


Article Figures & Data
Figures
- FIGURE 1.
Normal esophageal transit (single swallow). Sequential dynamic images (left, 0–25 s) demonstrate normal bolus transit through esophagus. Composite image (center) is produced by summing all images from the initial 30 s. Regions of interest (dotted lines) that define upper, middle, and lower thirds of esophagus are shown. Time–activity curves (right) show counts recorded in each region as bolus progresses down esophagus. Esophageal transit time (11 s) is measured from time–activity curves of leading to trailing edges of upper and lower thirds of esophagus.
- FIGURE 2.
Normal global esophageal emptying (multiple swallows). Sequential images at 15 s per image are shown (left). Region of interest (rectangular box) is drawn over entire esophagus. From this region, time–activity curve (right) is generated showing percentage of activity retained in esophagus at each time. Amount of activity retained after multiple swallows can be used to help characterize primary esophageal motor disorders (Fig. 3; Table 1) or to follow therapeutic interventions as in achalasia.
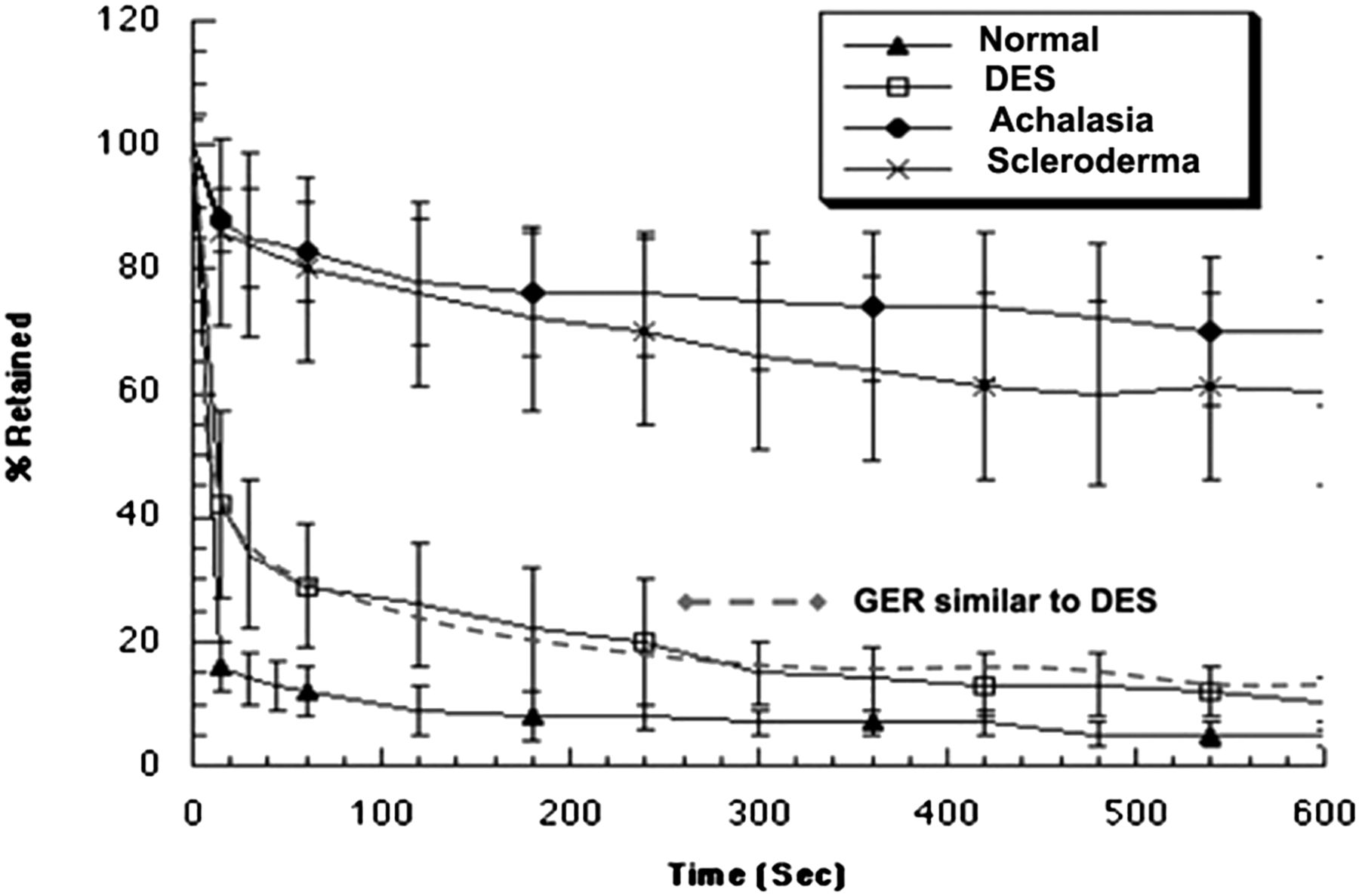
- FIGURE 3.
