


Abstract
Preoperative lymphatic mapping in conjunction with intraoperative γ-probe detection is widely used for sentinel node localization in melanoma, breast cancer, and other malignancies. 99mTc-radiocolloids have been the standard radiotracers used for sentinel node mapping. 99mTc-tilmanocept is a receptor-binding molecular imaging agent approved by the U.S. Food and Drug Administration for lymphatic mapping and lymph node localization in breast cancer, melanoma, clinically node-negative squamous cell carcinoma of the oral cavity, and other solid tumors. It has several advantages over conventional radiocolloids, including rapid injection site clearance, high sentinel node extraction, and low distal node accumulation, which can lead to efficient resource use.
Lymphatic mapping with sentinel lymph node (SLN) localization has emerged as a valuable prognostic tool in the management of melanoma and early breast cancer. There are numerous definitions of an SLN based on location, lymphoscintigraphy interpretation, and use of a γ-detection probe or vital blue dye (VBD). Morton’s original definition that a sentinel node is “the first lymph node that receives afferent lymphatic drainage from a primary tumor” best reflects the concept of stepwise spread of cancer (1). Nodal involvement has a significant impact on tumor staging, treatment, and prognosis. However, in breast cancer, most studies show no change in survival or only a slightly reduced survival in patients with nodal micrometastasis compared with those without (2–4). Thus, lymphatic mapping and SLN localization have emerged as accurate and minimally invasive procedures for identifying clinically node-negative patients. Lymphatic mapping can be performed with radiotracers, VBD, or both. 99mTc-labeled radiocolloids have traditionally been used in nodal mapping. In the United States, filtered 99mTc-sulfur colloid (SC) is most commonly used. The other tracers include 99mTc-nanocolloid human serum albumin (Nanocoll; GE Healthcare) in Europe and 99mTc-antimony trisulfide in Australia and Canada (5). 99mTc-tilmanocept (Lymphoseek; Navidea) is a relatively new Food and Drug Administration–approved receptor-targeted radiotracer for mapping and localization of lymph nodes draining breast cancer or melanoma. It is also approved to guide SLN biopsy in patients with clinically node-negative squamous cell carcinoma of the oral cavity. On October 15, 2014, the Food and Drug Administration approved the expanded use of 99mTc-tilmanocept for lymphatic mapping in solid tumors (6). 99mTc-tilmanocept exhibits distinct advantages over radiocolloids, including rapid clearance of the injection site, high sentinel node extraction, and low distal node accumulation, which can lead to efficient use of resources in the clinic (5). This article reviews and summarizes the existing data on this new receptor-binding molecular imaging agent.
THE IDEAL RADIOTRACER
