


Abstract
The purpose of this study was to determine whether certain factors in the preparation and use of 99mTc-sulfur colloid affected the number of sentinel lymph nodes (SLNs) detected during SLN mapping and during intraoperative SLN identification. The factors that were investigated included the use of a dry heat block versus a hot water bath to heat the 99mTc-sulfur colloid bulk vial, amount of 99mTcOH4− added to form the sulfur colloid particles, time between the unit dose calibration and the injection of the dose, and breast quadrant in which the injection occurred. Methods: Data were collected retrospectively and quantitatively analyzed from images and reports of 488 patients with breast cancer who had undergone SLN mapping and intraoperative SLN identification from January 1, 2008, to June 30, 2011, inclusive. The dependent variables assessed were the number of SLNs visualized during lymphoscintigraphy, number of radioactive SLNs removed during surgery, and total number of lymph nodes removed intraoperatively. Results: There was no significant difference in outcomes when comparing the amount of 99mTcOH4− added during the preparation process to form the sulfur colloid particles, time between the unit dose calibration time and the time that the unit doses were injected, or location in the breast tissue in which the unit dose was administered. Initially, there were observed significant differences in outcomes when the heating methods used to prepare the 99mTc-sulfur colloid were compared. When the increased number of patients who were administered a calibrated unit dose activity of 74 MBq in the group using a dry heat block preparation method was taken into account, however, the findings were not significant. Conclusion: The use of a dry heat block versus a hot water bath to heat the 99mTc-sulfur colloid bulk vial, amount of 99mTcOH4− added to form sulfur colloid particles, time between the unit dose calibration and the injection of the dose, and breast quadrant in which the injection occurred do not affect the number of SLNs detected during SLN mapping and during intraoperative SLN identification.
Lymph node mapping (lymphoscintigraphy) is a common nuclear medicine imaging procedure for patients with breast cancer who are scheduled for a sentinel lymph node (SLN) biopsy. Patients are given an injection of a 99mTc-labeled colloid into their breast tissue near the tumor site. 99mTc-labeled colloid particles enter the lymphatic channels and are carried by lymph flow to lymph nodes draining the tumor. The SLN is the first lymph node to receive lymphatic drainage from a tumor (1). Hence, a negative tumor status of the SLN should accurately predict a negative histopathologic status of downstream nodes in the same lymphatic basin (2).
Although the aim of nuclear medicine lymphoscintigraphy is normally to identify one or more SLNs for biopsy, it has been noticed that 4–8 lymph nodes have frequently been identified during nuclear medicine lymph node imaging at Duke University Medical Center. Identifying a higher number of SLNs leads to more invasive surgery. Cheng et al. state that “…indiscriminate removal of axillary nodes may cause tissue damage similar to that in axillary lymph node dissection” (3). Complications that may result from unnecessary SLN removal or axillary lymph node dissection are an increased risk of lymphedema, axillary nerve damage, decrease in shoulder function, pain, and infection (4–6).
In the United States, 99mTc-sulfur colloid is the only product currently available for lymph node mapping and SLN detection approved by the Food and Drug Administration (3). Unfiltered 99mTc-sulfur colloid was used in this retrospective study. The particle size of unfiltered 99mTc-sulfur colloid ranges from 15 to 5,000 nm, depending on the preparation method, with the average size ranging from 305 to 340 nm (3). A 1996 study of sulfur colloid particle stability by Eshima et al. established that there were no significant changes in particle size over a 6-h period after the reconstitution and labeling of particles. However, it has been demonstrated that sulfur colloid kits that had a prolonged heating time of 10 min, compared with a reduced heating time of 3 min, showed an increase in the percentage of larger sulfur colloid particles formed (7). Larger sulfur colloid particles demonstrate a slower transit time in the lymphatic system, which may minimize the visualization of non-SLNs. Another advantage of larger 99mTc-sulfur colloid particles is longer tracer retention within the SLN, allowing for intraoperative detection the following day (3). However, particles larger than about 200 nm will be retained at the site of injection because they are too large to readily flow through lymphatic channels (8).