Esophageal emptying for primary esophageal motility disorders. Mean data for healthy subjects are shown compared with diffuse esophageal spasm (DES), achalasia, and scleroderma. Emptying curve for patients with esophagitis from gastroesophageal reflux is similar to DES. (Adapted from (75).)
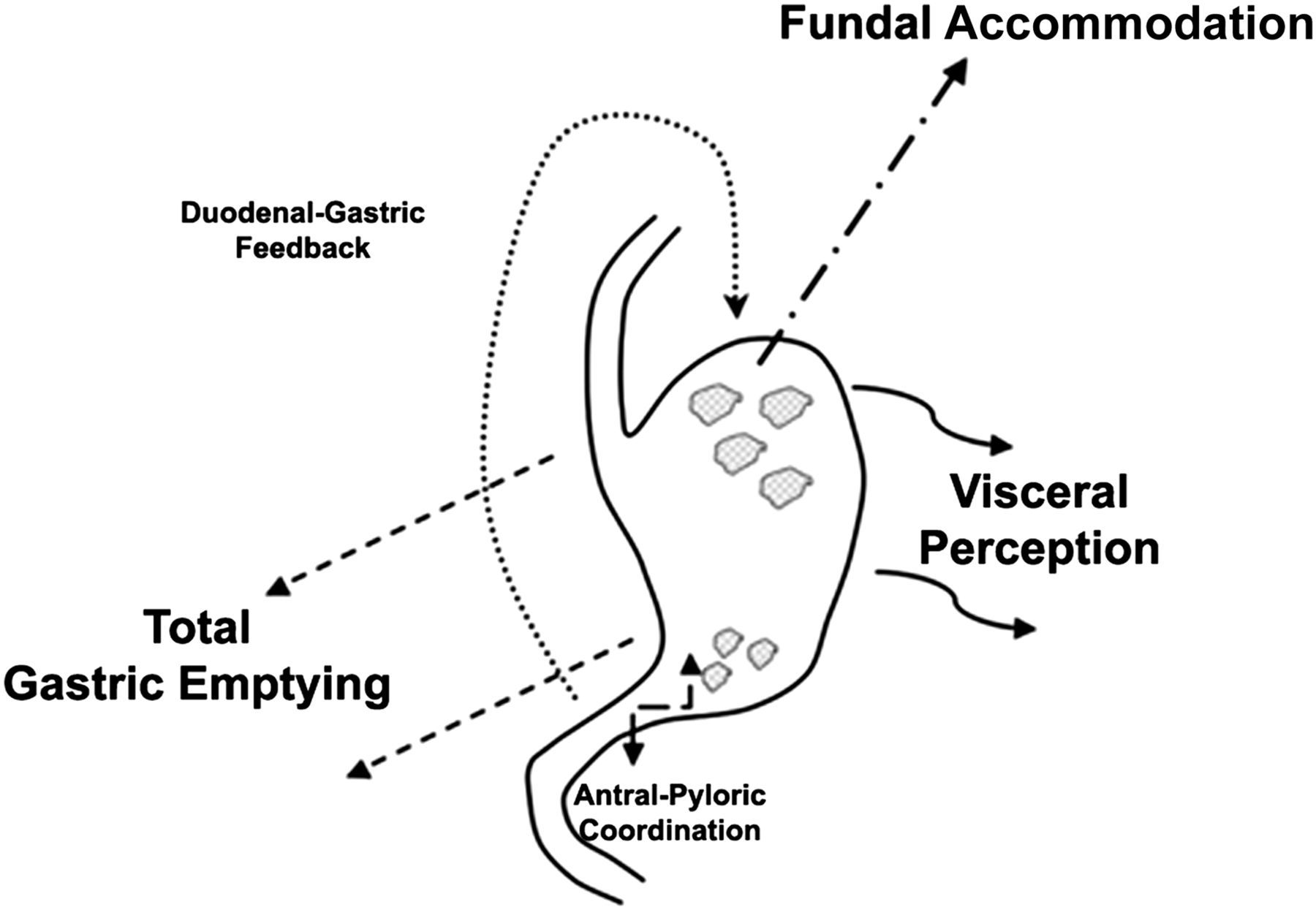
- FIGURE 4.