An ideal lymph node imaging agent would exhibit rapid clearance from the injection site, rapid uptake and high retention within the first draining lymph node, and low uptake by distal lymph nodes (7). The commonly used agents—unfiltered or filtered 99mTc-SC, albumin-based colloids, and 99mTc-antimony trisulfide colloid—do not exhibit all these characteristics. Furthermore, the ideal agent should have low radiation absorption, high biologic safety, rapid and stable 99mTc labeling, and radiochemical purity (8). Vera et al. reported the synthesis and preliminary biologic testing of a synthetic macromolecule, 99mTc-diethylenetriaminepentaacetic acid (DTPA)-mannosyl-dextran (the same as 99mTc-tilmanocept), for sentinel node detection and found that it exhibited the desired properties of rapid clearance from the injection site and low accumulation in distal nodes (9).
99MTC-TILMANOCEPT
Description of the Agent
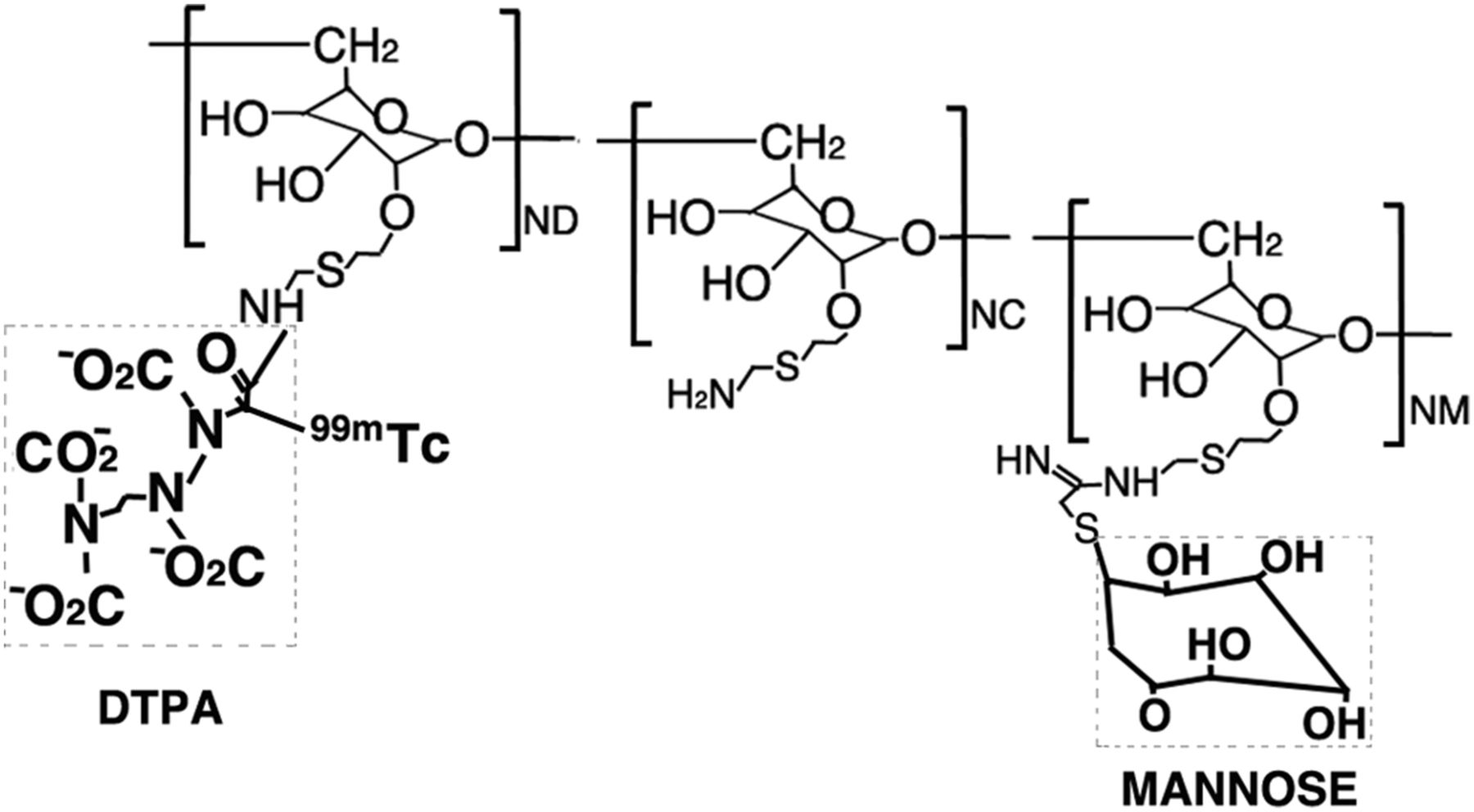
99mTc-tilmanocept is a novel radiopharmaceutical designed to overcome certain limitations of the conventionally used radiocolloids. It accumulates in lymphatic tissue by selectively targeting and binding to CD206 receptors on the surface of macrophages and dendritic cells, which are found in high concentration in lymph nodes (10). Tilmanocept is DTPA-mannosyl-dextran, a macromolecule with an average diameter of 7 nm. It consists of multiple units of DTPA and mannose, each covalently attached to a dextran backbone (Fig. 1). The mannose acts as a ligand for the CD206 receptor, and the DTPA moieties serve as the binding site for 99mTc. Its small size allows rapid lymphatic uptake, and the targeted receptor binding on macrophages and dendritic cells in lymph nodes limits its migration into the distal nodes (9). In contrast to 99mTc-tilmanocept, unfiltered 99mTc-SC particles have an average size ranging from 305 to 340 nm. Filtered 99mTc-SC particles are mostly between 100 and 220 nm, whereas 99mTc-nanocolloid human serum albumin and 99mTc-antimony trisulfide particles range from 5 to 100 nm and 3 to 30 nm, respectively (11).

Molecular structure of 99mTc-tilmanocept. It is composed of a dextran backbone to which multiple units of mannose and DTPA are attached. DTPA units serve as attachment sites for radioactive labeling with 99mTc. Mannose units provide a molecular mechanism by which 99mTc-tilmanocept binds to CD206 receptor specific to reticuloendothelial cells.
Chemically, 99mTc-tilmanocept consists of 99mTc, dextran 3-[(2-aminoethyl)thio]propyl-17-carboxy-10,13,16-tris(carboxymethyl)-8-oxo-4-thia-7,10,13,16-tetraazaheptadec-1-yl-3-[[2-[[1-imino-2-(d-mannopyranosylthio)ethyl]amino]ethyl]thio]propyl ether complexes. 99mTc-tilmanocept is supplied as a kit that is stored at room temperature and prepared by radiolabeling with 99mTc and diluting with the supplied diluent before use. Each vial provides doses for up to 4 patients. Some clinics may rely on private radiopharmacies to supply a prepared dose.