The Radiopharmacy at our institution has used 2 different methods, a boiling water bath and a dry heat block set at 100°C to heat the sulfur colloid kit for 5 min. In the boiling water bath, the kit vial may be brought to maximal temperature (approaching 100°C) at a faster rate and is at that temperature for a longer period of time because the boiling water is in intimate contact with the vial surface and covers a larger proportion of the vial’s volume than the dry heat block. Using the results of the study by Eshima et al., we speculated that the kits heated in the hot water bath, when compared with the use of the dry heat block, may form larger sulfur colloid particles (7).
The lymph node uptake of the radiopharmaceutical is not solely based on the colloidal particle size but may be also affected by the number of sulfur colloid particles that are injected (2). An autoradiograph of 99mTc-sulfur colloid estimated that 5.5 × 108 particles per milliliter are formed during preparation. However, using this method of counting, only particles larger than about 200 nm can be visualized (9). The higher the number of particles that are draining to a lymph node, the sooner the lymph node becomes saturated, allowing colloidal particles to progress to the next lymph node within the lymphatic chain (2). A 99mTc-sulfur colloid bulk vial that is compounded with a lower amount of 99mTcOH4−, compared with a vial that is compounded with a higher amount, will have a greater ratio of sulfur colloid particles to 99mTc activity, assuming all other preparation factors remain constant. Thus, for equal amounts of administered dose activity, a lymphoscintigraphy dose that was drawn from a 99mTc-sulfur colloid bulk vial with a high ratio of sulfur colloid particles to 99mTc activity may result in an increased number of SLNs localized because of the higher number of sulfur colloid particles.
The objective of this study was to analyze factors that could increase the number of lymph nodes that accumulate the 99mTc-sulfur colloid, thus leading to an increase in unnecessary lymph node removal, which in turn may lead to increased morbidity rates (4). The study considered 4 aspects related to the preparation and use of the 99mTc-sulfur colloid, namely, the use of a heating block versus a hot water bath to prepare the 99mTc-sulfur colloid, amount of 99mTcOH4− used in forming the sulfur colloid particles, time between the preparation of the 99mTc-sulfur colloid unit dose and the injection of that dose, and breast quadrant in which the injection occurred.
MATERIALS AND METHODS
Preparation Protocol
The Radiopharmacy at Duke University Medical Center uses a kit manufactured by Pharmalucence for the preparation of the 99mTc-sulfur colloid injection administered during lymph node mapping studies. This kit is prepared following the radiation safety and aseptic procedures detailed in the package insert. The first kit preparation step is to add 99mTcOH4− to the sulfur colloid reaction vial (10). The eluate from 99Mo/99mTc generators used for labeling sulfur colloid kits is consistently less than 24 h old. The activity of the 99mTcOH4− added varies daily depending on the amount of the radioisotope available and the time scheduled for the patient’s appointment with the nuclear medicine department. Because the added 99mTcOH4− activity varies and the same type of preparation kit is used each time, the ratio of 99mTc activity to sulfur colloid particles is not constant. When a higher amount of activity of 99mTcOH4− is added, there are fewer sulfur colloid particles per megabecquerel of 99mTc in the preparation vial. Similarly, when a lower amount of activity of 99mTcOH4− is added, there are more sulfur colloid particles per megabecquerel of 99mTc.
Another step in the 99mTc-sulfur colloid preparation process is to heat the reaction vial in a vigorously boiling water bath (which, depending on altitude, approaches a temperature of 100°C (10)). For this step, the Radiopharmacy has used 2 different methods to heat the colloid kit. One method places the reaction vial into a boiling water bath for 5 min. The other method places the reaction vial into a dry heat block set at 100°C for 5 min. Originally, the boiling water bath heating method was used exclusively. However, the dry heat block method was subsequently adopted to better comply with USP <797> sterile compounding standards when the Radiopharmacy moved to a new site in the Medical Center starting May 12, 2009. During this time, it was noted that more SLNs were being visualized and localized than had been in the past. Hence, the Radiopharmacy switched back to using the boiling water bath heating method for 99mTc-sulfur colloid preparation on December 27, 2010.
