivalent) approved this retrospective study, and the requirement to obtain informed consent was waived. A retrospective search of our pathology database over a 4-y period (2011–2015) revealed 31 total HER2+ GC and GEJC cases, all confirmed by fluorescence in situ hybridization. HER2 testing was performed either on a biopsy or on the corresponding resection for each patient.
We identified 65 random cases of HER2-negative (HER2−)GC/GEJCs distributed evenly over the same time period. As per institutional protocol and recommended practice (5), these cases tested negative by immunohistochemistry and were never tested by fluorescence in situ hybridization.
Patient baseline clinical characteristics including age and sex were recorded. The outcomes of interest were disease-related mortality and time to death (mo).
Pathologic Criteria
All GC and GEJC diagnoses were rendered by specialty-trained gastrointestinal pathologists. The following pathologic parameters, when available, were collected from the surgical pathology report of cases that underwent resections: tumor size (from resected tumors with gross anatomic descriptions), histologic diagnosis, tumor differentiation, and presence of lymph node metastasis. There was not information available for some of these variables because a subset of cases tested for HER2 were biopsies (28 total HER2+ and 41 total HER−), and the corresponding resections either had not been performed or had been performed at an outside institution.
All cases were re-reviewed to confirm the presence of carcinoma and HER2 status by immunohistochemistry. HER2 immunohistochemistry was performed using the HercepTest A0485 (Dako) antibody. HER2 immunohistochemistry stain scoring was interpreted in accordance with the parameters used in the Trastuzumab for Gastric (TOGA) clinical trial (3) and proposed by Hoffman et al. (10). Using the criteria postulated by the TOGA trial, we characterized HER2+ cases as 3+ staining by immunohistochemistry or 2+ staining by immunohistochemistry with a concomitant positive fluorescence in situ hybridization with a HER2–to–chromosome 17 ratio of 2.2 or more.
Radiologic Criteria
PET/CT imaging was performed after the diagnosis of carcinoma was established by pathology and for the purpose of pretreatment staging. All PET/CT studies were performed on the latest generation of scanners, 2 Discovery PET/CT machines (Discovery DST-E and the Discovery D690 PET/CT [GE Healthcare]). Both have similar lutetium-yttrium oxyorthosilicate crystals and reconstruction protocols. A standard oncologic PET imaging using a 3-dimensional acquisition protocol was performed with administered 18F-FDG doses of approximately 555 MBq (15 mCi) and an approximately 60-min but no later than 90-min postinjection delay. No intravenous contrast was administered. Blood sugars were measured in all patients, and scans were rescheduled per protocol if blood sugar was greater than 150. All SUVmax measurements were recalculated from clinical scans by an experienced nuclear medicine physician using a similar technique. Regions of interest were drawn over target lesions using an automated image segmentation threshold Advantage Workstation technique (GE Healthcare). This is a Food and Drug Administration–approved and routinely clinically used technique.
Data Analysis
Continuous variables were expressed as a mean and SD. Comparison of means was performed using the Student t test. Proportions were compared using the Fisher exact test. Kaplan–Meier analysis was performed using the survival data to compare patients with differential HER2 expression. The SUVmax median value was calculated, and SUVmax below and above the median value were used for its relationship to mortality. Data analysis was performed using the STATA statistical software program (StataCorp. 2015. Stata Statistical Software: Release 14; StataCorp LP.).
RESULTS
The clinical characteristics of the 96 patients in the study are summarized in Table 1. There was no difference in patient’s age (70 and 67 y, respectively; P = 0.23) or sex (77% and 69% men, respectively; P = 0.61) between HER2+ and HER2− GC/GEJC cases.
Clinical Characteristics
The mean SUVmax (±SD) of HER2+ cancers (9.7 ± 6.3) was similar to that of HER2− cases (8.4 ± 5.4) (P = 0.6) as shown in Figure 1. There was also no difference in tumor size among cases with differential HER2+ expression (2.6 and 3.8 cm, respectively; P = 0.06).
