


Abstract
Current radiation protection recommendations do not provide clear guidelines or advice on pregnancy screening strategies for diagnostic nuclear medicine procedures. Previous studies have reported on variations in current practice for pregnancy screening before diagnostic nuclear medicine procedures. The development of consensus statements aims to provide a consistent approach and assist nuclear medicine personnel to confidently question patients about their pregnancy status. Methods: The Delphi technique was chosen for the research design. A panel consisting of 10 experienced nuclear medicine personnel from Australia and New Zealand was recruited. Panel members were provided with a summary of existing research. Consensus agreement was predefined as 80%. Questionnaires were developed and distributed to the panel members, with iterative analysis and feedback between survey rounds. Three survey rounds were conducted online using SurveyMonkey between December 2013 and June 2014. The round 1 questionnaire was developed from the results of a previous survey. It consisted of 30 questions designed to gather the opinions of the expert panel. After analysis of the round 1 responses, consensus statements were developed for round 2 and revised in round 3. Results: Consensus was achieved for 16 statements. The statements recommend using verbal questioning with patient signature, defining the age range for questioning as 12–55 y, providing advice on the use of pregnancy testing, and questioning potentially difficult groups such as teenagers. A flowchart was included for comment in round 3. Conclusion: This was the first Australian study to develop consensus statements and a flowchart to assist nuclear medicine personnel in consistently and confidently questioning patients about their pregnancy status before diagnostic procedures. Implementation of these statements into clinical practice guidelines should reduce the possibility of inadvertent fetal irradiation.
Determining the pregnancy status of a female patient before a diagnostic nuclear medicine procedure is potentially problematic. Although the risk to a fetus from the ionizing radiation is relatively small, radiation-protection documents recommend that all women of childbearing age be questioned about their pregnancy status before any procedure using ionizing radiation to reduce the possibility of fetal irradiation (1,2). James et al. (3,4) have previously shown that, in Australia and New Zealand, a variety of approaches are used by nuclear medicine personnel to question patients about their pregnancy status. The studies revealed that an ad hoc method of questioning (whether verbal or in writing) is being used. The types of questions asked, the age range questioned, and circumstances for the use of pregnancy testing varied across nuclear medicine departments. These variations in the approach used to identify women in the early stages of pregnancy may contribute to an increased number of cases of fetal irradiation, and therefore the development of a consistent approach was recommended.
Consistency in health care practice is important to ensure all individuals are provided with the same standard of quality care (5). Formal consensus research methods are increasingly used to develop statements and guidelines for a range of health practices when evidence in the literature is lacking or conflicting (6). The Delphi technique is an established method for creating consensus statements or guidelines from expert opinion when there is a lack of evidence on a topic (7,8).
The aim of this study was to gather the opinions of an expert panel of nuclear medicine personnel and develop consensus statements regarding the most appropriate methods for questioning female patients about their pregnancy status before diagnostic nuclear medicine procedures. The establishment and implementation of consensus statements into practice will ensure a more consistent approach to assist nuclear medicine personnel to confidently and accurately identify women in the early stages of pregnancy.
MATERIALS AND METHODS
Ethics approval for the study was provided by the University of Newcastle Human Research and Ethics Committee (approval number 2009-H-0270). All participants gave written informed consent.
Design
The Delphi technique was chosen to develop consensus statements on how to determine the pregnancy status of patients before diagnostic nuclear medicine testing. The technique was first described in the 1950s by the RAND Corp., and since the 1970s it has been widely used in health care to develop consensus statements and guidelines (7). The technique uses a panel of experts, selected on the basis of their expertise and experience, to explore important aspects of a topic while maintaining participant anonymity. The Delphi process involves a series of questionnaire rounds, each followed by iterative analysis and feedback. The process concludes when a predefined level of consensus is reached (6). As the Delphi does not require participants to physically meet, it can be conducted online, making it a cost-effective method to enable recruitment of participants from diverse geographic locations.