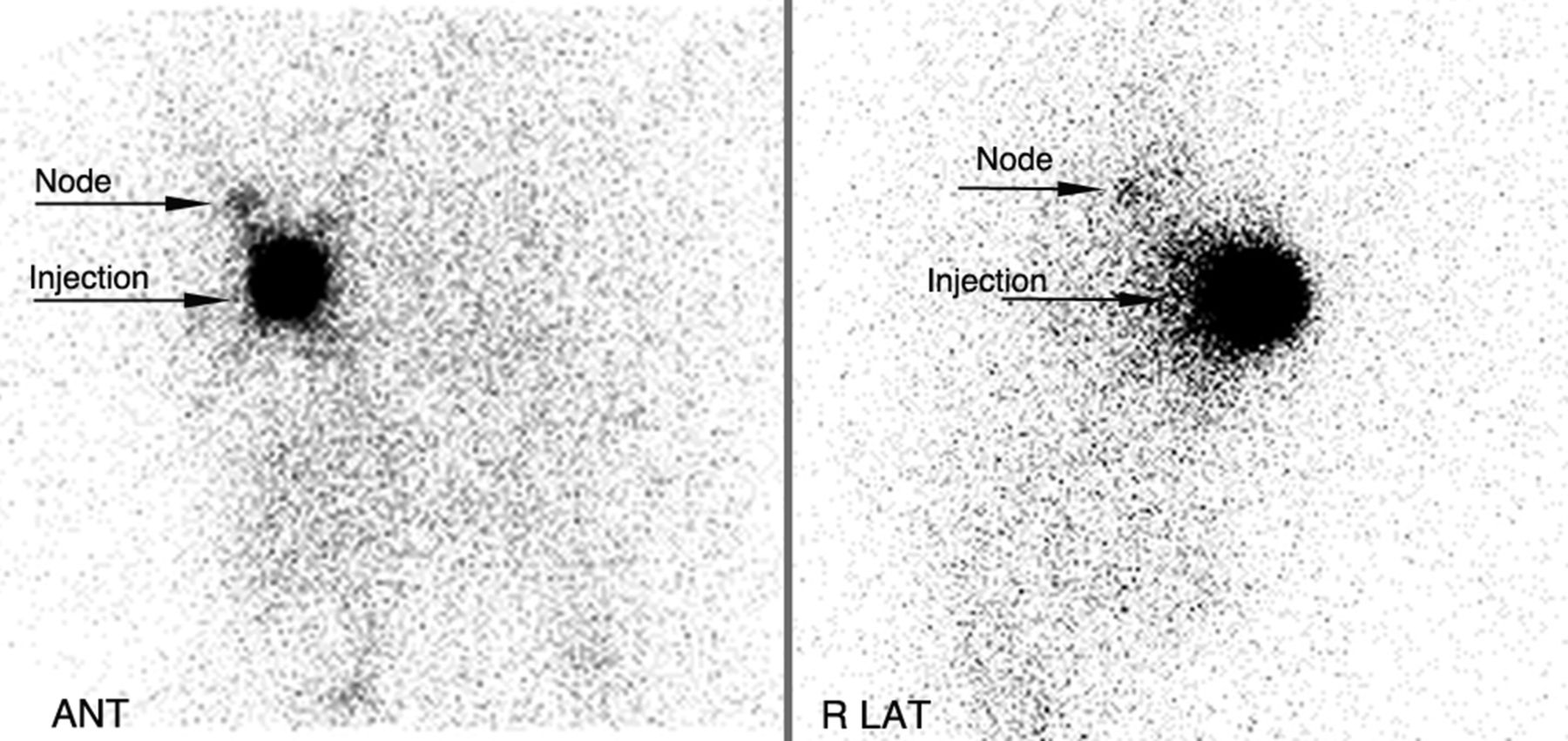
The recommended dose of 99mTc-tilmanocept is 18.5 MBq (0.5 mCi) as a radioactivity dose and 50 μg as a mass dose, administered at least 15 min before initiating intraoperative lymphatic mapping. Lymphatic mapping should be completed within 15 h of 99mTc-tilmanocept injection. The route of administration depends on the tumor location and the protocol of the clinic. Administration routes include intradermal and subcutaneous for breast cancer and melanoma, as well as subareolar and peritumoral for breast cancer. Injection volumes range from 0.1 to 1 mL given in a single injection or multiple injections depending on the indication and route of administration (10). Example 99mTc-tilmanocept images are shown in Figures 2–4.