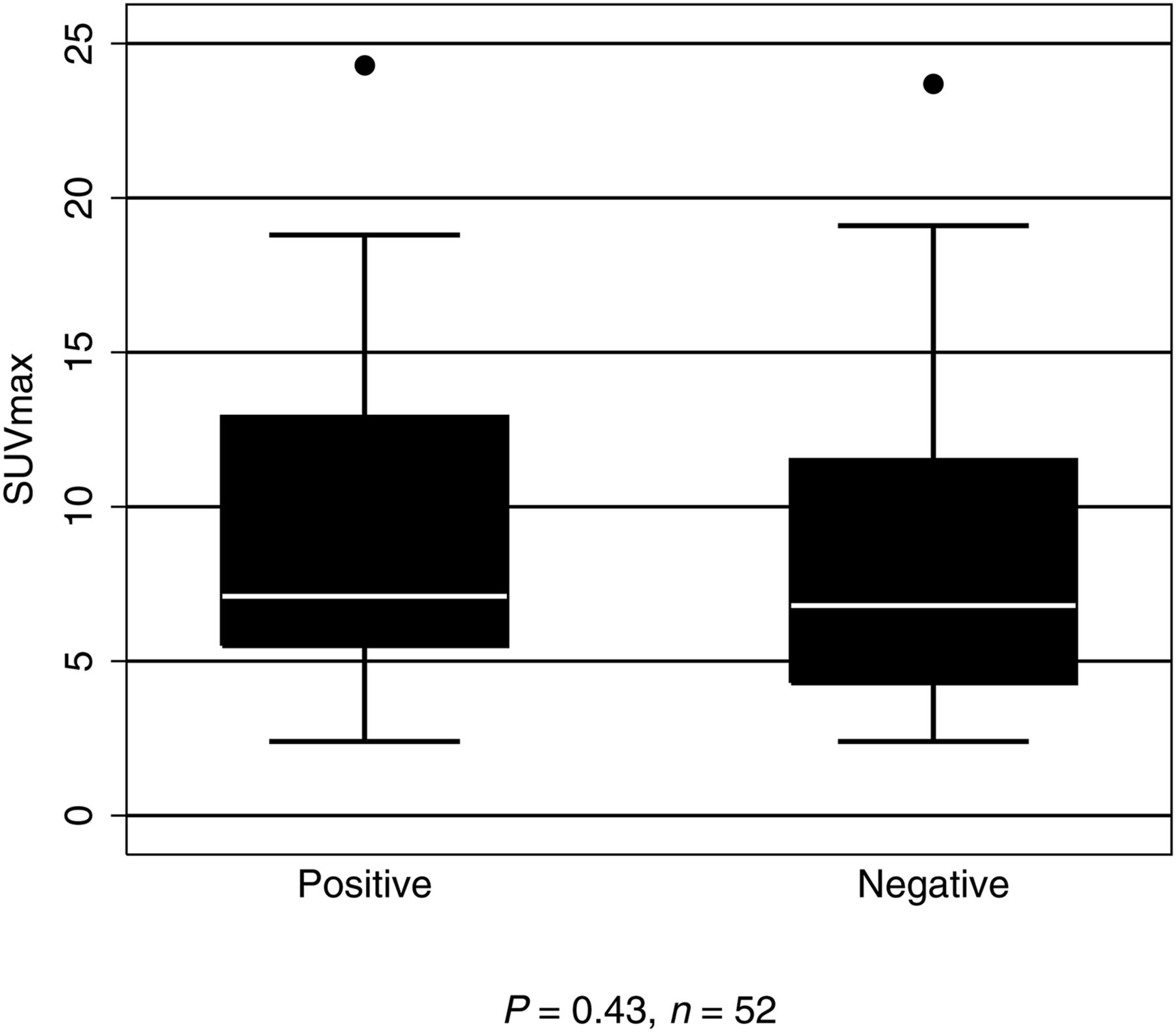
SUVmax, by HER2 status.
