


Abstract
Many patients referred for PET suffer from anxiety, possibly affecting the workflow and patient experience. In addition, patient anxiety may affect image quality through uptake of 18F-FDG in muscles or brown adipose tissue (BAT).This study investigated the effects of a nonpharmacologic intervention—the use of audiovisual imagery in the PET uptake room—on patient anxiety and false-positive uptake of 18F-FDG (in muscles and BAT). Methods: A 2-stage study was conducted on 101 patients. The cohort undergoing the intervention included 51 patients. The first stage (n = 35) included physiologic measurements (cardiovascular activity, muscular activity, skin conductance, and cortisol), a state anxiety questionnaire, and visual evaluation of 18F-FDG uptake in muscles and BAT; the second stage (n = 66) included only the state anxiety questionnaire and the 18F-FDG uptake evaluation. Results: Throughout the stay in the uptake room, a significant decrease in overall anxiety was found, together with several other significant changes in patient physiology. In the cohort with audiovisual intervention, however, the decrease in patient anxiety was significantly larger. The cohort with intervention also showed significantly lower 18F-FDG uptake in BAT but not in muscles. Conclusion: The investigated audiovisual intervention helps to lower patient anxiety in the PET uptake room and can lower false-positive 18F-FDG uptake in BAT.
PET with 18F-FDG, either as a separate modality or in combination with CT, is an established imaging modality in oncology. When undergoing such a medical procedure, patients can experience medium to high levels of anxiety. For instance, Flory and Lang (1) recently found that patients in the waiting room before diagnostic testing report high levels of anxiety; these levels are even higher than those of patients undergoing more complicated and risky treatments. High patient anxiety can affect the hospital workflow (e.g., extra time needed to calm the patient, to address patient noncompliance, and other issues) and the patient’s experience. In addition, high patient anxiety may cause unwanted false-positive 18F-FDG uptake in muscles or brown adipose tissue (BAT) and thereby complicate medical diagnosis (2–7).
Patient anxiety is typically measured using self-report instruments. One widely used instrument is the State-Trait Anxiety Inventory (STAI) (8), comprising separate measures for state anxiety and trait anxiety. The full STAI comprises, both for state and for trait, 20 items that can be rated on a 1–4 scale, yielding a total score range of 20–80. There is no formal clinical cutoff, but scores of 40 or more are considered to indicate high anxiety (9). van Knippenberg et al. (10) showed that it is possible to create a reliable 8-item version of the STAI. In addition, anxiety may be reflected in the patient’s physiologic state, quantifiable in terms of, for example, heart rate (variability), skin conductance, muscle tension, and cortisol concentration (11). These physiologic parameters may also be worth observing to gain a broader understanding of 18F-FDG uptake, being a physiologic process.
There currently is no common agreement on the use of pharmacologic interventions to reduce anxiety in PET patients. Sheldon et al. (12) suggested that pharmacologic agents are likely to be effective in decreasing patient anxiety, though few studies have adequate sample sizes to determine the most effective agents. Both Miyasaka et al. (13) and Male et al. (14) found that anxiety was reduced after the use of diazepam in one of their anxiety questionnaires but not in all. Helmus et al. (15) reported that 10 mg of diazepam had an anxiolytic effect only for highly anxious subjects. Dyck and Chung (16) reported that 10 mg of diazepam and 80 mg of propranolol did not decrease preoperative anxiety more than a placebo treatment does. Surprisingly, in one study, anxiety increased in young men both after low-dose (7 mg) and after high-dose (12 mg) diazepam but decreased with a placebo (17). In addition to these mixed results in terms of effectiveness, administration of agents such as diazepam to PET patients may entail several other drawbacks, including ethical objections, inability of outpatients to drive home, and undesirable interactions with other (possibly unknown, prescribed) drugs.
Various nonpharmacologic techniques to lower anxiety have been reported in the literature, including audiovisual imagery, music, physical exercises, art therapy, massage therapy, mental distraction, meditation, progressive muscle relaxation, breathing exercises, and Reiki (12). Most of these, however, seem unsuitable for integration into the PET procedure. For example, some techniques require high physical activity (potentially causing false-positive 18F-FDG uptake in muscles) and others require an extensive time to master. Nevertheless, a few of these techniques may prove implementable and beneficial in terms of patient anxiety reduction. Music is found effective in reducing patient anxiety during the delivery of normal care (18). Videos may also be of added value in lowering anxiety (19). Videos and sounds of nature may be particularly effective because of claimed beneficial effects on restoration of attention (20) and stress coping resources (21).