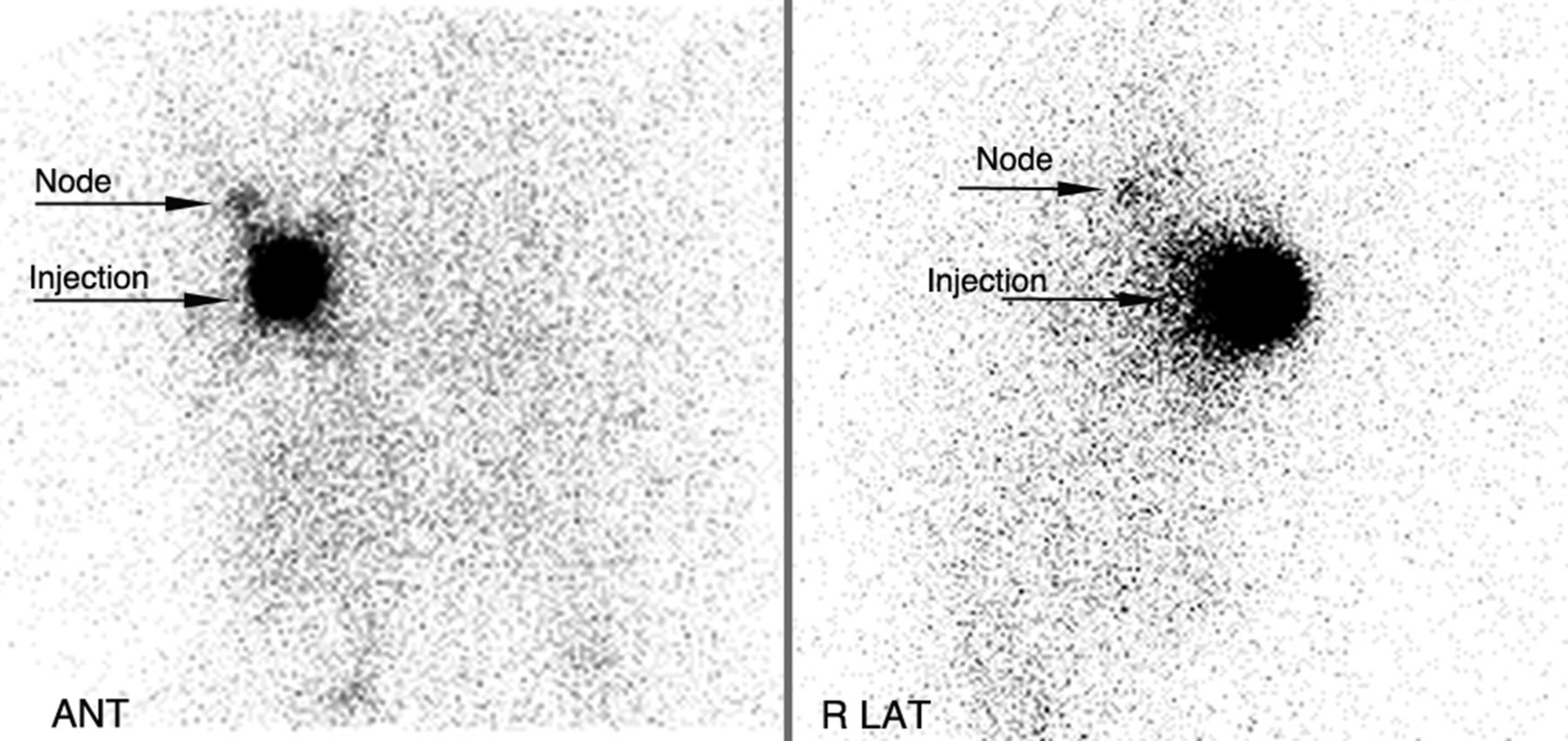
Squamous cell carcinoma in floor of mouth. 99mTc-tilmanocept was injected at tumor site, and anterior cervical nodes were visualized bilaterally. ANT = anterior; LAT = lateral.
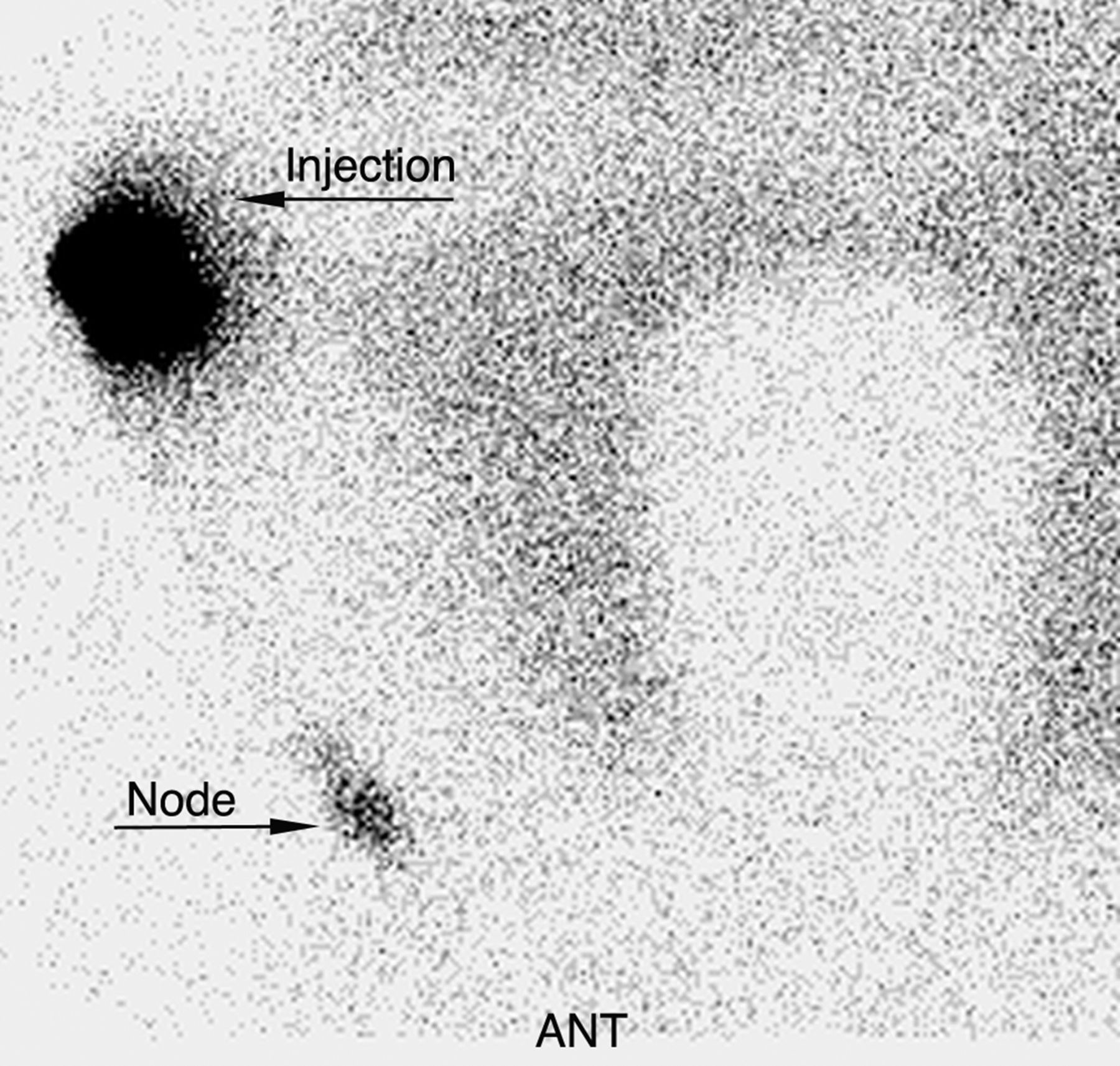