No difference was seen between HER2+ and HER2− cases with regards to tumor histology (81% and 57% intestinal type, respectively; P = 0.11), tumor differentiation (47% and 68% poorly differentiated, respectively; P = 0.06), or presence of lymph node metastases (60% and 40% with metastases, respectively; P = 0.23). The pathologic characteristics of the cases studied are summarized in Table 2.
Tumor Pathologic Characteristics
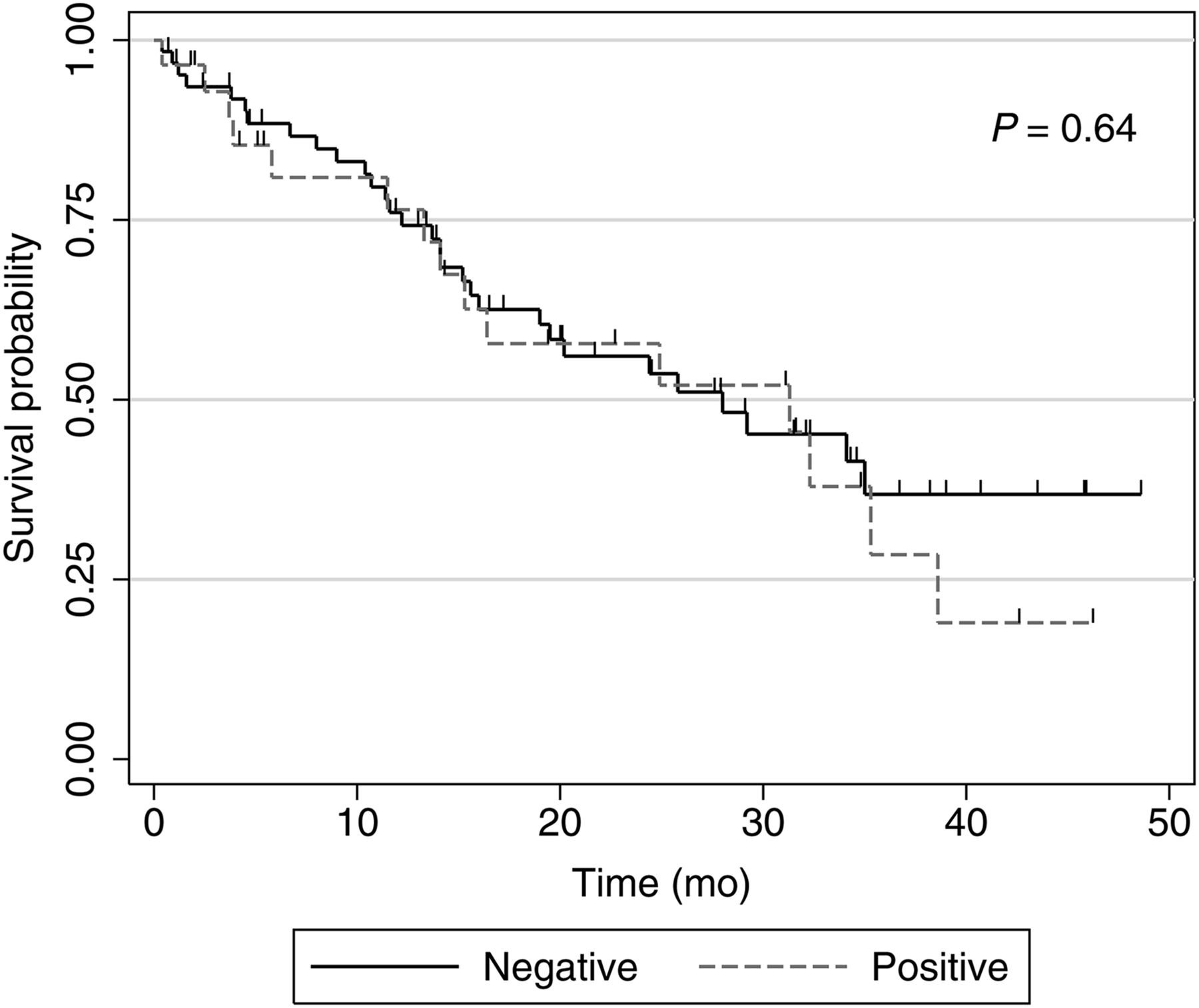
The Kaplan–Meier analysis did not show any survival difference between patients with HER2+ and HER2− cancers (P = 0.64, Fig. 2).