Multiple factors associated with GE are considered important to explain dyspeptic patient symptoms. Total GE, impaired fundal accommodation, and visceral hypersensitivity are 3 major factors currently under study. Antral–duodenal coordination and duodenal–gastric feedback mechanisms are also considered important but are not as well characterized. (Modified from (76).)
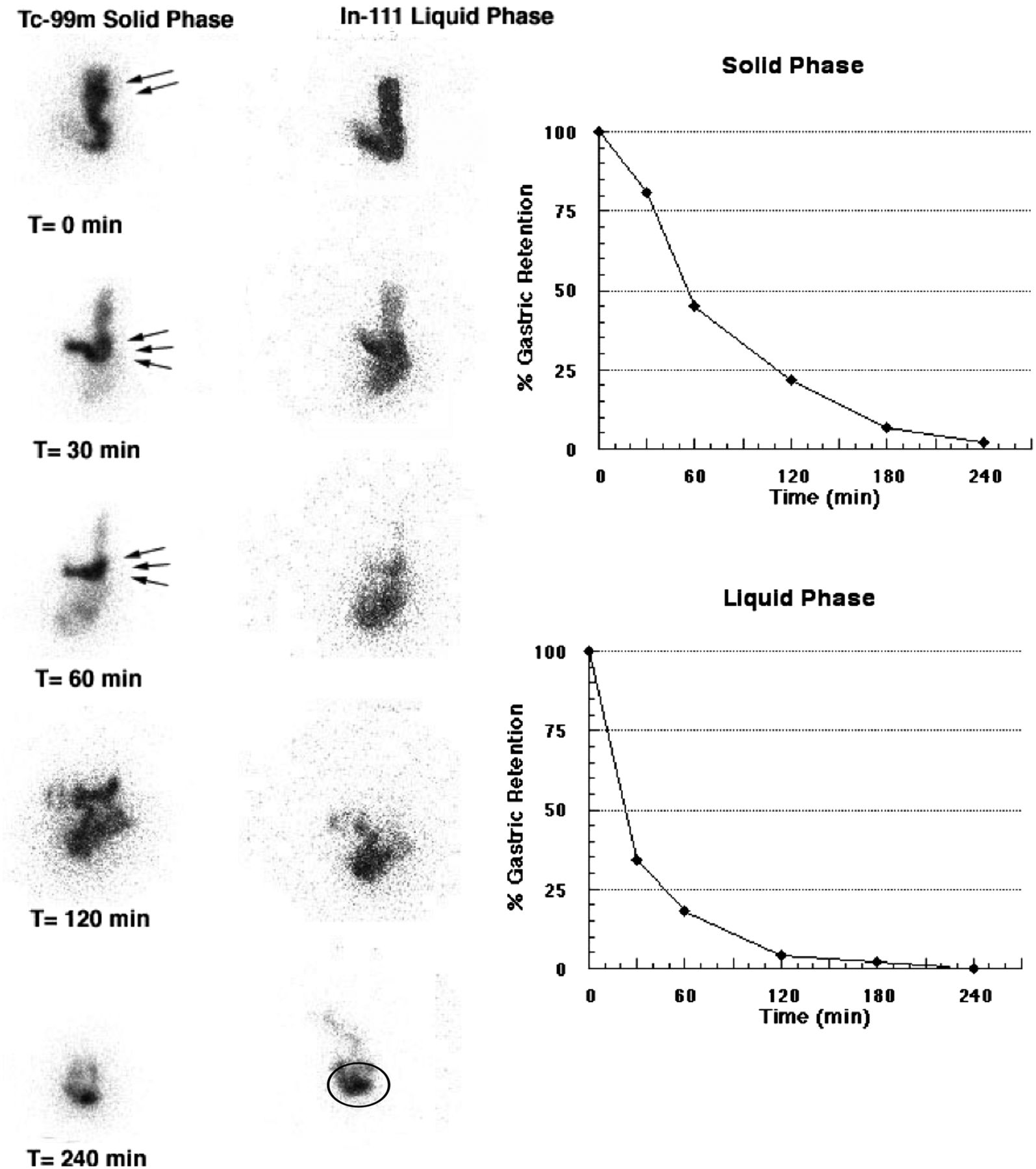
- FIGURE 5.
Normal dual-isotope, solid–liquid GE study (anterior views only). These images demonstrate early rapid distribution of liquids throughout stomach at 0 min. Liquid emptying curve is monoexponential. In contrast, solids show preferential early fundal localization (accommodation) (double arrows). Over time, solids progress down into antrum (triple arrows). Solid emptying curve is sigmoidal because of early lag phase for