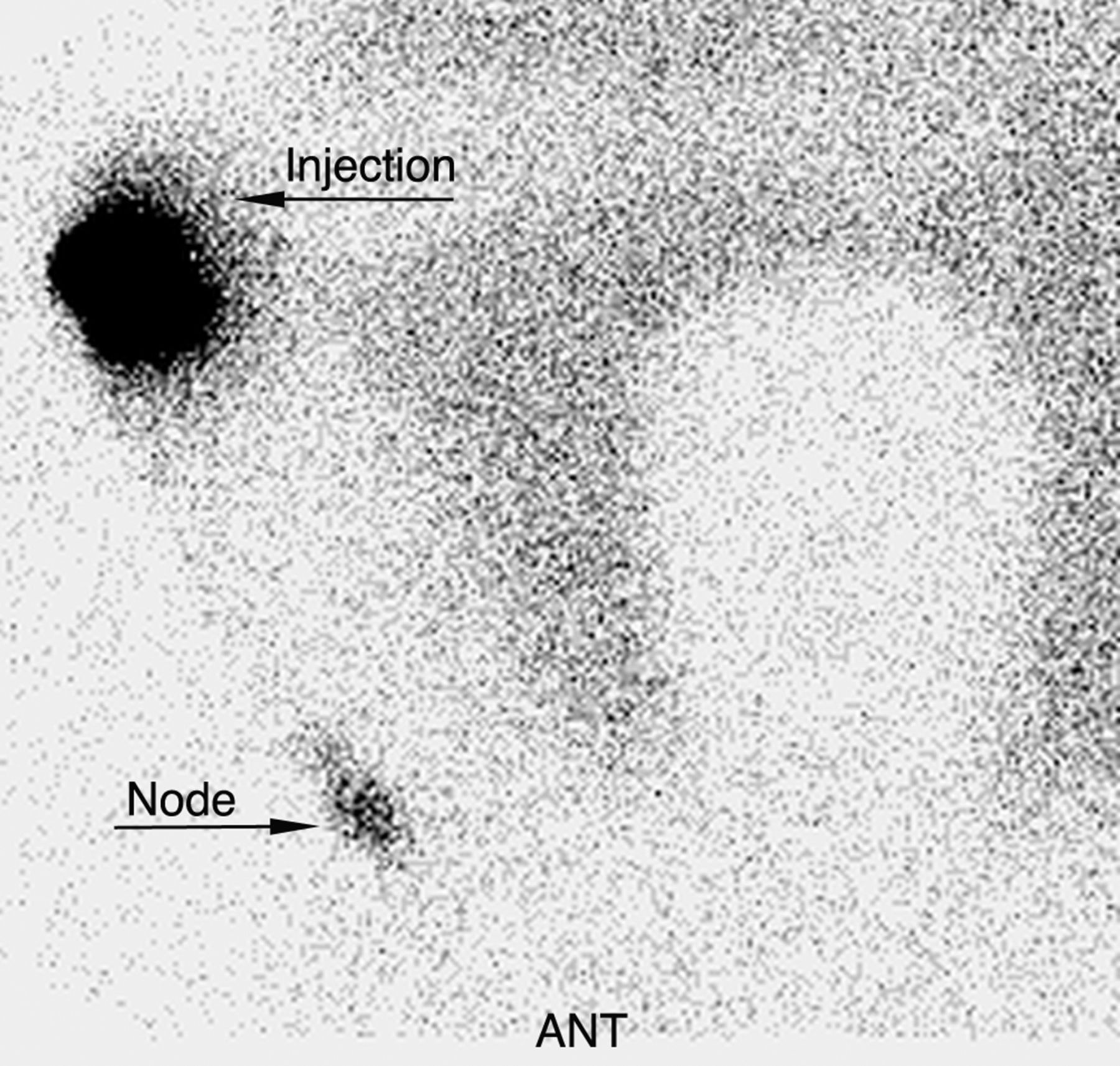
Cancer in right breast. After periareolar intradermal injection of 99mTc-tilmanocept in right upper outer quadrant, sentinel node was identified in right axilla. ANT = anterior; LAT = lateral.