The radiochemical purity for the 99mTc-sulfur colloid bulk vials was more than 95%. Each 99mTc-sulfur colloid bulk vial provides patient doses that are diluted with sterile sodium chloride in an appropriate number of syringes and vials to bring the amount of radioactivity to within the recommended dose and volume range for the patient’s scheduled study. The time that a patient’s unit dose is made from the bulk vial depends on the scheduled time of the lymph node mapping study; thus, the time between the unit dose preparation and the actual injection time varies with each case.
Injection and Imaging Protocol
The 99mTc-sulfur colloid used at our institution for SLN localization is unfiltered and administered in a combined subcutaneous and intradermal technique into the tissue of the breast. A total volume of approximately 0.4 mL in an insulin syringe with a 28-gauge needle is used for each injection site. The facility’s standard protocol for the administered dose activity for lymph gland imaging for patients with a diagnosis of breast cancer varies depending on their date of surgery. This variance is due to the half-life of 99mTc. For example, when the patient is scheduled for lymphoscintigraphy and surgery on the same day as the injection, they receive a 99mTc-sulfur colloid dose of 18.5 MBq (0.5 mCi) ± 10%. On the other hand, patients who have their surgery scheduled for the day after the lymphoscintigraphy injection receive a 99mTc-sulfur colloid dose of 74 MBq (2.0 mCi) ± 10%. Patients with bilateral breast cancer receive a 99mTc-sulfur colloid injection at each cancer site specified by the surgeon.
Immediately after the 99mTc-sulfur colloid injection, planar images are acquired for 3 min in the anterior, anterior–oblique, and lateral projections. Additional images are acquired if needed for identification of the SLNs between an hour and 24 h after the 99mTc-sulfur colloid injection. The delayed images are acquired in the same projections as the initial images. The planar images are acquired for 3 min each, and the transmission images using a 57Co sheet source are acquired for 1 min each to help localize the SLNs by creating a silhouette of the patient’s body.
The location of the lymph nodes that are visualized on the last images obtained are marked externally on the patient’s skin using a permanent marker and directed by a hand-held γ-detecting intraoperative probe. For this marking, patients are positioned in a manner similar to their positioning on the operating room table. A handheld γ-detecting intraoperative probe is used by the surgeon during the operation to assist in identifying the surgical incision site and the lymph nodes visualized during the lymph node mapping. In addition, the surgeon commonly injects a blue dye deeply into the patient’s breast tissue before the operation to aid in locating lymphatics and lymph nodes that drain the breast tumor site. At the time of surgery, the nuclear medicine technologist completes a form noting the number of lymph nodes removed, radioactive counts of each lymph node removed, and whether each lymph node removed contained blue dye.
Research Method
The Duke University Health System Institutional Review Board approved a waiver of consent and Health Insurance Portability and Accountability Act authorization for this retrospective study. The data were collected from previously acquired images and reports that fully met the criteria described below. Data were collected from the lymph node mapping images and the subsequent intraoperative lymph node identification reports that used 99mTc-sulfur colloid injections from a bulk vial that was prepared with 2,960 MBq (80 mCi) ± 10% (2,664–3,256 MBq) of 99mTcOH4− or with 6,660 MBq (180 mCi) ± 10% (5,994–7,326 MBq) of 99mTcOH4−. The study indication for the lymph node imaging for this retrospective analysis was breast cancer. For patients undergoing bilateral lymphoscintigraphy and bilateral intraoperative lymph node identification on the same day, only the left breast was considered. Further, the study must have been performed between January 1, 2008, and June 30, 2011, inclusive, at Duke University Medical Center to be considered for inclusion in the study’s data.
The activity of 99mTcOH4− that was added to the sulfur colloid bulk vial and the heating method that was used to prepare the 99mTc-sulfur colloid bulk vial were determined from examining the Radiopharmacy’s preparation records. Further, the time and activity for which the 99mTc-sulfur colloid unit dose was calibrated were determined from the Radiopharmacy’s preparation records. From the lymphoscintigraphy report on the picture archiving and communication system (PACS), the breast quadrant of the injection site and the time that the patient was injected with the 99mTc-sulfur colloid dose were determined. The last set of lymph gland mapping images on the PACS that was acquired before surgery was used by a CNMT masked to the patient data to quantify the number of visible SLNs and to determine the time that the final lymph node mapping images were acquired. The intraoperative SLN identification reports on the PACS were used to determine the number of radioactive SLNs and the total number of lymph nodes that were removed during surgery.