Overall survival, by HER2 status.
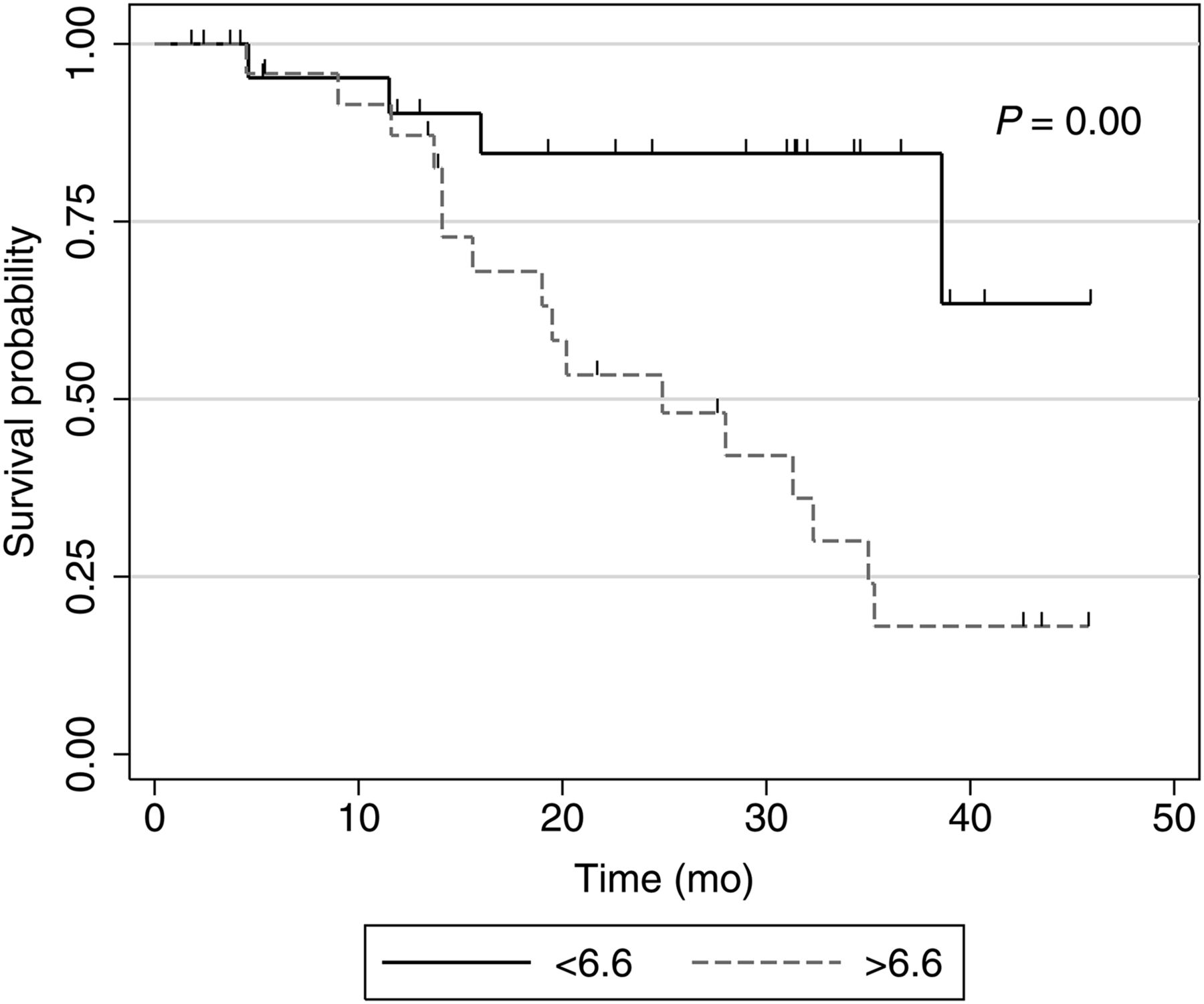
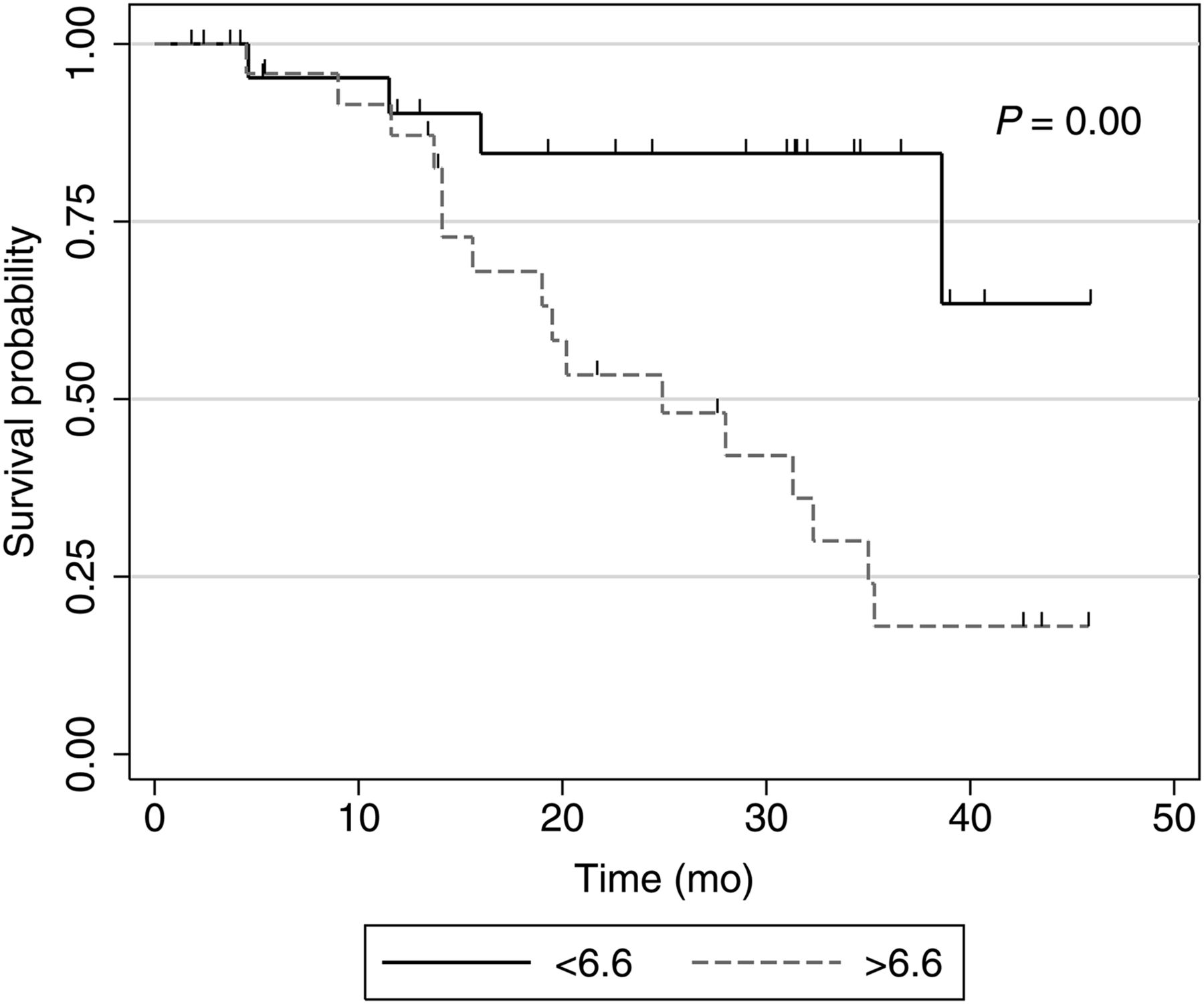
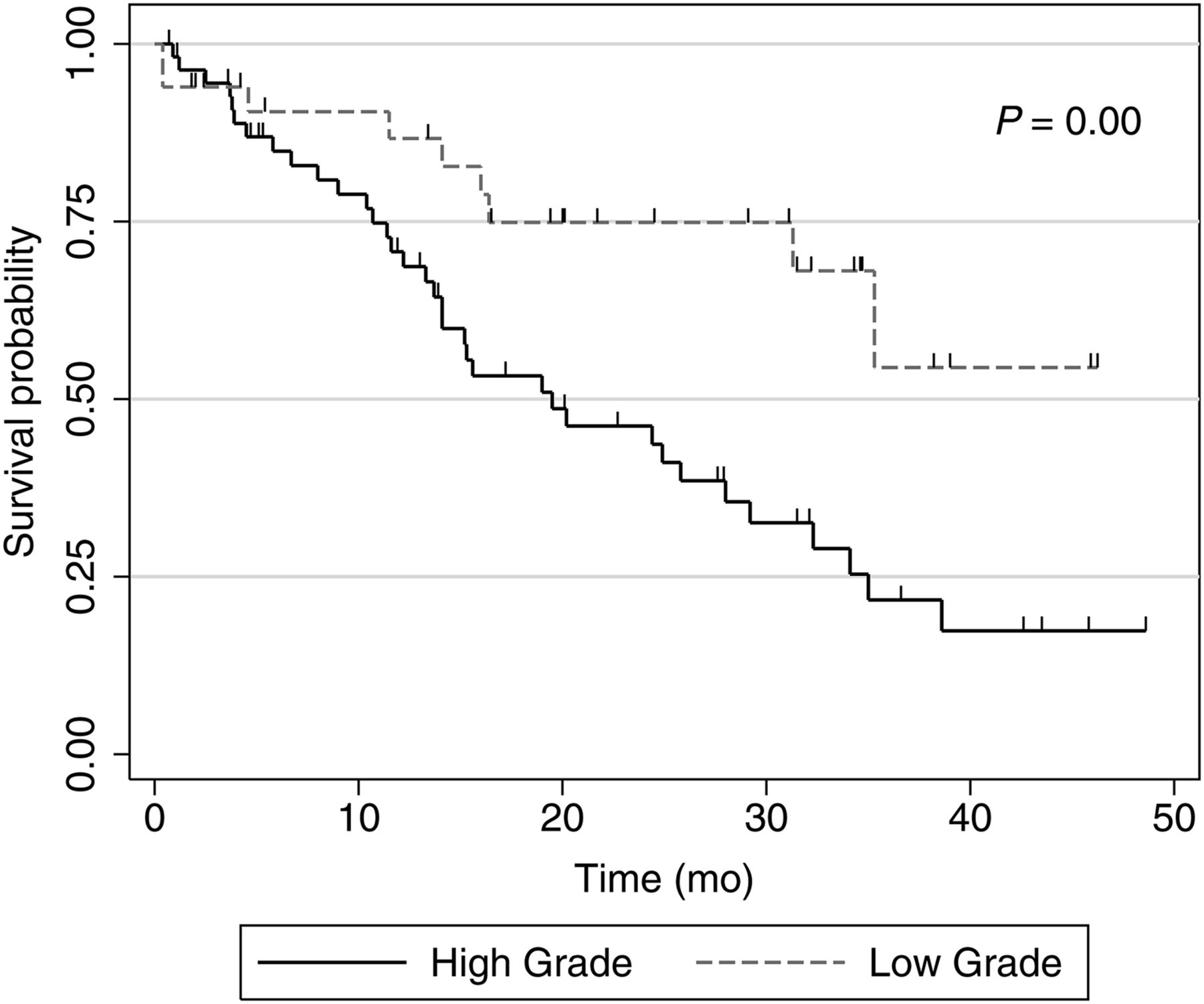
However, there was a statistically significant difference in overall survival between the patients with high tumor metabolic signatures (SUVmax above the median of 6.6) compared with those with metabolic signatures lower than the median SUVmax. The cumulative incidence of death for tumors with high metabolic signatures was 60% compared with 18% in patients with low metabolic signature (P = 0.00), during the study period (Fig. 3). The mean SUVmax of patients who survived during the study period was 7.6 (±5.4) mo versus 10.0 (±4.2) mo among patients who died. Additionally, Kaplan–Meier analysis demonstrated a significant association of survival with tumor differentiation, with poorly differentiated tumors more likely to be associated with death (61% cumulative death incidence vs. 28% in moderately differentiated, P = 0.02, Fig. 4). This was also statistically significant