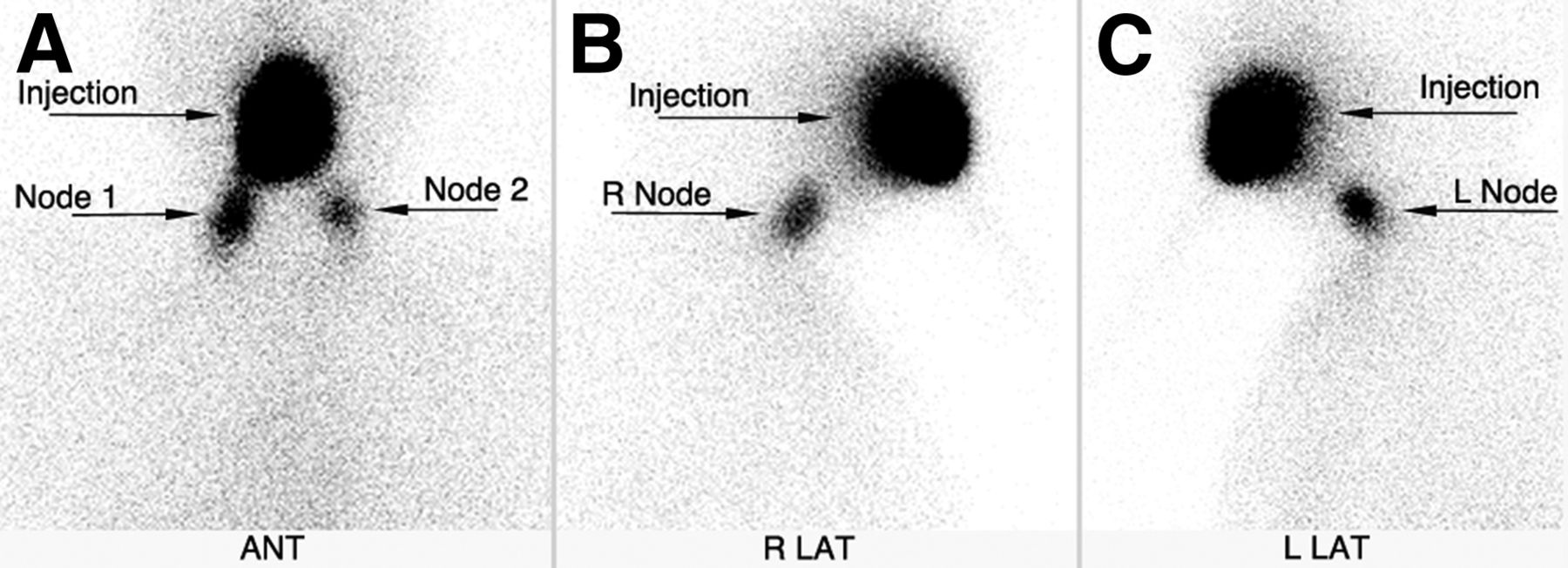
Melanoma in right arm. After intradermal injection of 99mTc-tilmanocept around lesion, sentinel node was identified in right axilla.
The radiation exposure associated with 99mTc-tilmanocept lymphatic mapping is relatively low. The estimated effective dose equivalent from an 18.5-MBq (0.5-mCi) dose of 99mTc-tilmanocept in women with breast cancer and melanoma are 0.3302 and 0.2511 mSv, respectively, and the effective dose equivalent in men with the same diagnoses is 0.296 and 0.2024 mSv, respectively (10). For comparison, the average effective dose equivalent reported with other diagnostic studies such as mammography is 0.4 mSv and that for 2-view chest radiography is 0.1 mSv (12).
99mTc-tilmanocept has no contraindications, and in clinical trials no serious adverse or hypersensitivity reactions were reported. However, there may be a risk of allergic reactions due to its chemical similarity to dextran. The most common adverse reactions included injection site irritation or pain, which occurred in less than 1% of patients. In animal studies, locally injected anesthetics have been reported to reduce lymphatic flow. Coinjection (mixture) of local anesthetics with 99mTc-tilmanocept is not recommended and may impair the lymph node mapping. A review of clinical data did not identify any differences in safety or efficacy between elderly (65–90 y old) and younger (18–65 y old) patients (10).
Preclinical Studies
The potential application of 99mTc-tilmanocept to other cancers (e.g., gastric, colon, and prostate), along with demonstration of an acceptable biodistribution, lack of toxicity, low absorbed radiation dose, and favorable pharmacokinetic properties (faster injection site clearance, rapid accumulation, and longer retention in the sentinel node), have been reported in preclinical studies. Readers are directed to the referenced articles for further details (9,13–16).
99mTc-Tilmanocept Versus 99mTc-SC
Multiple phase I–III trials and retrospective studies have demonstrated the superior performance of 99mTc-tilmanocept over filtered 99mTc-SC.