Four hundred eighty-eight patients met criteria to be included in this research study. Four factors from these data were analyzed to determine whether any factor led to significant outcomes. The factors were the ratio of the amount of radioactivity to the number of sulfur colloid particles, heating method used, amount of time between the 99mTc-sulfur colloid unit dose calibration time and the injection of that dose, and location of the injection within the breast tissue. The outcomes are defined as number of SLNs visualized on the last set of lymph gland mapping images that were acquired before surgery; number of radioactive SLNs removed intraoperatively, which includes hot and blue lymph nodes and only hot lymph nodes; and total number of lymph nodes removed during surgery, which includes hot and blue lymph nodes, only hot lymph nodes, only blue lymph nodes, and only palpable lymph nodes.
The collected data were organized in groups according to the preparation method used for the bulk vials of 99mTc-sulfur colloid (Table 1). A comparison between the groups was performed using 1-way ANOVA in Tables 2–4 (11). Group A is the standard for these comparisons. The outcome effects for group B and group C were subtracted from group A. A P value of less than 0.05 implies a significant outcome result. Additionally, the frequency of 18.5- and 74-MBq 99mTc-sulfur colloid unit doses was calculated and presented in Table 3.
Heating Method and Amount of Radioactivity for Each Group
ANOVA for Number of SLNs Visualized in Each Group
Frequency Distribution of Unit Dose for Each Group
Multivariable Regression for Number of SLNs Visualized for Each Coefficient
Multivariable Regression for Number of Radioactive SLNs Removed for Each Coefficient
Further in Tables 4–6, the joint effect of all factors together was examined using a multivariable regression (11). The baseline consisted of an 18.5-MBq 99mTc-sulfur colloid unit dose withdrawn from a bulk vial prepared with the dry heat block heating method administered into the inner mid zone of the breast tissue exactly at the time of unit dose calibration. The outcomes of the baseline were compared with the outcomes of the other coefficients. A log(Y + 1) transform was used on the response Y (counts) to achieve approximate normality for residuals. The homoscedasticity of residuals was checked by plotting against fitted values. A cutoff of ±3 was used for standardized residuals to identify outliers. Influential observations were identified by Cook’s distance (12). Because only comparisons between individual treatments and baseline—that is, canonically estimated effects—are presented in this paper, it was not necessary to adjust P values for multiple comparisons. Again, a P value of less than 0.05 implies a significant outcome result.
Multivariable Regression for Number of Lymph Nodes Removed for Each Coefficient
RESULTS
The average number of SLNs visualized in group B appears to be higher than those in groups A and C (Fig. 1)—a result that is confirmed by the ANOVA analysis (Table 2). Group A had an average of 2.4 SLNs visualized per patient. When group B was compared with the baseline group A (group B – group A), there was a statistically significant increase of approximately 0.8 SLNs visualized, with a significant P value of 0.003. A similar pattern was found for the number of radioactive SLNs removed and the number of lymph nodes removed, with the comparison between group B and group A being statistically significant.

Distribution of sentinel nodes by group.
To establish whether the amount of 99mTcOH4− added to the bulk vial to form the sulfur colloid particles altered the outcomes, group A was compared with group C (group C – group A). Again, Table 2 shows an effect of approximately 2.4 SLNs visualized in group A. When group C was compared with group A, there was an insignificant decrease of approximately −0.2 SLNs visualized, with an insignificant P value of approximately 0.6. The results were equivalent for the number of radioactive SLNs removed and the number of lymph nodes removed. Hence, there was no significant difference when the water bath at 2,960 MBq ± 10% was compared with the water bath at 6,660 MBq ± 10%. Similar conclusions were obtained when the same model was fitted as a log linear model with Poisson response.