Expert Panel Members
The participants were nuclear medicine technologists, nuclear medicine physicians, and medical physicists in Australia and New Zealand who had at least 5 y of experience working in nuclear medicine. Potential participants were purposively selected from members of Special Interest Group committees of the Australian and New Zealand Society of Nuclear Medicine, the medical physicist register of the Australasian College of Physical Scientists and Engineers in Medicine, and the nuclear medicine clinical supervisor database from the School of Health Sciences at the University of Newcastle. A low response for participation was anticipated because of the ongoing nature of the Delphi method and the time commitment required for the study. Hence, a total of 35 potential participants were invited to participate in the study via email with the aim of achieving a panel of at least 10 experts. A participant information sheet and consent form was attached to the invitation email.
Survey Rounds
Panelists were asked to participate in up to 3 rounds of web-based questionnaires. All questionnaires were conducted online using SurveyMonkey. To ensure all panel members began the process with an equivalent knowledge base, each member received an email containing published articles summarizing issues surrounding the topic. The email also included a web link to the first-round online survey. The questionnaire for round 1 was developed from the results of our previous cross-sectional study (4). The round 1 questionnaire consisted of 30 questions with both closed and open responses to allow the participants to give their rationale for any answers. The questions covered a range of issues, including demographic information, method of questioning, and use of pregnancy testing. Rounds 2 and 3 provided panel members with a report on the analysis and feedback from the previous round, including quotes from participant responses and the level of agreement for each question. A series of statements was developed for each round, and panel members were asked to agree or disagree with each one. A free-text comment box was included after each statement. Consensus was predefined as achieving more than an 80% agreement on any statement. Areas lacking consensus were redeveloped according to the feedback, and panel members were given the opportunity to revise their responses. Statements achieving consensus were reiterated in the following round, and panel members asked to confirm their agreement and comment if needed.
RESULTS
Expert Panel Members
Ten people agreed to participate in the study: 8 nuclear medicine technologists, 1 medical physicist, and 1 nuclear medicine physician. There were 7 female participants. Nine participants worked in Australia and 1 in New Zealand. All participants had at least 5 y of experience working in nuclear medicine. All 10 completed round 1; however, only 9 participants completed rounds 2 and 3. Because all 10 participants were emailed the links to rounds 2 and 3 and their responses were anonymous, it is not known if the same participant was the nonresponder for both rounds.
Survey Rounds
Three survey rounds were conducted between December 2013 and June 2014. After round 1, the results of the survey, including comments from the panel members, were tabulated and used to develop 12 statements for the round 2 questionnaire. Ten of these 12 statements achieved consensus agreement in round 2 (Table 1). Areas lacking consensus in round 2 included questioning of teenage girls and women with “cultural barriers,” standard questions to ask, and use of pregnancy testing. These areas were further developed into 9 new statements for the round 3 questionnaire. In round 3, panel members were also asked to review and comment on the round 2 consensus statements. The responses and comments from round 3 resulted in 7 new statements achieving consensus and 1 statement from round 2 being revoked (Table 1). Panel members disagreed (62.5%) with asking women about hysterectomy and commented that asking about hysterectomy was not necessary if date of last menstrual period (LMP) was asked first, as this would “prompt them to say that they have had a hysterectomy.”
Final Consensus Statements from Rounds 2 and 3
Consensus Statements
All panel members agreed that the development of guidelines for pregnancy screening before diagnostic nuclear medicine procedures is needed to provide a consistent approach. Verbal questioning was agreed to be the most appropriate method before all diagnostic procedures, regardless of the potential radiation risk to the fetus. However, the patient should be required to provide her signature to document that the procedure and risks had been explained and to verify her pregnancy status. All panel members agreed that standard questions should include date of LMP. Childbearing age range was defined as 12–55 y.