A phase I clinical trial comparing 99mTc-tilmanocept with filtered 99mTc-SC for sentinel node detection was performed on 12 patients with breast cancer using peritumoral/subdermal injections at the 3-, 6-, 9-, and 12-o’clock positions and acquisition of serial images for 180 min. Sentinel nodes, excised within 4.2–7.3 h of administration, were assayed in a dose calibrator. 99mTc-tilmanocept exhibited a significantly faster injection site clearance (P = 0.0025) and equivalent primary sentinel node uptake (P = 0.75). The mean 99mTc-tilmanocept clearance half-time was 2.72 ± 1.57 h, compared with 49.5 ± 38.5 h for filtered 99mTc-SC (17). Faster injection site clearance and equivalent sentinel node uptake were similarly demonstrated in another phase I trial also in breast cancer patients but with an intradermal injection technique. The intradermal injection, however, did not exhibit a faster clearance half-time than peritumoral/subdermal injection (18). A similar phase I trial by the same group, performed on melanoma patients, also found that 99mTc-tilmanocept demonstrated faster injection site clearance and equivalent primary sentinel node uptake when compared with filtered 99mTc-SC (7).
The efficacy of 99mTc-tilmanocept in 2-d lymphatic mapping protocols for breast cancer patients has also been proven. A study measuring injection site clearance and SLN accumulation after a single intradermal injection of 99mTc-tilmanocept and 99mTc-SC using a 2-d protocol found that 99mTc-tilmanocept cleared from the injection site significantly faster than 99mTc-SC (P < 0.001). The mean SLN uptake of 99mTc-tilmanocept was statistically equivalent to that of 99mTc-SC (P = 0.213). The extended interval provided by the 2-d protocol demonstrated that SLN accumulation of 99mTc-tilmanocept can persist for at least 24 h after administration (19). A retrospective analysis of 32 breast cancer patients also found that although the clearance rate of 99mTc-tilmanocept was faster than that of filtered 99mTc-SC, there was no significant difference between the 2 radiopharmaceuticals for the detection of radioactive SLNs in 2-d breast lymphatic mapping procedures (20).
A phase I study testing the biodistribution and safety of 99mTc-tilmanocept at different molar doses was performed on 24 breast cancer patients by Ellner et al. (21). Patients were categorized into 4 groups: 3 different molar doses of 99mTc-tilmanocept (0.2, 1.0, or 5.0 nmol) and a dose of filtered 99mTc-SC. They found that the injection site clearance of 99mTc-tilmanocept was not statistically different in a dose-dependent manner; however, dose-dependent sentinel node uptake was observed (P = 0.03). These findings also led to the selection of 1 nmol as the optimal molar dose. No clinically significant changes were seen in laboratory parameters among any of the dose levels at 4 or 24 h after injection, compared with preoperative levels. Absorbed radiation doses did not differ among the three 99mTc-tilmanocept dose levels but were lower than for filtered 99mTc-SC.
Baker et al. evaluated the technical outcomes of SLN biopsy in breast cancer patients mapped with 99mTc-tilmanocept and VBD versus filtered 99mTc-SC and VBD. They found that fewer SLNs were removed from patients mapped with 99mTc-tilmanocept plus VBD than from patients receiving filtered 99mTc-SC plus VBD (P < 0.001). Similar proportions of patients were identified with pathologic node involvement, whether mapped with 99mTc-tilmanocept or with filtered 99mTc-SC. However, in the 99mTc-tilmanocept group, a larger proportion of removed nodes were found to be positive (1.7 times greater) (22).
A prospective phase II clinical trial on 31 breast cancer and 47 cutaneous melanoma patients demonstrated the safety and efficacy of 99mTc-tilmanocept in intraoperative lymphatic mapping. Lymphoscintigraphy identified a hot spot in 94.5% of patients before surgery. Intraoperatively, at least one regional SLN was identified in 96.2% of patients. In addition to high per-patient localization rates, 99mTc-tilmanocept exhibited mapping sensitivity of 95.1% (resected tissues) and tissue specificity of 100% (lymph nodes). The overall proportion of 99mTc-tilmanocept–positive lymph nodes containing metastatic disease was 13.7%. Five procedure-related serious adverse events occurred, none of which were related to 99mTc-tilmanocept (23).
Two nonrandomized phase III trials, in which 15 centers contributed 154 patients, compared 99mTc-tilmanocept with VBD for identification of the SLN in clinically node-negative cutaneous melanoma. The primary endpoints included concordance (proportion of blue nodes detected by 99mTc-tilmanocept; 90% was the prespecified minimum concordance level) and reverse concordance (the proportion of radioactive nodes detected by VBD). Intraoperatively, 232 of 235 blue nodes were detected by 99mTc-tilmanocept, for 98.7% concordance (P < 0.001). 99mTc-tilmanocept detected 364 nodes, of which 232 were detected by VBD, for a 63.7% reverse concordance. Melanoma was identified in the SLNs of 22.1% of patients. 99mTc-tilmanocept identified more SLNs in more patients and identified more melanoma-containing nodes than VBD, with no serious adverse events attributed to 99mTc-tilmanocept (24). A similar phase III study for SLN mapping was performed on breast cancer patients. Intraoperatively, 207 of 209 nodes detected by VBD were also detected by 99mTc-tilmanocept, for a concordance rate of 99.04% (P < 0.0001). 99mTc-tilmanocept detected 320 nodes, of which 207 (64.7%, reverse concordance) were detected by VBD. Metastatic disease was identified in the SLNs of 18.2% of patients. More SLNs in more patients with a higher number of metastatic lymph nodes were identified by 99mTc-tilmanocept than by VBD (25).