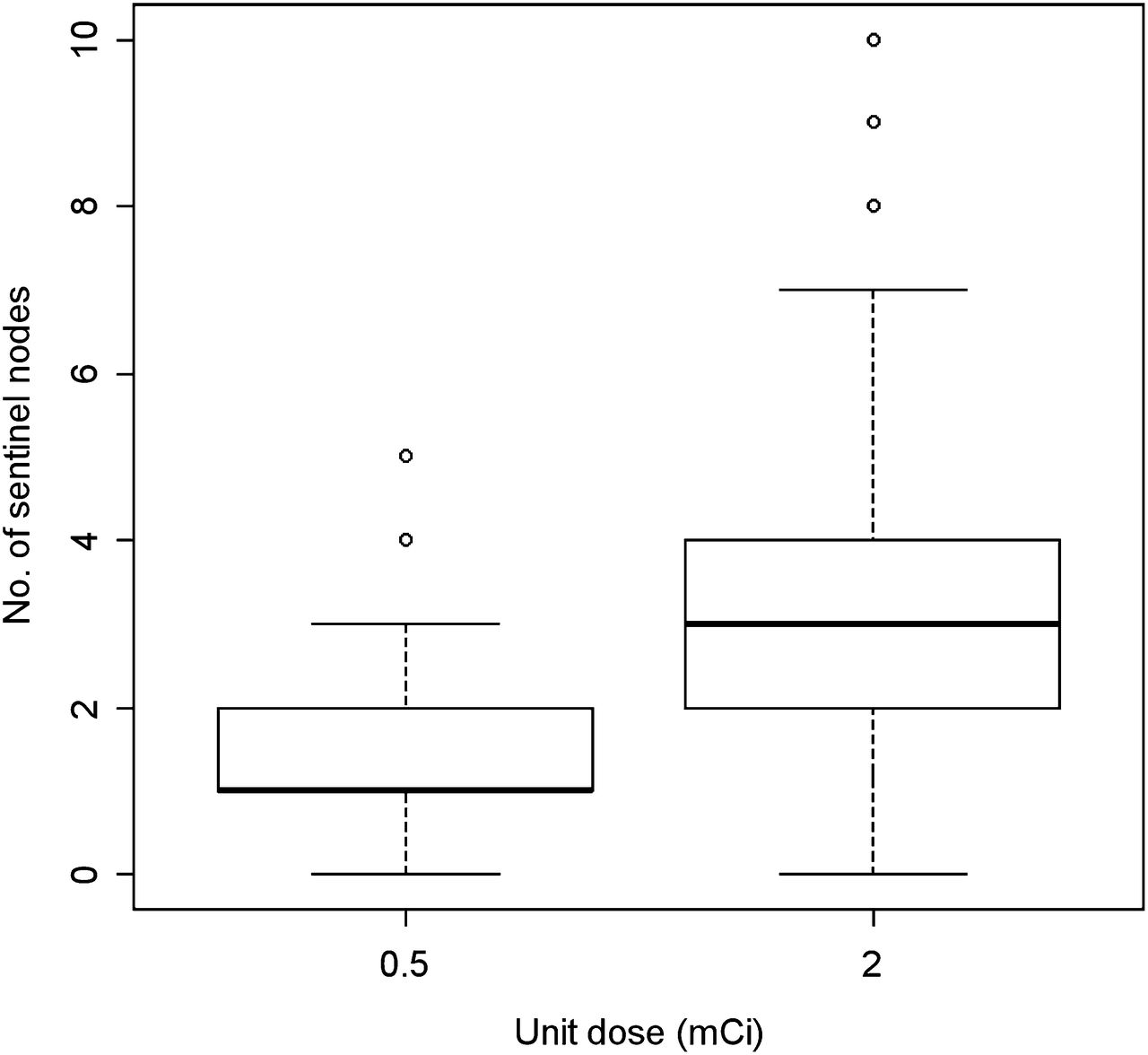
To see if the observed outcome differences between the 2 heating methods used could be explained by other factors, the joint distribution of heating method and unit dose was examined. As seen in Table 3, there are approximately equal numbers of either heating method using a calibrated unit dose of 18.5 MBq. However, there is a preponderance of the dry heat block method with a calibrated unit dose of 74 MBq. When the heating method used during preparation was compared, group A versus group B, group B had over 6 times more 74-MBq 99mTc-sulfur colloid unit doses than group A. The average number of SLNs visualized at a higher unit dose was substantially higher than at a lower unit dose (Fig. 2), suggesting that some of the apparent differences due to the heating method used could actually be due to a higher unit dose.