solids. Over time, one can observe small-bowel transit of solids and liquids, with buildup of activity in the terminal ileum (oval region of interest).
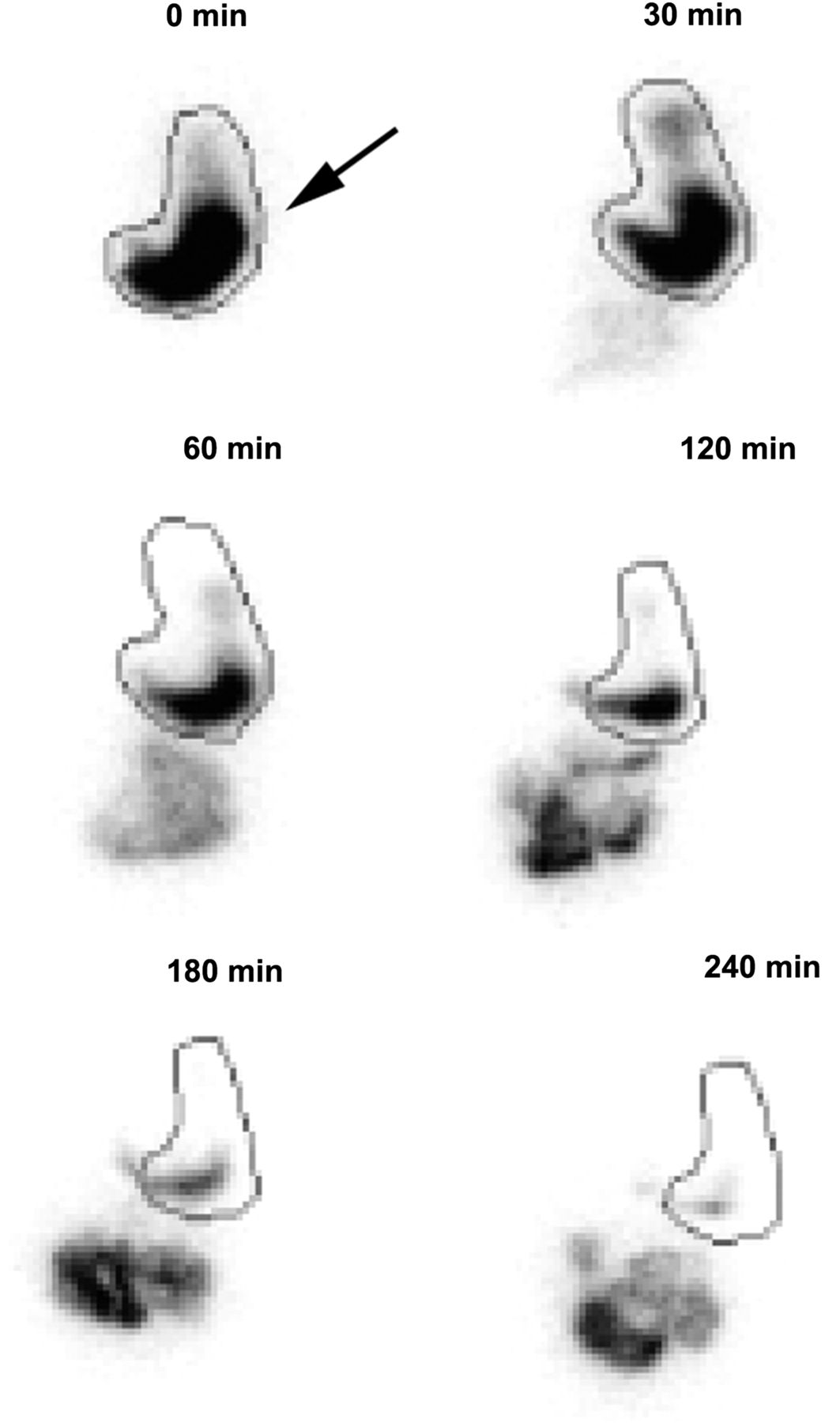
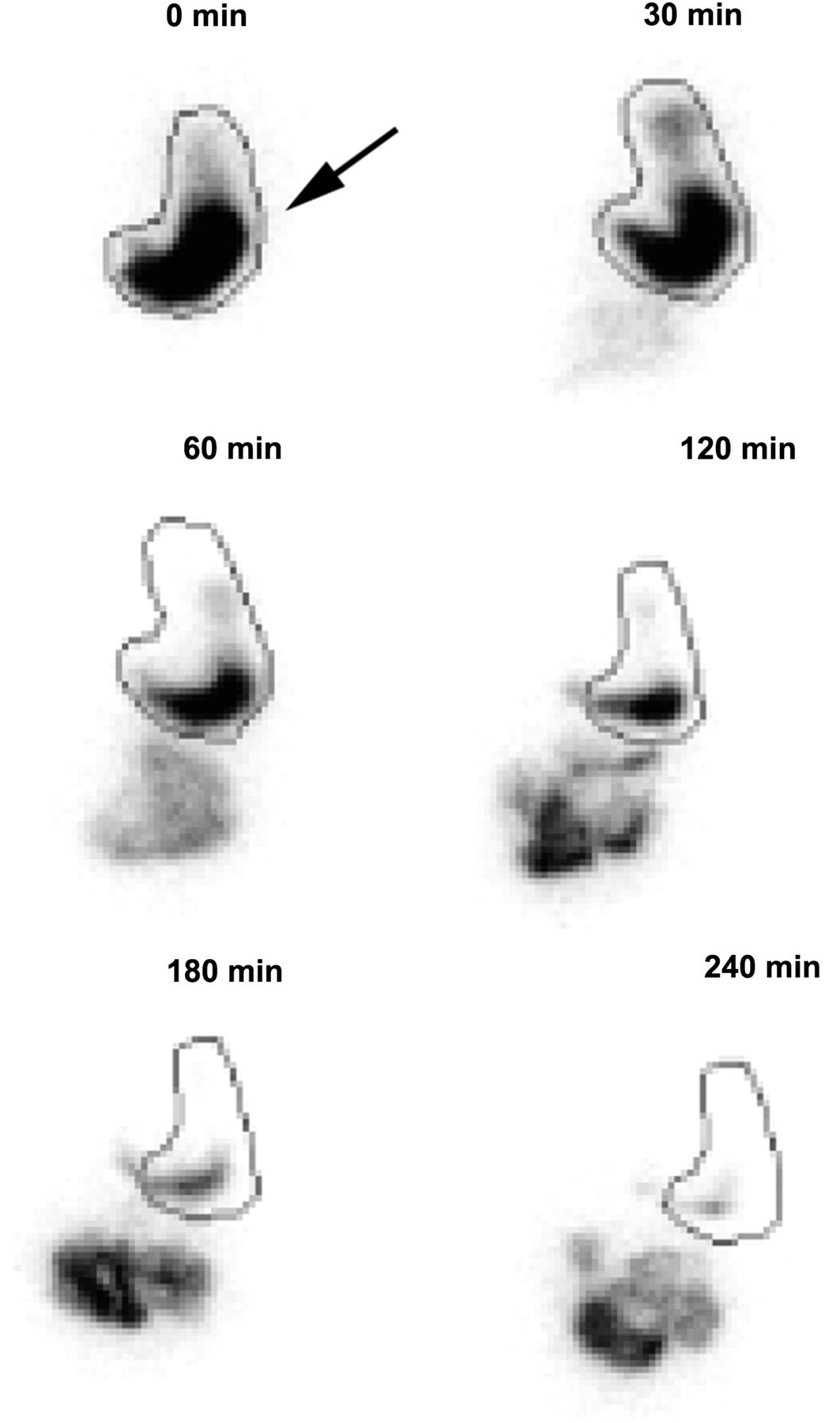
- FIGURE 6.
Impaired fundal accommodation (anterior views only). First postmeal ingestion image (0 min) shows lack of normal fundal accommodation, with most of meal being seen in distal stomach rather than in fundus (arrow). Overall GE was normal, with 42% of meal retained at 120 min and 8% at 240 min.


Tables
Adult Infant Child/adolescent A: Esophageal G1: Infant regurgitation H1: Vomiting and aerophagia A1: Heartburn G2: Infant rumination H1a: Rumination A2: Chest pain G3: Cyclic vomiting H1b: Cyclic vomiting A3: Dysphagia G4: Infant colic H1c: Aerophagia A4: Globus G5: Functional diarrhea H2: Abdominal