


Abstract
Peripheral vascular disease (PVD) is an atherosclerotic disease affecting the lower extremities, resulting in skeletal muscle ischemia, intermittent claudication, and, in more severe stages of disease, limb amputation and death. The evaluation of therapy in this patient population can be challenging, as the standard clinical indices are insensitive to assessment of regional alterations in skeletal muscle physiology. Radiotracer imaging of the lower extremities with techniques such as PET and SPECT can provide a noninvasive quantitative technique for the evaluation of the pathophysiology associated with PVD and may complement clinical indices and other imaging approaches. This review discusses the progress in radiotracer-based evaluation of PVD and highlights recent advancements in molecular imaging with potential for clinical application.
Peripheral vascular disease (PVD) is a progressive atherosclerotic process that results in stenosis or occlusion of noncoronary blood vessels. Although PVD can affect the arteries, veins, and lymphatics, primary interest has been focused on the effects on the arteries supplying the lower extremities. PVD affects approximately 8 million Americans (1) and an estimated 10% of the worldwide population (2), with increasing prevalence in older individuals (3). PVD has significant health implications, resulting in progressive limb ischemia that can lead to life-altering claudication, nonhealing ulcers, limb amputation, and, in severe cases, death (2). Despite these numbers and a close association with coronary artery disease, PVD still remains a relatively underdiagnosed disease (4).
Several techniques have been used for the evaluation and detection of PVD, including ankle–brachial indices, duplex ultrasound, MR imaging, CT angiography, SPECT, and PET (5,6). The ankle–brachial index is a widely applied diagnostic tool for the detection of PVD that uses the blood pressure differential between the upper and lower extremities to detect a functionally significant arterial obstruction, but this technique can be problematic in the setting of microvascular disease and medial calcification (7,8). Ultrasound is another relatively inexpensive, widely available, and fast diagnostic imaging tool compared with other imaging techniques, and these advantages have contributed to the routine application of this approach for screening and evaluation of PVD. Ultrasound, however, has limited penetration depth and is useful for assessment of only large-vessel blood flow (6). MR imaging has increased spatial resolution and tissue penetration and also allows for the evaluation of lower-extremity tissue perfusion and oxygenation in PVD patients (9–11). However, MR techniques are limited by their insensitivity to measure perfusion at rest and usually require exercise or protocols to provoke reactive hyperemia in order to generate an adequate augmentation of flow. Additionally, MR has decreased sensitivity for targeted molecular imaging and has fewer imaging probes available than nuclear imaging approaches (12). CT angiography allows for visualization of vessel morphology and is commonly used to assess the severity of PVD and to guide vascular interventions; however, quantitative tools for assessing the arterial tree in vivo are not readily available in the clinical setting (13).
Nuclear imaging approaches provide high sensitivity and, when applied with biologically targeted radiotracers, offer potentially novel methods for the investigation of PVD, with integration of perfusion and assessment of tissue oxygenation, metabolism, or biologic processes such as angiogenesis (Table 1) (6). SPECT and PET are the primary nuclear imaging modalities, with SPECT being more established, less expensive, and more widely available. SPECT imaging also allows the simultaneous evaluation of multiple radiotracers. PET imaging provides increased sensitivity and resolution and generally involves radiotracers with shorter half-lives, resulting in lower levels of ionizing radiation exposure to patients. Both SPECT and PET, although providing higher sensitivity, also have lower spatial resolution when compared with CT and MR (submillimeter to ∼1 mm resolution). The recent emergence of hybrid SPECT/CT and PET/CT systems, however, has allowed for the colocalization of high-sensitivity SPECT and PET imaging (within the picomolar range) with high-resolution anatomic imaging to optimally localize and quantify radiotracer uptake. Additionally, these hybrid imaging systems now permit correction of attenuation and partial-volume effects, allowing for more precise radiotracer quantification within anatomically defined regions of interest (12). This review discusses the progression of radiotracer-based assessment of PVD and highlights targeted imaging approaches that may offer new directions for investigation and clinical application.
Radiotracers for Perfusion and Molecular Imaging of PVD
RADIOTRACER IMAGING OF PVD
Assessment of Lower-Extremity Perfusion and Blood Flow
Impaired lower-extremity perfusion is a key pathophysiologic mechanism that drives the complications associated with PVD (14), making assessment of perfusion a valuable tool for evaluation of disease progression and the effectiveness of therapy. The first nuclear medicine studies examining lower-extremity skeletal muscle blood flow in patients with vascular disease evaluated the clearance rates of 24Na-chloride (15), 133Xe (16), and 99mTc-pertechnetate (17) after intramuscular injection of these radiotracers. The development of nuclear medicine in later years led to 2-dimensional imaging of microspheres and albumin that were radiolabeled with 99mTc (18), 131I-sodium (19), and 111In (20) to measure lower-extremity perfusion; however, these techniques were not ideal, as they required invasive intraarterial injections to evaluate blood flow during the first pass through the circulation. The need for techniques that did not require intraarterial injections ultimately led to the incorporation of 201Tl as a perfusion agent in many imaging studies (7,21). 201Tl is a diffusible tracer with biologic properties similar to potassium, allowing for transport into viable cells via the sodium–potassium pump (22), thus making the tracer uptake a reliable measure of both myocardial (23) and skeletal muscle perfusion (21,24–26). 201Tl perfusion imaging can be performed after an intravenous injection at rest or during exercise and has a high first-pass extraction (∼85%), providing a reliable estimate of flow over a wide physiologic range (23). Whole-body 201Tl scintigraphy has been shown to be useful for evaluating perfusion abnormalities in the lower extremities of PVD patients at rest and during exercise stress (25,26), as well as in the identification of perfusion abnormalities in asymptomatic patients presenting with normal ankle–brachial indices (7). The assessment of PVD severity has traditionally been based on determining ratios of activity between nonstenotic and stenotic legs, or normalizing activity in lower-extremity regions of interest to whole-body activity in the presence of bilateral disease (7,21,27). With the emergence of 3-dimensional SPECT imaging systems, it was possible to more accurately detect and localize regions of lower-extremity ischemia under both rest and stress conditions with 201Tl (24). One of the first lower-extremity imaging studies to use 201Tl SPECT for the investigation of PVD evaluated stress profile curves from multiple transverse images in the leg during reactive hyperemia with normalization of regional activity to whole-body activity (Fig. 1) (24).