Distribution of sentinel nodes by unit dose.
When a multivariable regression model was fitted for the outcomes, it was noticed that the heating method did not cause a significant difference for any of the outcomes (Tables 4–6). Instead, the unit dose was a highly significant factor for 2 of the outcomes—a P value of less than 0.0001 for the number of SLNs visualized and a P value of 0.01 for the number of lymph nodes removed. The unit dose approached significance, with a P value of 0.07 for the number of radioactive SLNs removed.
Additionally in the multivariable regression model, the significance of the time difference between the 99mTc-sulfur colloid unit dose calibration time and the time that the unit doses were injected as well as the significance of the breast tissue area in which the unit dose was administered were assessed. When the time difference between the unit dose calibration and the time that the unit doses were injected was compared, there was no significant difference in the resulting outcomes (Tables 4–6). Similarly, there was no consistent zone where the outcomes were significantly different when the locations in the breast tissue in which the unit dose was administered were compared (Tables 4–6).
We examined pairwise interactions between covariates and the presence of a possible nonlinear trend by adding a quadratic term in time. None of these terms was significant, and only the unit dose by heating method term is reported for brevity. None of the fitted models exhibited heteroscedasticity in residuals. The distribution of residuals was found to be approximately normal. Sensitivity analysis was performed by excluding outliers and influential observations and refitting the models. Estimated coefficients and their significance were not substantially changed from those reported.
DISCUSSION
The preparation and use factors of 99mTc-sulfur colloid that were analyzed did not affect the outcomes of lymphoscintigraphy. When ANOVA was used to compare the groups in Table 1, it appeared that the use of the dry heat block heating method produced an increase in the number of SLNs visualized and removed intraoperatively. However, after the data were fitted with a multivariable regression model, the significance of the outcomes was due to the increased number of 74-MBq 99mTc-sulfur colloid unit doses used in group B, compared with group A. Once the effect of the unit dose was adjusted, there was no residual effect due to the heating method used.
A considerable finding is that the heating method used during preparation of the 99mTc-sulfur colloid bulk vials did not change the number of SLNs visualized or localized intraoperatively. The increase in the number of SLNs noticed during the period of dry heat block use may have been due to other factors, such as the patient’s age, patient’s body weight, size of the breast tumor, or presence of metastases in the SLNs (3,13). Nevertheless, it would be interesting to explore whether the integrated temperature–time of fluid within a vial of 99mTc-sulfur colloid varies between the boiling water bath and dry heat block heating methods at 100°C for 5 min.
Comparing the different amounts of 99mTcOH4− added to the bulk sulfur colloid vial during preparation did not significantly alter the number of lymph nodes visualized or removed during surgery. Not finding significant outcomes from the preparation factors investigated is an important finding for nuclear medicine. For instance, during radioisotope shortages a smaller activity of 99mTcOH4− may have to be added to the bulk sulfur colloid vial. The results of this study showed that outcomes did not significantly change when atypical amounts of 99mTcOH4− were added during the preparation of 99mTc-sulfur colloid.
It is an interesting finding that the significant outcomes that resulted in comparing the boiling water bath with the dry heat block heating methods during the preparation of 99mTc-sulfur colloid bulk vials were actually due to the increase in number of patients included in the research study who were administered a 74-MBq 99mTc-sulfur colloid unit dose. This was not a factor that was being investigated initially. The fact is that more patients undergo lymphoscintigraphy the day before surgery than the day of surgery at Duke University Medical Center. It happened by coincidence that more 74-MBq 99mTc-sulfur colloid unit doses were involved because it was not part of the data collection process.