For patients with cognitive impairment, the caregiver, medical records, or medical personnel should be consulted to determine the possibility of pregnancy and whether a pregnancy test is required. An interpreter should be used to question women with language barriers. The phrase “under normal circumstances” was included in these 2 statements to allow for flexibility and individual patient situations. Teenagers aged 12–17 y should first be asked if they have started menstruation and, if the answer is yes, then questioned about pregnancy. Therefore, if possible, and under normal circumstances, teenagers should be questioned away from accompanying parents or other adults. The phrase “culturally and linguistically diverse” should be used to describe women from varying religious, spiritual, racial or ethnic backgrounds and where possible, under normal circumstances, they should be questioned by female personnel.
All panel members agreed that pregnancy testing should be used whenever there is any uncertainty about the patient’s pregnancy status and that, if available in a reasonable time, serum human chorionic gonadotropin (HCG) testing should be used. If urine HCG testing is used before the date of missed menses and the result is negative, the procedure should be postponed until menstruation begins. Retesting with the serum HCG test was also provided as an option, but this statement achieved only 75% agreement.
Flowchart
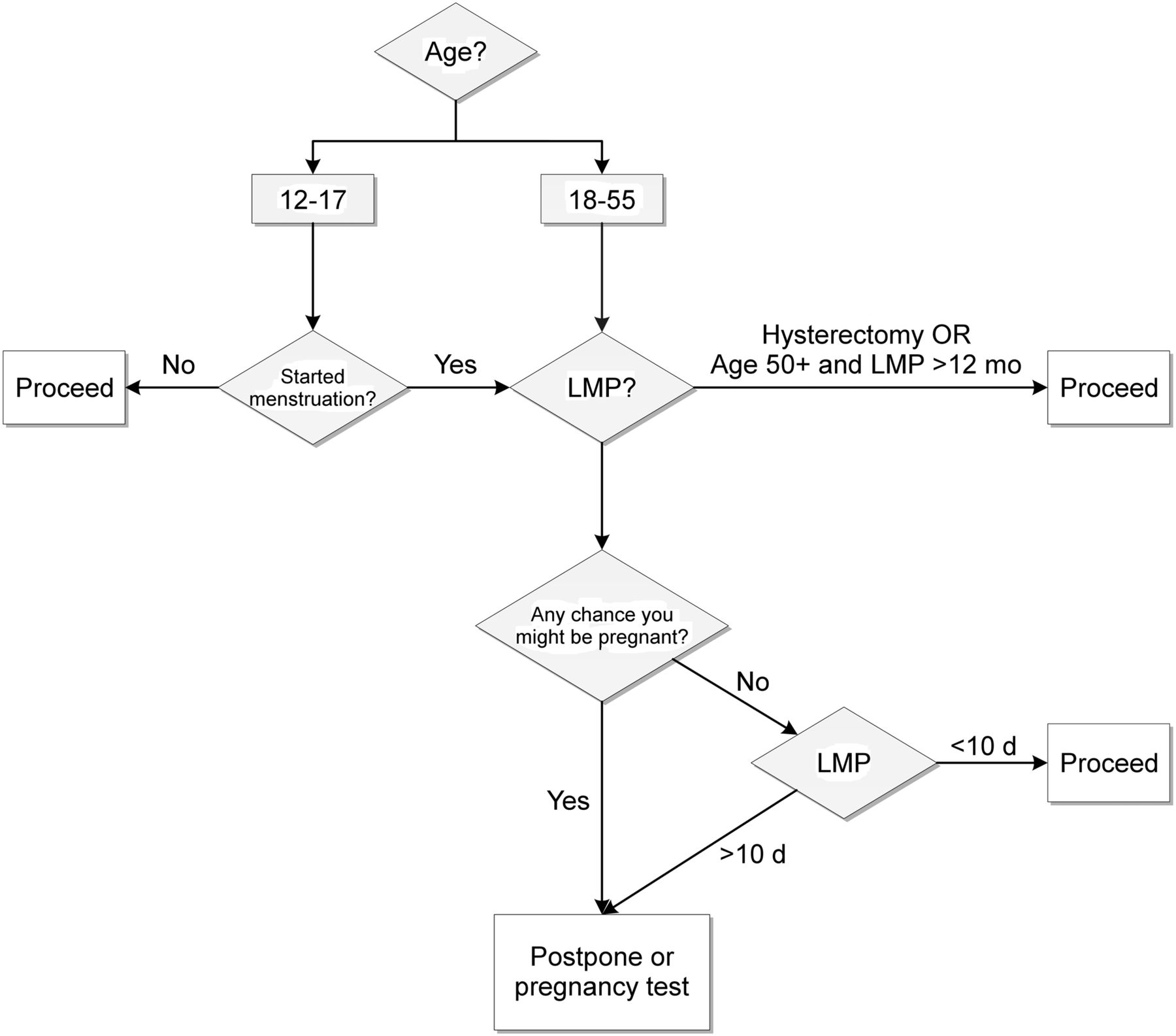