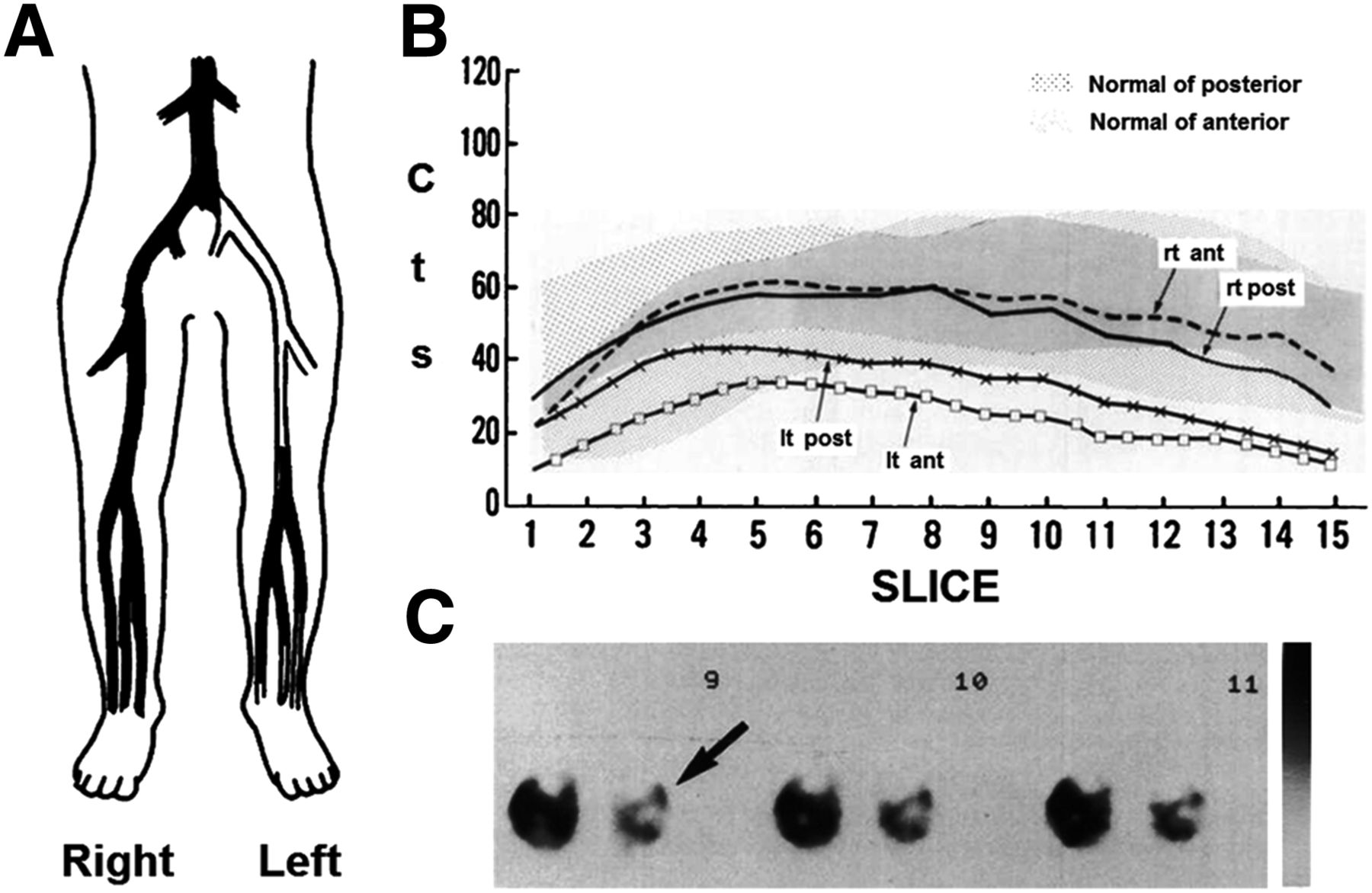
Arteriography (A) demonstrates unilateral PVD, which is confirmed by abnormal 201Tl SPECT stress perfusion profile curves of anterior and posterior tibial muscle components of the left leg (B) as well as visual inspection of 201Tl SPECT transverse images (C; perfusion defect noted by arrow). (Reprinted from (24).)
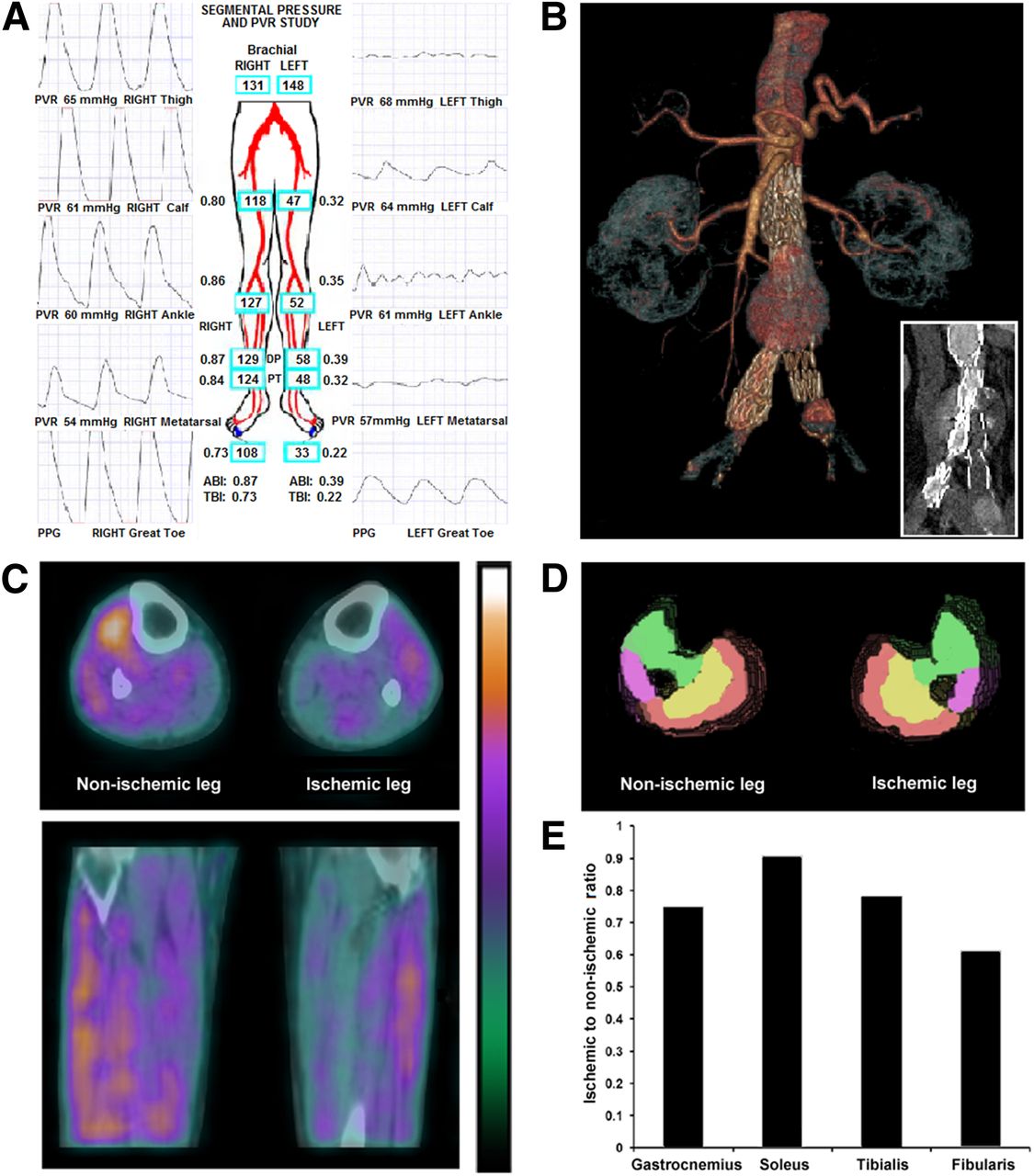
Although 201Tl has proven to be an effective technique in multiple studies, the long half-life and less favorable imaging characteristics compared with 99mTc-labeled radiotracers has resulted in the adoption of these newer 99mTc-labeled perfusion tracers that provide better image quality (28). Additionally, 99mTc-labeled compounds demonstrate little redistribution, allowing for injections during treadmill exercise and measures of peak exercise perfusion at a delayed imaging time (28). The biodistribution and kinetics of the 99mTc-labeled compounds also make it possible to perform lower-extremity perfusion measurements in combination with myocardial perfusion (27). One 99mTc-labeled compound in particular, 99mTc-sestamibi, has been incorporated in several studies examining lower-extremity perfusion in