Nonetheless, this study demonstrated that an increased number of SLNs were detected during lymphoscintigraphy and intraoperatively in patients who received a 74-MBq calibrated unit dose of 99mTc-sulfur colloid the day before their scheduled surgery. A study by Gray et al. established similar results. They found that administration of 74 MBq of 99mTc-sulfur colloid on the day before the operation resulted in a mean of 1.6 hot and blue SLNs identified intraoperatively, whereas administration of 18.5 MBq of 99mTc-sulfur colloid on the day of surgery resulted in a mean of 1.1 hot and blue SLNs identified intraoperatively (14).
Supplemental research needs to be performed to determine whether the results of this study are due to the actual use of 74-MBq 99mTc-sulfur colloid unit doses or solely due to the increased number of 74-MBq 99mTc-sulfur colloid unit doses included in the groups. If a significant outcome is produced when comparing the use of 74- with 18.5-MBq unit doses of 99mTc-sulfur colloid, it could be due to time differences between the administration of the dose and time of the latest lymph node mapping image or the time of surgery. In general at Duke University Medical Center, the time frame between the administration of a 74-MBq unit dose of 99mTc-sulfur colloid and last lymph node mapping image before surgery may range from 3 to 29 h. For patients receiving a 74-MBq 99mTc-sulfur colloid unit dose, the time between the administration of the 99mTc-sulfur colloid unit dose and the time of the patient’s surgery may range between 18 and 34 h at Duke University Medical Center.
Prior research has shown that there are fewer radioactive SLNs that are removed if more than 12 h have elapsed between 99mTc-sulfur colloid administration and SLN biopsy (3). On the basis of this finding, patients who are administered a 74-MBq unit dose of 99mTc-sulfur colloid during lymphoscintigraphy should have fewer SLNs visualized and intraoperatively removed.
Additionally, if significantly different outcomes are truly produced when comparing the use of 74- with 18.5-MBq unit doses of 99mTc-sulfur colloid, this difference could be due to the fact that more sulfur colloid particles are within a unit dose syringe containing 74 MBq of 99mTc-sulfur colloid than 18.5 MBq of 99mTc-sulfur colloid withdrawn from the same bulk vial. However, it was demonstrated in this research study that the number of sulfur colloid particles per activity of 99mTcOH4− within the 99mTc-sulfur colloid bulk vial did not result in significant outcomes.
There were a several limitations noted in this retrospective study. One limitation was being unable to ascertain the time of the patients’ SLN biopsy from documents on the PACS. Additionally, other institutions may follow dose preparation and lymphoscintigraphy protocols different from those used in this study. Another limitation of this study was not being able to determine the actual time, instead of the calibration time, at which the 99mTc-sulfur colloid bulk vials and unit doses were made. Further, no published information was available concerning differences in particle size distribution of 99mTc-sulfur colloid related to the 2 different heating methods. An additional limitation was that several patient factors—including the patients’ age, body weight, breast tissue size, prior surgical and medical history, breast tumor size, or presence of metastases in the SLNs—were not evaluated in this study.
CONCLUSION
Factors involving the preparation and use of the 99mTc-sulfur colloid for SLN mapping and intraoperative localization were investigated. None of the factors examined produced significantly different outcomes related to the number of SLNs visualized during lymphoscintigraphy or removed intraoperatively. Additional research focusing on the outcomes resulting from the administered unit dose activity of 99mTc-sulfur colloid used should be explored. Further investigation is also needed as to whether the integrated temperature–time of fluid inside the 99mTc-sulfur colloid bulk vial during heating preparation, and thus particle size distribution, differs between the water bath and the dry heat block heating methods.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We express thanks to Robin Davis, Neil Petry, Diane Walker, and the Radiopharmacy staff at Duke University Medical Center. Further, we acknowledge Dr. Patrick Kelly and Crystal Botkin from Saint Louis University. We also thank NMAA statistics and research methods professor Dr. Glen Heggie, from the University of Missouri-Columbia, and NMAA program director James Bellamy, from the University of Arkansas for Medical Sciences.
Footnotes
↵† Deceased.
Published online Apr. 29, 2013.
REFERENCES
- Received for publication November 28, 2012.
- Accepted for publication February 24, 2013.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.