pain B: Gastroduodenal G6: Infant dyschezia H2a: Dyspepsia B1: Dyspepsia G7: Functional constipation H2b: Irritable bowel B2: Belching H2c: Abdominal migraine B3: Nausea/vomiting H2d: Childhood abdominal pain B4: Rumination H3: Constipation and incontinence C: Bowel H3a: Functional constipation C1: Irritable bowel H3b: Nonretentive fecal incontinence C2: Bloating C3: Constipation C4: Diarrhea C5: Unspecified D: Functional abdominal pain E: Biliary F: Anorectal Condition Visual bolus transit analysis from dynamic display Esophageal transit time Esophageal retention at 10 min Normal Normal aboral bolus transit through upper, middle, and lower thirds of esophagus with normal relaxation of lower esophageal sphincter <14 s <18% Nonspecific esophageal motility disorder Any localized abnormal retrograde–antegrade bolus movement (normal movement is mild, transient, and retrograde in distal esophagus before relaxation of lower esophageal sphincter, which clears rapidly) >14 s >18% Isolated lower esophageal sphincter dysfunction Normal bolus transit in upper and middle esophagus with delayed transit localized at gastroesophageal junction >14 s Usually <18%; may see mild retention of <30% Scleroderma Marked delay in bolus transit, typically localized to distal esophagus >30 s >30%, with marked improvement when upright Diffuse esophageal spasm Repetitive retrograde–antegrade contractions throughout esophagus >14 s Normal or mild retention, <30% Achalasia Marked delay in bolus transit throughout esophagus (may progress normally in upper esophagus from oropharyngeal propulsion) >30 s >50%, with no improvement when upright





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}