PVD (27,29,30). Application of 99mTc-sestamibi imaging in patients has revealed improved sensitivity for detecting differences in resting perfusion between the lower extremities of PVD patients with unilateral disease and improved sensitivity compared with Doppler ultrasound for the detection of PVD (31). Preliminary data from our lab have shown that SPECT/CT imaging with 99mTc-tetrofosmin also has potential for assessing regional differences in lower-extremity perfusion in PVD patients with abnormal CT angiography findings and ankle–brachial indices (Fig. 2).
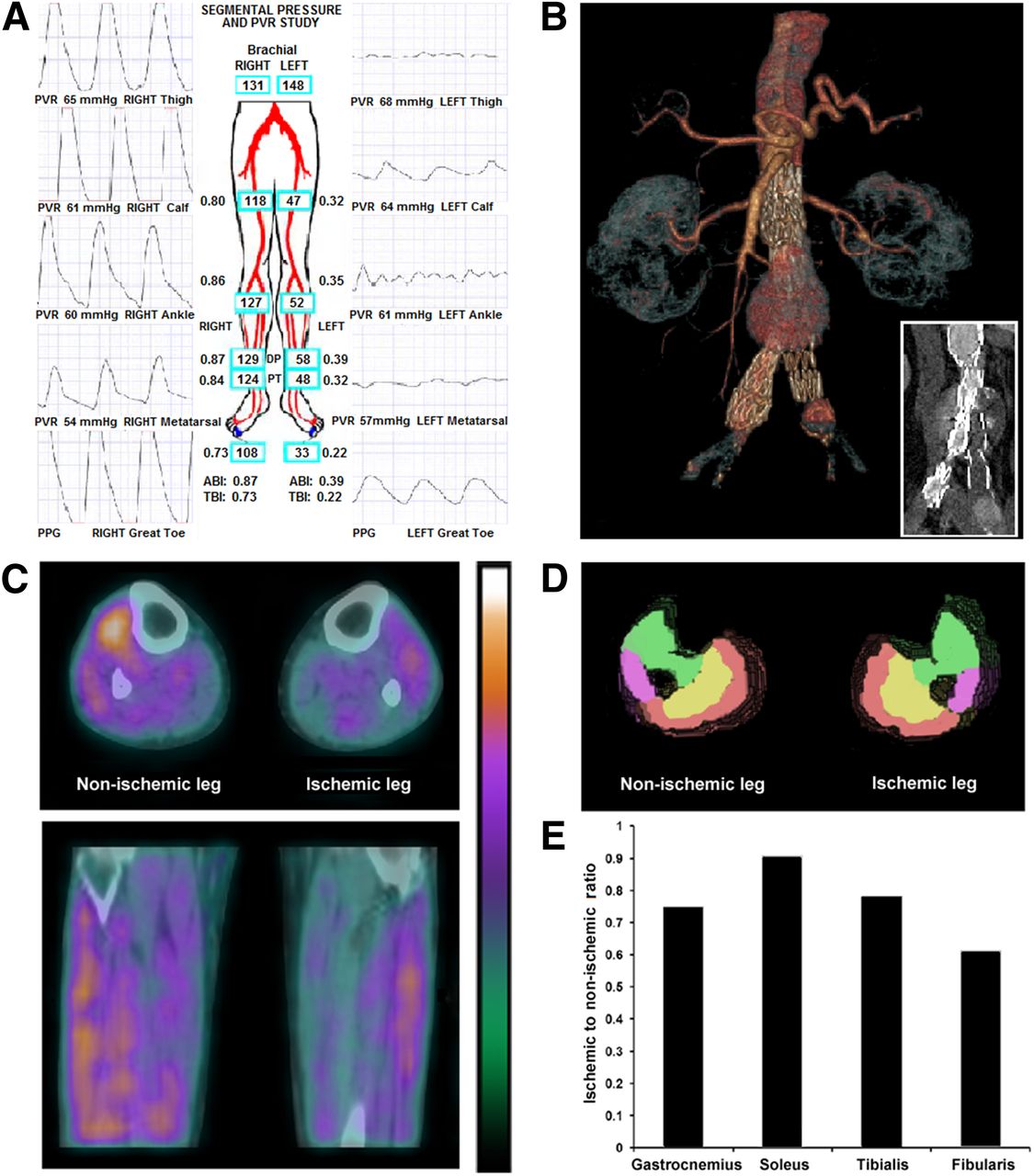
Multimodality evaluation with ankle–brachial indices (A), CT angiography (B), and hybrid 99mTc-tetrofosmin SPECT/CT (C) reveals impaired lower-extremity pressures and tissue perfusion in PVD patient with previously implanted aortoiliac stents (B). Segmentation of muscle groups into 3-dimensional regions of interest by CT attenuation images (D) confirmed differences in regional tissue perfusion between legs (E). Red = gastrocnemius; yellow = soleus; green = tibialis; purple = fibularis; ABI = ankle–brachial index; PPG = photoplethysmograph; PVR = pulse volume recording; TBI = toe–brachial index.