99mTc-Tilmanocept Versus 99mTc-Nanocolloid Human Serum Albumin
99mTc-nanocolloid human serum albumin is a widely used radiocolloid in Europe, often in conjunction with VBD. Tokin et al. retrospectively compared 99mTc-tilmanocept with 99mTc-nanocolloid human serum albumin in breast cancer patients who underwent intraoperative lymphatic mapping. Data analysis revealed a higher localization rate (proportion of patients with at least one localized lymph node) and degree of localization (average number of localized nodes per patient relative to patient population) for 99mTc-tilmanocept than for 99mTc-nanocolloid human serum albumin (P < 0.0001) (8).
99mTc-Tilmanocept in Oral Cavity Squamous Cell Carcinoma
SLN biopsy for early-stage oral cavity cancer has decreased treatment morbidity and cost. It is gaining acceptance as an effective alternative to elective neck dissection for staging the N0 neck (26). Though several studies showing the utility of 99mTc-tilmanocept in breast carcinoma and melanoma are available, only a few studies have outlined its role in detection of SLNs in oral cavity squamous cell carcinoma. A preliminary single-institution experience within the setting of a phase III multi-institutional study, reported by Marcinow et al., demonstrated a high negative predictive value and low false-negative rate in the identification of occult nodal metastases in head and neck squamous cell carcinoma using 99mTc-tilmanocept (27). They also compared planar imaging with SPECT/CT and found that SPECT/CT identified additional SLNs in 55% of the cases, thus improving preoperative SLN localization, including delineation of SLN locations near the primary tumor. The trial was terminated early on the basis of an interim review by the Data and Safety Monitoring Committee for positive efficacy outcome and no safety concerns.
A recent multicenter, open-label, phase III trial by Agrawal et al. found a high rate of SLN identification with the use of 99mTc-tilmanocept SLN biopsy in patients with intraoral or cutaneous head and neck squamous cell carcinoma. When used with serial sectioning and immunohistochemistry, SLN biopsy with 99mTc-tilmanocept accurately predicted the pathologic status in neck nodes, with a low false-negative rate, high negative predictive value, and high overall accuracy, potentially avoiding more extensive surgery, including elective neck dissection (28).
Superior performance characteristics for 99mTc-tilmanocept in intraoperative lymphatic mapping have also been demonstrated in a cohort of 384 patients with multiple solid tumors, including breast cancer, melanoma (all sites), and head and neck squamous cell carcinoma (cutaneous and oral [tongue, floor-of-mouth, gingiva, and lip]) (29–32).
Reimbursement
For the imaging procedure, SNMMI recommends Current Procedural Terminology code 78195 (lymphatic and lymph node imaging) for all settings and payers. When 99mTc-tilmanocept is injected for lymph node mapping without imaging, the Current Procedural Terminology code to be used is 38792 (injection procedure; radioactive tracer for identification of sentinel node). Since January 1, 2014, the additional specific drug code for 99mTc-tilmanocept, diagnostic, up to 18.5 MBq (0.5 mCi), is Healthcare Common Procedure Coding System level II code A9520 (33). According to the Medicare Hospital Outpatient Prospective Payment System, the proposed 2015 rates for codes 78195, 38792, and A9520 are $363.90, $285.47, and $240, respectively (34).
CONCLUSION
Preoperative and intraoperative lymphatic mapping with 99mTc-tilmanocept, a Food and Drug Administration–approved agent based on receptor targeting, provides a novel and clinically valuable approach to complement oncologic surgery. The safety and superior efficacy profile of 99mTc-tilmanocept in comparison to the traditionally used radiotracers has been demonstrated in several preclinical and clinical studies. The main advantages include rapid injection site clearance, high sentinel node extraction, and low distal node accumulation.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
-
Published online May 8, 2015.
-
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than June 2018. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
REFERENCES
- Received for publication February 12, 2015.
- Accepted for publication April 21, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Tumor Immune Cell Targeting Chimeras (TICTACs) For Targeted Depletion of Macrophage-Associated Checkpoint Receptors
- Sentinel Lymph Node Biopsy in Breast Cancer with 99mTc-Tilmanocept: A Multicenter Study on Real-Life Use of a Novel Tracer
- 99mTc-Tilmanocept Versus 99mTc-Sulfur Colloid in Lymphoscintigraphy: Sentinel Lymph Node Identification and Patient-Reported Pain
- Use of 99mTc-Tilmanocept as a Single Agent for Sentinel Lymph Node Identification in Breast Cancer: A Retrospective Pilot Study