when the tumors were grouped into high-grade tumors (poorly differentiated and anaplastic tumors) and low-grade tumors (moderately and well-differentiated tumors). Patients with high-grade tumors showing an SUVmax above 6.6 had a mean survival of 19.0 mo, whereas those with low-grade tumors and SUVmax below 6.6 had a mean survival of 26.9 mo (sample too small to establish statistical significance). Tumor differentiation and SUVmax were found not to be independent predictors of survival by multivariate analysis. Two tumors in the cohort were well differentiated, and their mean SUVmax was 2.4 (neither was above 6.6).
Overall survival, by SUVmax (above and below median SUVmax of 6.6).

Overall survival, by tumor differentiation.
DISCUSSION
At present, treatment decisions for GC/GEJC follow pathologic assessment of the tissue specimen. In an era of expanding use of efficient noninvasive diagnostic methods, an imaging biomarker used to predict HER2 overexpression in tumors would be a welcome tool, particularly if it could contribute toward treatment decisions. This is of particular importance because trastuzumab is increasingly being used in a neoadjuvant role for HER2+ GC/GEJC based on the level of HER2 expression (11,12). The criteria for HER2 positivity require only a small proportion of cells (10% in resections, and only 5 clustered cells in biopsies) to be positive, and heterogeneity of HER2 expression is well recognized, which can lead to false-negative results in small biopsies (3,13). Trastuzumab is expensive and its use is not without risk and is known to potentially cause significant cardiac side effects. Thus, finding noninvasive measures that may help predict response to HER2-directed therapies that also overcome sampling issues inherent in small biopsies can be of clinical value (14).
Chen et al. (15) recently identified a relationship between HER2 positivity and decreased SUVmax in gastric cancers of all anatomic subtypes; however, to our knowledge this is the first study comparing the radiologic SUVmax from patients with HER2+ and HER2− GC/GEJC matched by age, sex, tumor size, and histology. There was no significant difference in SUVmax between the 2 groups, and hence the metabolic signature cannot be used to predict HER2 expression status of GC/GEJC on initial staging. However, there was a significant association of high SUVmax with worse survival, with patients with SUVmax above 6.6 showing a mean survival of 12.2 mo. In addition, the mean SUVmax of all patients who died was higher (10.0 vs. 7.7), and the cumulative likelihood of death with an SUVmax more than 6.6 was 60% over 4 y. Taken together, these findings suggest that the metabolic signature (SUVmax) is a useful indicator of biologic aggressiveness and survival. This finding is not entirely surprising, having been replicated previously in gastric carcinoma (16–18). When adding the variable of tumor differentiation (identified at biopsy), cases with an SUVmax above 6.6 and poor differentiation (high grade) showed a shorter interval to death than low-grade tumors, although this trend was not significant.