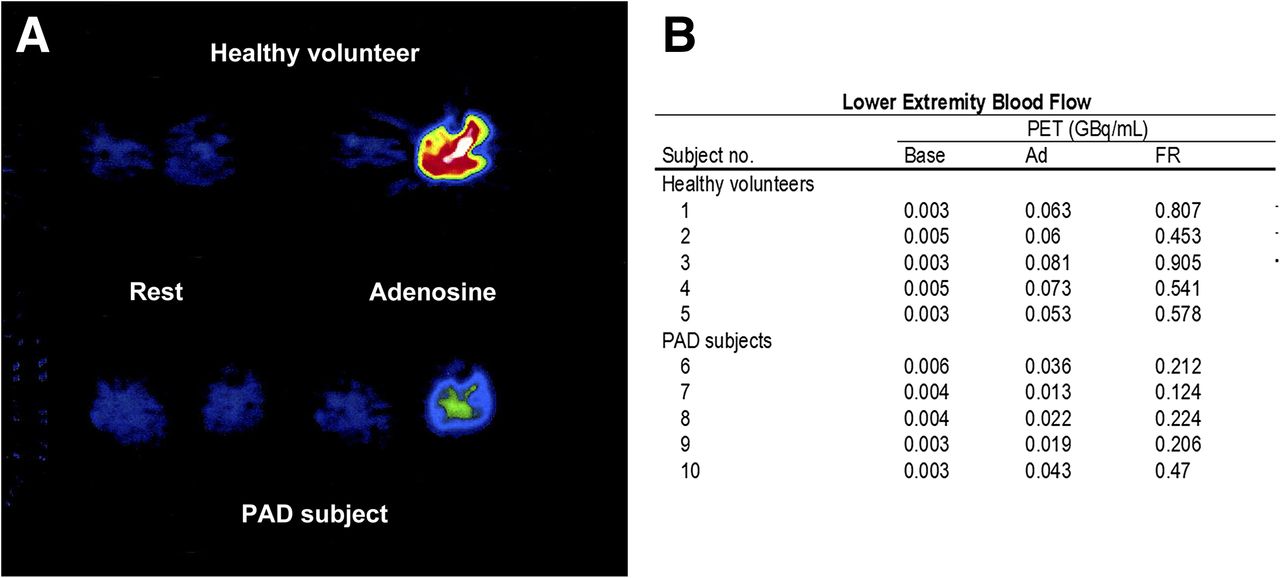
PET imaging can also assess lower-extremity blood flow in PVD (32–36). The primary PET radiotracer implemented in patient studies has been 15O-water (32,33,35,36), which can freely diffuse into tissue (37) and has a short half-life (∼2 min), making the tracer useful for repeated measurements of blood flow on the same individual in a single visit (33), at rest and during exercise (38,39), or during vasodilator stress (Fig. 3) (32). An 15O-water rest–stress PET study found significant differences in flow reserve within the calves of PVD patients when compared with healthy volunteers, and these differences correlated with thermodilution-derived flow reserve values (32). Another study found significantly reduced exercise-induced muscle blood flow in the distal legs of PVD patients who were referred for lower-limb amputation; these findings suggested that 15O-water PET imaging may be a valuable tool for determining the level of subsequent amputations (33). Kalliokoski et al. (39) demonstrated that PET assessment of blood flow and oxygen uptake in lower-extremity skeletal muscle may be a useful tool for evaluating patient responses to exercise training programs. However, they observed considerable variability in baseline PET flow measurements, and therefore complementary techniques such as angiography may be required for thorough evaluation of patients with PVD.
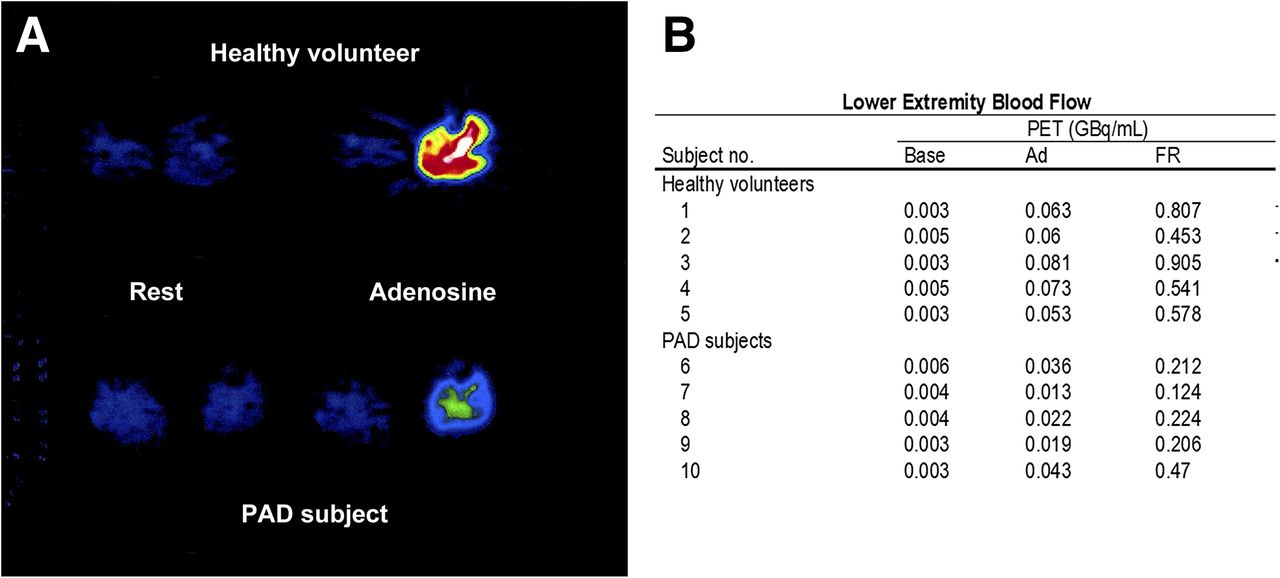
Lower-extremity PET H215O imaging of healthy subject and PVD patient during selective adenosine infusion into left leg (A). Baseline and adenosine stress blood flow was assessed, and flow reserve was expressed as ratio of adenosine flow to baseline flow (B). Flow reserve was significantly lower in PVD patients than in healthy subjects. (Reprinted from (32).).