In round 3, panel members were provided with a flowchart that could be used by nuclear medicine personnel to assist in questioning women about their pregnancy status. The panel members commented that the flowchart would be “helpful” and was “a great idea” to support any guidelines and to be used as a “quick reference guide.” The flowchart questions initially separated women into 3 age groups: 12–17 y, 18–49 y, and 50–55 y. However, the 2 older age groups were combined in the final version. Questions in the initial flowchart included whether menstruation had started (12–17 y only), whether the patient had undergone hysterectomy, the date of LMP, whether the patient was sexually active, and whether the patient thought there was any chance she might be pregnant. Panel members made comments and suggested changes for the flowchart. The question about hysterectomy was considered unnecessary as the information is usually provided when asking about date of LMP. Therefore, the first question for patients aged 18–55 y was changed to date of LMP. Questions about sexual activity were also considered unnecessary and removed. The flowchart was revised to reflect this feedback (Fig. 1).
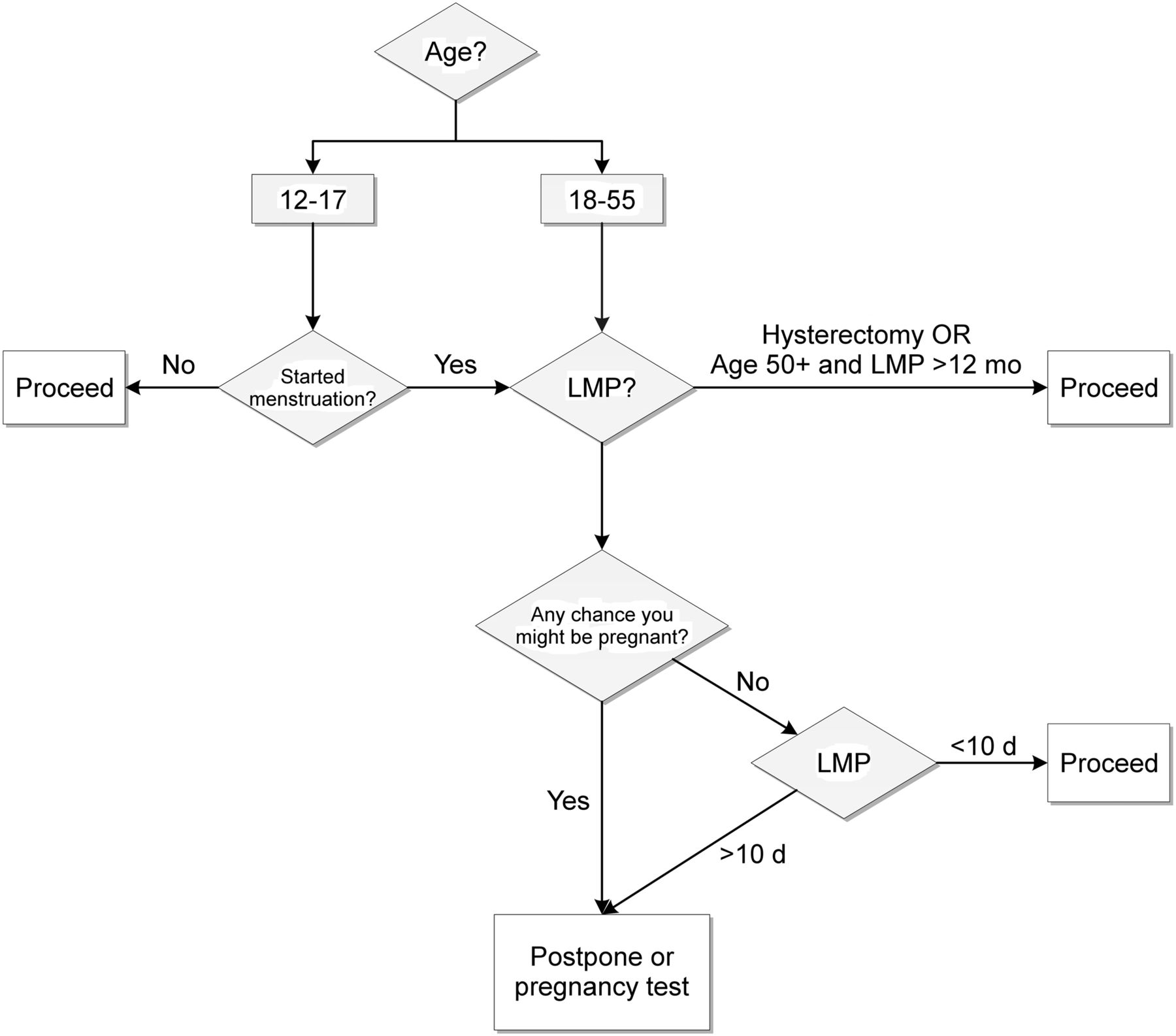
Final flowchart.
DISCUSSION
National and international radiation protection guidelines recognize the increased radiosensitivity of fetal tissue (1,2,9,10). They recommend that all female patients of childbearing age be questioned about their pregnancy status before any procedure using ionizing radiation to avoid fetal irradiation. However, the radiation protection guidelines do not provide clear instructions on how to question the patient or which patients to question. The age range for questioning has not previously been defined and there is no advice on questioning potentially difficult patient groups, such as teenagers. This study has developed 16 consensus statements to assist nuclear medicine personnel in Australia and New Zealand in confidently questioning patients and how to accurately assess pregnancy status.
Age Range
The consensus statements developed in this study define the age range for questioning as 12–55 y. There are a very small number of cases of individuals under the age of 12 y or over 55 y becoming pregnant. Australian birth statistics for 2012 show the total number of births at 309,582, with 405 (0.13%) from mothers aged 15 and under, and only 45 (0.01%) from mothers 50 y and over (Table 2) (11). These numbers include only the number of live births, not the number of miscarriages or induced abortions. Medicare Australia statistics for item 35643, “Evacuation of the Contents of the Gravid Uterus by Curettage or Suction Curettage,” show that in 2012 there were over 61,500 terminations performed in Australia, with 7,145 of these performed in women aged 19 y or less and 15,020 in women 35 y or more. The actual number of induced abortions performed is difficult to calculate because Medicare data do not include information on patients admitted to the hospital and because it is estimated that approximately 15% of private patients do not claim a Medicare benefit (12). These factors, and the aggregation of data for ages 15 y and under, make it difficult to calculate the number of pregnancies in very young teenage girls. However, assuming a worst-case scenario in which all of the 7,145 terminations in the group 19 y old or less were conducted on teenagers under the age of 15 y, the estimated number of pregnancies in girls under 15 y old accounts for less than 2.5% of all pregnancies.