The strength of this study rests on its direct comparison between the radiologic and pathologic parameters in 1 cohort using prognosis as the outcome. Moreover, we found no difference in tumor size, histologic type, or lymph node metastasis among HER2+ and HER2− cases, all of which are parameters that have been shown to demonstrate differential 18F-FDG uptake (17,19–21). Our study does not address the pathobiologic link between HER2 overexpression and tumor metabolic activity. If HER2 overexpression is indeed associated with increased gastric tumor metabolic activity, as has been shown previously in the breast (22), then the lack of a difference between HER2 groups in SUVmax could reflect tumor heterogeneity. If true, this reflects a significant weakness in the current HER2 testing on limited biopsy samples. Alternatively, gastric HER2+ overexpression may have no correlation with increased glycolysis or glucose transporter expression, pathobiologic factors that have been shown to be independently linked to higher 18F-FDG uptake in the GC/GEJ (19–21,23). Additional studies examining the relationship of HER2 and mechanisms of metabolism in gastric cancer are required. An additional caveat is that the metabolic signature of tumors can show variability after treatment as noted in a previous study, and this may also be a valuable tool in assessing the molecular genotype (24), survival, or treatment strategies at the initial staging or restaging phase.
Our study did not show any difference in several clinicopathologic parameters including patient age, sex, or tumor size with regards to HER2+ and HER2− status of the patients. These findings are similar to many previous studies, but other, discrepant findings have also been reported in the literature (13,25–30). Recent meta-analyses also show conflicting conclusions regarding effect of HER2 expression on patient survival (8,13). Indeed, the correlation of HER2 expression in gastric carcinoma with various clinicopathologic parameters and survival remains controversial. Chief among cited reasons for these discrepancies is variability in pathologic HER2 assessment methodologies (29). The immunohistochemistry and fluorescence in situ hybridization methods used in our laboratory have been validated and reproduced, and are currently considered standard of care (5). HER2 overexpression clearly characterizes a subset of GC/GEJC that benefits from targeted therapy, but the clinical and pathologic consequences of this finding still remain largely unclear.
Our study has some limitations. The cohort, particularly the HER2+ patients, is small for a comparison study. This can be explained in part because the prevalence of HER2+ gastric cases in our hands is relatively low compared with the others reported in the literature (25,31). This may be due to several preanalytical variables, such as the antibody used for immunohistochemistry. Although, the performance of the Dako HercepTest A0485 antibody seems comparable with the Ventana 4B5 (32), a recent study that directly compared results of these antibodies showed a slightly better performance with the Ventana system (33). For the purposes of this investigation, increased specificity allows us to be confident that our HER2+ cases are truly HER2-overexpressing at the molecular/genetic level. Tumor heterogeneity is well recognized in HER2 expression in GC/GEJC, and cases that are negative on biopsies may show different results on resection specimens, and the chances of positivity is increased when multiple blocks are used. In this study, we tested either the biopsy or the resection, whichever specimen was available before therapy, and only 1 block was tested in each case.
CONCLUSION
We present the first study comparing tumor SUVmax and HER2 status in age- and sex-matched patients with GC/GEJC. We did not find a significant difference in SUVmax between HER2+ and HER2− cases. HER2 status did not predict overall survival; however, patients with higher metabolic signatures (irrespective of HER2 status) showed overall decreased survival. This effect is amplified when considering tumors, which—in addition to showing high metabolic signature—are also poorly differentiated. These findings elucidate important aspects of the pathobiology of GC/GEJC—higher metabolic signature (SUVmax) and poor differentiation are more indicative of clinical aggressiveness than HER2+ status. Further investigation using larger cohorts is required to replicate these findings and identify the most effective treatment strategies based on radiologic-pathologic correlation.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 27, 2016.
REFERENCES
- Received for publication July 31, 2016.
- Accepted for publication October 14, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.