PET imaging of preclinical animal models of PVD have been used to evaluate lower-extremity rest and stress blood flow and have demonstrated a high correlation (r2 = 0.98) between PET- and microsphere-derived blood flow values (34,40). In a murine model of PVD, PET imaging with 13N-ammonia has been used to assess acute and chronic changes in lower-extremity perfusion, showing a close correlation between PET perfusion results and histologic analysis of tissue fibrosis and necrosis (34).
Although PET imaging has proven to be useful for evaluating the lower extremities, the short half-life of available tracers can also present a limitation for lower-extremity PET imaging. Stress imaging with PET has traditionally required the use of exercise ergometers that are attached to scanners, as images must be acquired during or immediately after exercise stress. The recent development of an 18F-labeled perfusion agent (flurpiridaz) for myocardial perfusion, however, may assist with the promotion of exercise PET imaging of both the heart and the lower extremities. The longer half-life (∼110 min) of 18F-flurpiridaz allows for tracer injection during peak treadmill exercise and then serial evaluation of myocardial and skeletal muscle stress perfusion. The high extraction fraction of 18F-flurpiridaz in the myocardium may offer an advantage for evaluating lower-extremity skeletal muscle blood flow; however, this possibility still needs to be established (41).
Imaging of Angiogenesis
Targeted imaging of peripheral angiogenesis, in combination with lower-extremity perfusion imaging, may offer valuable information for in vivo assessment of the underlying pathophysiology associated with PVD. Angiogenesis, or the formation of new capillaries, is a complex process that involves various cell interactions and can be influenced by multiple stimuli, including lower-extremity ischemia (42). Radiotracer imaging of angiogenesis can focus on multiple regulatory targets, such as nonendothelial targets (e.g., monocytes, macrophages, and stem cells), endothelial cell targets (e.g., growth factor receptors, integrins, CD13, and cell adhesion molecules), extracellular matrix proteins, and proteases (43). Although many targets are potentially available for in vivo assessment of angiogenesis (Table 1), imaging studies investigating angiogenesis in the setting of limb ischemia have been primarily directed at vascular endothelial growth factor (VEGF) receptors and integrins, both of which play important roles in the process of angiogenesis (44).
VEGF ligands play a key role in the angiogenic process through binding to VEGF receptors (VEGF receptors 1–3), making VEGF receptors effective targets for the assessment of peripheral angiogenesis (45,46). A study by Lu et al. (45) demonstrated that targeted imaging of 111In-labeled recombinant human VEGF121, an angiogenic protein that is released in response to hypoxia and binds to VEGF receptors, could track ischemia-induced angiogenesis in a rabbit model. Another study used 64Cu-labeled VEGF121 to evaluate serial changes in VEGF receptor 2 expression in a murine model of hind limb ischemia with and without exercise training and found significantly higher levels of activity within ischemic limbs than in nonischemic contralateral limbs (46).