Births and Age of Mother: Australia 2012 (11)
Potentially Difficult Patient Groups
Certain groups of patients, such as teenagers, women with cognitive impairment, and women with language or cultural barriers, have been identified as potentially problematic to question about their pregnancy status (4). When teenage girls are accompanied by an adult relative, they may be reluctant to provide truthful answers to questions about pregnancy for fear of embarrassment or recrimination (13). Removing the girl to another area under the guise of weighing her provides an opportunity to ask the relevant questions in privacy. This strategy may raise issues about the legality of questioning a minor without a parent or guardian present. The age of consent for medical procedures and treatment varies depending on the country and state. However, in Australia, if the girl is deemed “Gillick-competent,” she is entitled to the same confidentiality for medical information as an adult. A Gillick-competent or “mature minor” child is deemed to be old enough, or mature enough, to make her own decisions and understand the issues and consequences regarding medical treatment (4,13,14).
In round 2 of the Delphi study, participants commented on the use of the phrase “cultural barriers” as being “too nonspecific.” The Multicultural Health curriculum statement within The RACGP Curriculum for Australian General Practice (15) uses the phrase “culturally and linguistically diverse” to define groups and individuals who differ according to religion and spirituality, racial backgrounds, and ethnicity as well as language. They suggest that the phrase “culturally and linguistically diverse background” can be used to reflect intergenerational and contextual issues, not only migrant experience. This phrase was agreed on to replace “cultural barriers” by 8 of the 9 participants in round 3 of the Delphi study.
Pregnancy Testing
In the early stages of pregnancy, especially before the date of missed menses, a serum HCG test is the most accurate method to determine pregnancy. Although the minimum detection limits for urine HCG pregnancy tests have decreased over the past 20 y to 10–20 IU/L, their performance in the lower range of HCG concentration is poor and false-negative results are common when the test is used before the date of missed menses (16–18). These false-negative results may be due to user error, urine sample dilution, variations in menstrual cycle duration and calculation of the date of missed menses, and variations in the timing of implantation and therefore the concentration of HCG in urine (16–18).
A systematic review published in 2013 reported on the accuracy of pregnancy checklists to rule out pregnancy (19). The checklists were based on criteria defined by the World Health Organization’s Selected Practice Recommendations for Contraceptive Use (20,21). The review reported on 3 studies (2,650 women) of diagnostic accuracy assessing the validity of a pregnancy checklist when compared with a urine pregnancy test. The checklists were able to confidently rule out pregnancy in women who are not pregnant, as there was a consistent 99%–100% negative predictive value across the included studies. Several other studies have reported on the ability of women to self-assess their pregnancy status (22,23). These studies also report excellent negative predictive value (99% and 100%) for questioning a woman if she “might be” pregnant.
Performing serum pregnancy tests on all female patients before diagnostic nuclear medicine procedures would be costly, time-consuming, and unnecessary. The consensus guidelines and associated flowchart provide a simple, consistent process for pregnancy screening that should identify most pregnancies and limit the number of pregnancy tests required. The current study demonstrates ongoing support for the development of consensus guidelines and reinforces the results from our previous studies (3,4,24).
CONCLUSION
The consensus statements and flowchart developed in this study cover a range of issues that have not previously been discussed in radiation protection documentation for diagnostic nuclear medicine procedures. They provide a clear and consistent approach for nuclear medicine personnel to follow when questioning patients about their pregnancy status. The statements recommend the use of verbal questioning with documentation via the patient signature, define the age range to question, provide strategies for teenagers and other potentially difficult groups, and provide advice on the use of pregnancy testing.
In future research, the results from this study will be used as a framework for the creation of best-practice guidelines for pregnancy screening before diagnostic nuclear medicine procedures. Implementation of the guidelines into clinical practice will provide advice and a consistent approach for questioning patients, thus helping nuclear medicine personnel to confidently and accurately determine pregnancy status and reduce the possibility of inadvertent fetal irradiation.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 22, 2015.
REFERENCES
- Received for publication September 8, 2014.
- Accepted for publication November 13, 2014.





{kind=link}