In addition to evaluating VEGF expression in preclinical models of PVD, studies have focused on targeted imaging of integrins (47–50). Integrins are transmembrane receptors that contribute to the angiogenic process through increased signal transduction as well as modulation of cell adhesion to the extracellular matrix (44). The αvβ3 integrin, which plays a key role in endothelial cell migration during angiogenesis (51), has gained significant attention for imaging of the angiogenic process (47–50). A study by Hua et al. (47) used a 99mTc-labeled peptide (NC100692) to target the αvβ3 integrin for serial assessment of angiogenesis in a murine model of hind limb ischemia. Immunofluorescent staining confirmed specific targeting of the αvβ3 integrin on endothelial cells. Another study also revealed increased retention of 99mTc-NC100692 within segmented regions of interest in proximal and distal muscles of the ischemic hind limb, with peak relative retention occurring 1 wk after femoral artery occlusion (48). In addition to 99mTc-labeled compounds, cyclic Arg-Gly-Asp (cRGD)–labeled 68Ga (49) and a 76Br-labeled dendritic nanoprobe (50) have been used to assess αvβ3 expression in murine models of hind limb ischemia. Studies using 68Ga- and 76Br-labeled tracers have also observed significantly higher levels of tracer retention (αvβ3 expression) in ischemic limbs at 1 wk after occlusion.
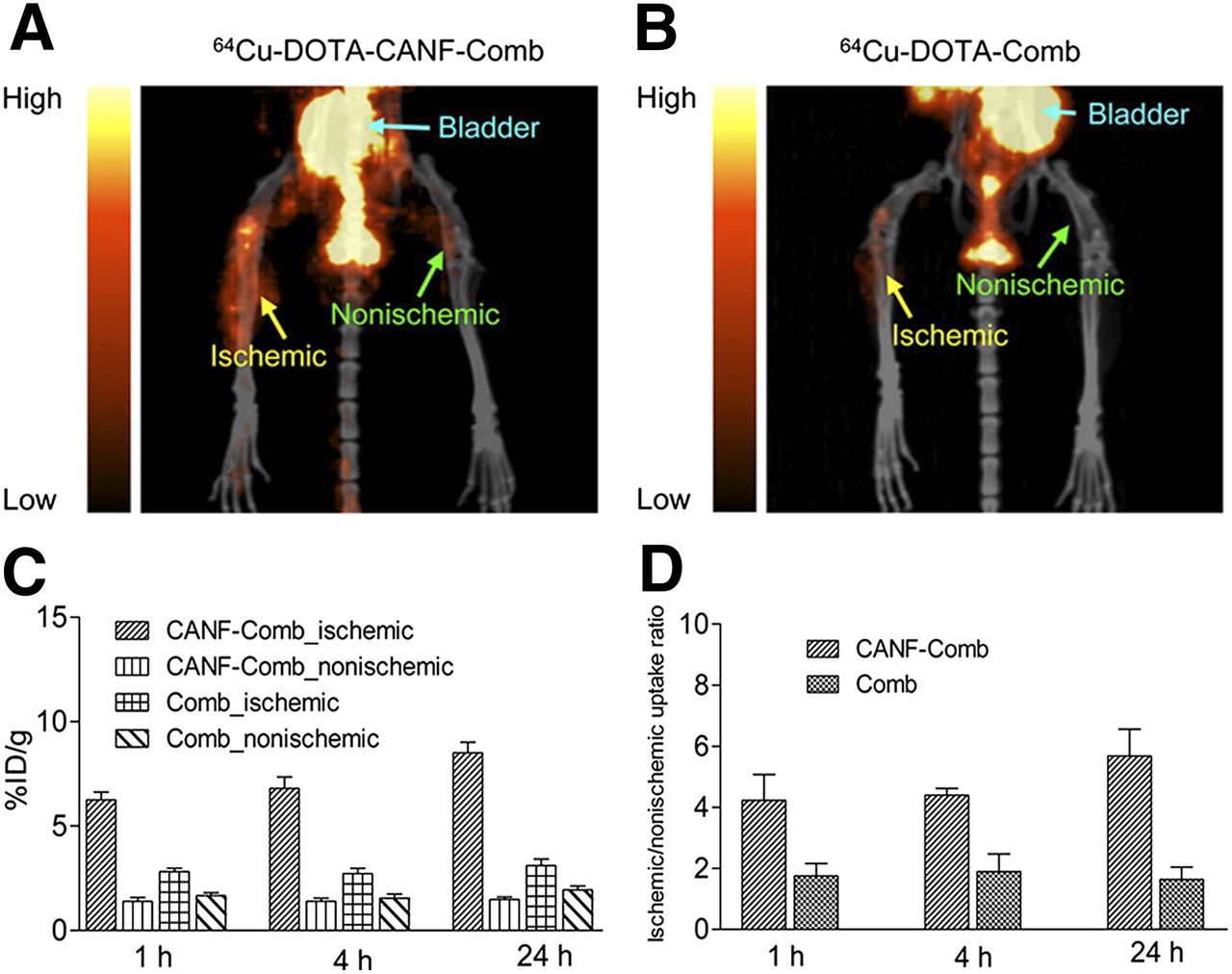
A more recent study has shown the feasibility of targeted PET imaging of angiogenesis with a 64Cu-labeled C-type atrial natriuretic factor–conjugated comblike nanoparticle that detects upregulation of natriuretic peptide clearance receptor (Fig. 4) (52). Natriuretic peptides are vascular homeostasis hormones that are secreted from heart and vasculature and function through interaction with their receptors, particularly natriuretic peptide clearance receptor (53). Liu et al. (52) compared PET nanoprobes developed for targeted and nontargeted PET imaging of natriuretic peptide clearance receptor in a murine model of hind limb ischemia. Targeted imaging with a receptor-specific nanoprobe proved to be highly sensitive to the angiogenic response when assessed 7 d after femoral artery ligation (Fig. 3), with immunohistochemistry confirming natriuretic peptide clearance receptor upregulation with colocalization in endothelial and smooth muscle cells.
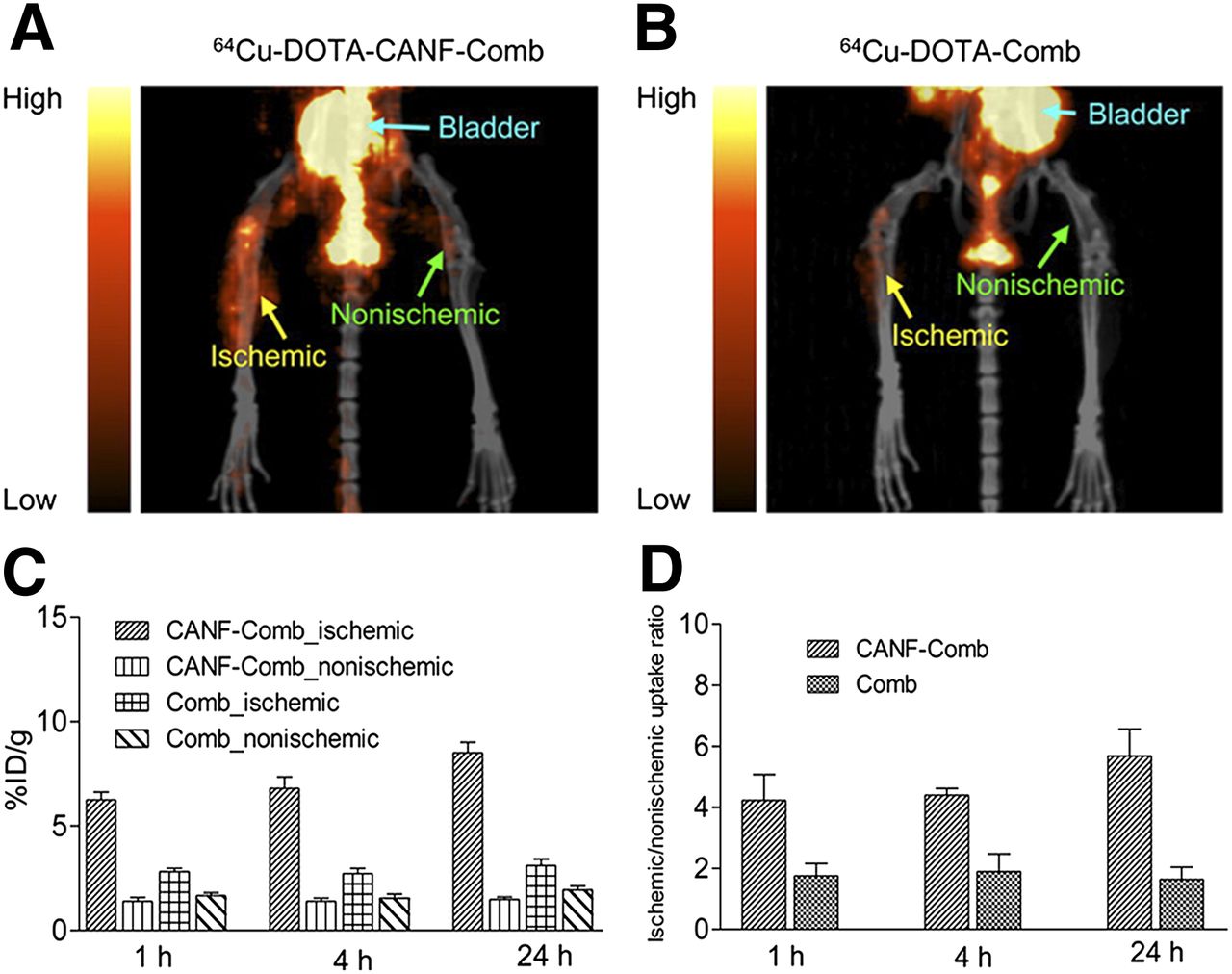
PET/CT imaging with 64Cu-DOTA–C-type atrial natriuretic factor–comb (A) and 64Cu-DOTA–comb (B) in mouse model of hind limb ischemia, 7 d after femoral artery occlusion. 64Cu-DOTA–C-type atrial natriuretic factor–comb uptake was significantly higher than uptake of 64Cu-DOTA–comb in ischemic limb when percentage injected tracer dose per gram of tissue (C) or ischemic-to-nonischemic leg ratios (D) were examined. (Reprinted from (52).) CANF = C-type atrial natriuretic factor.
Atherosclerosis Imaging
Although assessments of tissue perfusion, blood flow, and angiogenesis have potential for clinical application, recognition of unstable plaque that is vulnerable to rupture is another area of investigation. In recent years, the development of nuclear imaging probes for noninvasive assessment of plaque evolution and stability has grown substantially (Table 1) (54). The progression of plaque formation is generally characterized by expansive and restrictive vascular remodeling, with multiple signaling events and cell interactions contributing to these processes. Studies now regularly use atherosclerotic plaque localization and characterization obtained from CT and MR to facilitate quantification of radiotracer activity within lesions by normalization of tracer uptake in the vessel of interest to the blood activity in a remote artery. PET imaging offers spatial resolution superior to that of SPECT and therefore has been the favored modality for many in vivo imaging studies investigating atherosclerosis (54,55).
Among the currently available radiotracers for in vivo assessment of atherosclerosis, PET imaging of 18F-FDG has attracted attention (56). 18F-FDG is a glucose analog that is metabolized and converted to FDG-6 phosphate and subsequently trapped in the cytosol of metabolically active cells. This characteristic of 18F-FDG has resulted in the use for targeted PET imaging of activated macrophages, which are key mediators of the inflammatory response (57). Several clinical studies suggest that 18F-FDG imaging is highly reproducible (Fig. 5) (58) and correlates well with macrophage activity (59). However, a recent study did not find a significant correlation between 18F-FDG uptake in peripheral artery plaque and subsequent immunohistochemical staining of CD68, a measure of macrophage content (60). Although there are conflicting results as to the direct association between 18F-FDG uptake and plaque vulnerability, initial studies revealed an increased prevalence of vascular 18F-FDG uptake with increasing age and atherosclerotic risk factors (61,62). Cardiovascular risk factors have also been correlated with increased 18F-FDG uptake in specific peripheral arteries, making PET a potentially useful predictor of future cardiovascular events and tool for evaluating the effectiveness of medical therapy (63).
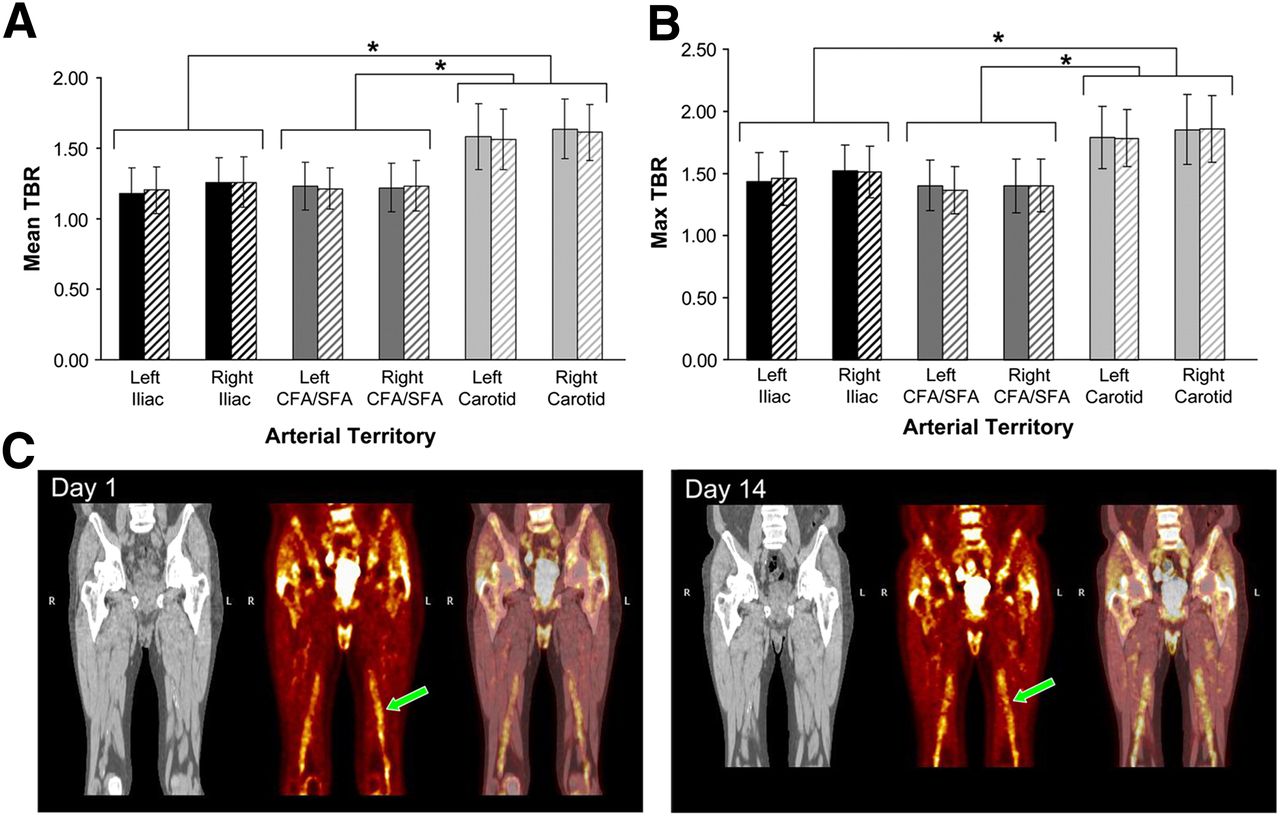
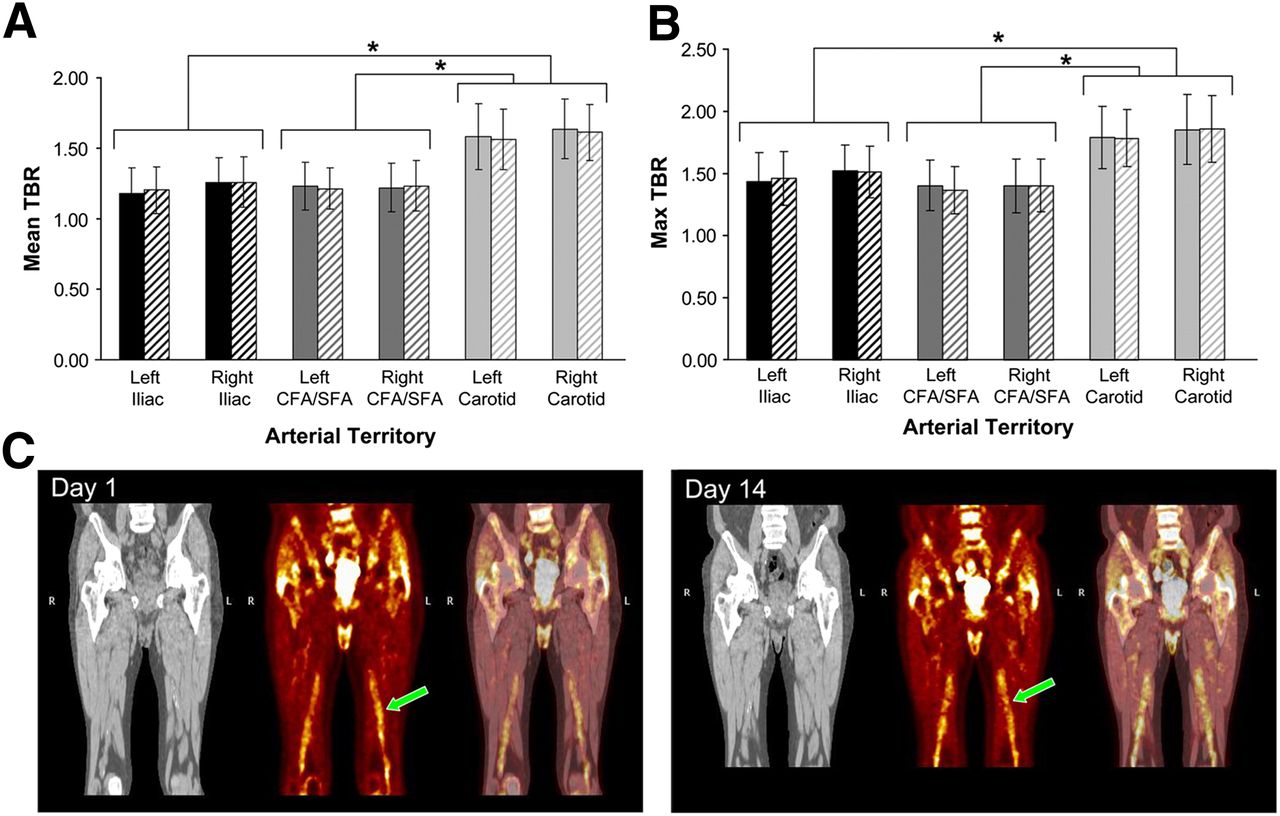
Analysis of mean (A) and maximum (B) 18F-FDG tumor-to-background ratios within multiple arterial regions on day 1 (solid bars) and 14 d later (hatched bars). No significant differences were observed within arterial regions across time. Carotid artery uptake was significantly higher than 18F-FDG uptake within lower-extremity arteries on days 1 and 14. 18F-FDG PET (C, middle) fused with CT imaging (C, right) revealed similar uptake in femoral arteries on days 1 and 14 (noted by arrows). CFA = common femoral artery; SFA = superficial femoral artery; TBR = tumor-to-background ratio. *P < 0.001. (Reprinted from (58).)
In addition to 18F-FDG, other PET radiotracers have also been developed for the evaluation of atherosclerosis in animal models and patients. Tracers have focused on various targets associated with atherosclerosis, including inflammatory cells, markers of extracellular matrix remodeling, and mediators of angiogenesis (Table 1); however, 18F-FDG is currently the only radiotracer that has been widely applied in the clinical setting (54,57,64). Few nuclear imaging studies have evaluated peripheral atherosclerosis to date (58,60,61,65–67), although 18F-FDG patient imaging has been shown to be highly reproducible when performed 2 wk apart (Fig. 5) (58). 18F-labeled sodium fluoride has also been used to investigate atherosclerotic plaque in peripheral vessels, with uptake being highest in the femoral artery (66). Additional preclinical studies with 64Cu-labeled natriuretic peptide and clinical studies using 11C-acetate have demonstrated increased radiotracer uptake within atherosclerotic lesions (65,67).
Developing Applications for Radiotracer-Based Investigation of PVD
Evaluation of deep vein thrombosis (DVT) in the lower extremities is a developing application for imaging of PVD that has garnered recent attention (68–71). Venous ultrasound is currently the most accepted tool for evaluating DVT; however, ultrasound is largely dependent on both operator skill and patient characteristics (72). Therefore, a more sensitive or specific technique might assist in the guidance of antithrombotic therapy. PET imaging has shown significantly higher uptake of 18F-FDG within thrombosed veins than within nonthrombosed veins, and 18F-FDG uptake has also been negatively correlated with time of DVT symptom onset, suggesting that 18F-FDG imaging may assist in the evaluation of DVT chronicity (68). Scintigraphy with the 99mTc-labeled peptide P280 (apcitide) has also been successfully applied in patients as a tool for detecting DVT (69). Based on the high affinity of the 99mTc-apcitide peptide to activated platelets, it may be possible to differentiate new from old thrombi, a clinically important distinction. 99mTc-apcitide imaging has been shown to possess high sensitivity and specificity for the detection of thrombi when compared with compression ultrasound and phlebography (70). Along with 99mTc-apcitide, another 99mTc-labeled peptide, recombinant tissue plasminogen, has also shown high sensitivity and specificity in the detection of thrombi (71). Together, these approaches may provide potential for improved detection and evaluation of lower-extremity DVT.
Hypoxia and acidosis may represent alternative markers for evaluation of PVD (73,74). Myocardial imaging with hypoxia markers has already proven to be effective and could be potentially translated to peripheral tissue to evaluate the balance of flow and oxygen consumption in ischemic limbs (74). The pH (low) insertion peptide, pHLIP, has emerged as a peptide that may be used to investigate changes in acidosis. At acidic pH levels, equilibrium is shifted toward the insertion of pHLIP into the cell membrane and results in tissue accumulation. Sosunov et al. (75) demonstrated that pHLIP can also be used to successfully target ischemic myocardium without requiring severe myocardial damage. Although there are currently no studies that have used pHLIP or hypoxia imaging in the investigation of PVD, future applications may enhance the understanding of the underlying pathophysiology of PVD and therapeutic interventions directed at improving angiogenesis, arteriogenesis, and tissue perfusion.
CONCLUSION
Approaches for radiotracer imaging of PVD continue to advance and show potential, with multiple molecular targets already available in preclinical models. Although many nuclear tracers have been developed, clinical application of molecular imaging in PVD has yet to reveal the full potential in patient populations. Continuing development of radiotracer imaging of PVD may provide effective, noninvasive techniques for evaluating serial responses to various forms of medical therapy, such as revascularization, exercise programs, and novel gene- or cell-based drug therapies. The high sensitivity of SPECT and PET imaging may be ideally suited for evaluation of these therapies and could complement anatomic and clinical indices for improved assessment of physiologic changes in PVD patients, providing potential guidance for vascular interventions as well as targeted delivery of drug therapies in the future.
Acknowledgments
We thank Da Yu Yu for assistance with the figures.
Footnotes
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than September 2018. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
REFERENCES
- Received for publication May 16, 2013.
- Accepted for publication August 14, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}