Besides a general reduction of a patient’s anxiety level, some specific organ systems can be targeted to reduce local false-positive 18F-FDG uptake. For example, to prevent uptake in BAT, a well-controlled room temperature is frequently suggested (22–24). Still, the optimal uptake room temperature remains indefinite. β-adrenergic blocking agents such as propranolol are also reported to lower 18F-FDG uptake in BAT (25,26). To prevent 18F-FDG uptake in muscles, avoiding strenuous exercise before and during the 18F-FDG uptake process is generally advised (5,27). In addition, several studies argue for the use of benzodiazepines such as diazepam to lower 18F-FDG uptake in muscles (3,28). However, these measures are not applicable for all patients (e.g., patients who need to drive a car after the procedure) and carry the previously mentioned inherent disadvantages of pharmacologic interventions.
Given these considerations and issues, a generally applicable and nonpharmacologic strategy to lower the risk of unwanted false-positive 18F-FDG uptake in normal organs is highly anticipated. The main aim of the present study was to investigate whether a nonpharmacologic intervention—the use of audiovisual imagery in the PET uptake room—can help reduce patient anxiety. Second, we wanted to gain insight into the effects of the intervention on 18F-FDG uptake in muscles or BAT. We hypothesized that the intervention would lower patient anxiety in the uptake room and would lower 18F-FDG uptake in muscles and BAT.
MATERIALS AND METHODS
The study was performed at The Netherlands Cancer Institute–Antoni van Leeuwenhoek Hospital, according to its medical ethical protocols. The study comprised 2 successive stages. In stage 1, we applied and evaluated several measurements to gain a broad insight into the effects of the intervention (the latter is further explained in the “Intervention” section). In stage 2, we selected a subset of these measurements targeted to quantify patient anxiety and 18F-FDG uptake in further detail.
Patients
A total of 101 outpatients participated: 35 patients in the first stage and 66 in the second stage. All patients were referred for 18F-FDG PET (or PET/CT) examination at The Netherlands Cancer Institute–Antoni van Leeuwenhoek Hospital from February to May 2011. When entering the Nuclear Medicine Department, patients were randomly assigned to either the intervention cohort or the control cohort by the nuclear medicine technologist. Patients were explicitly asked to give consent for their participation in the study without pay and on a voluntary basis. Patients who failed to give consent were excluded from the study.
Patient characteristics can be found in Table 1. The experimental cohort undergoing the intervention comprised, in total, 51 patients (15 in the first stage and 36 in the second stage) and the control cohort 50 patients (20 in the first stage and 30 in the second stage). Diazepam was administered according to local protocols; this included all patients with a high likelihood of adequate imaging of the nodal areas in the neck and axillae (e.g., breast cancer, head and neck cancer, malignant lymphoma) but excluded patients aged over 65 y and patients who needed to drive a car after the procedure.
Characteristics of the 101 Patients
Intervention
The PET facility at The Netherlands Cancer Institute–Antoni van Leeuwenhoek Hospital has 3 uptake rooms for PET patients. The uptake rooms are roughly comparable in size (∼3 × 3 m) and contain a standard hospital bed. In 1 of the 3 uptake rooms, an audiovisual installation (the experimental intervention) was placed (Fig. 1). In other words, the intervention cohort was placed in the uptake room with audiovisual installation and the control cohort was placed in 1 of the 2 uptake rooms without audiovisual installation.

(Left) Uptake room without audiovisual installation (control). (Right) Uptake room with audiovisual installation (intervention).
The audiovisual installation comprised a 119-cm (47-in) television above the patient bed, colored lighting in the rims around the installation, 4 bright-light spots to facilitate intravenous injection procedures, and a control panel positioned directly outside the uptake room. The content presented on the television was a video containing various nature scenes (19,21). The audio accompanying the visual content was ambient electronic music (29). A low audio volume was used. The rim lighting showed either a static monochrome color or a color that dynamically adapted itself to the colors presented on the television screen, depending on the operation mode. The adaptation algorithm was such that the rim colors would change only slowly and gradually. The light spots, situated next to the television screen, were used to assist the nuclear medicine physician with 18F-FDG injection. The control panel, positioned directly outside the uptake room, let the staff control the audiovisual installation.
Table 2 provides an overview of the workflow and operation modes of the audiovisual installation. The workflow began with the “patient preparation” mode, in which the nuclear medicine technologist informed the patient about the procedure and about the presence of the audiovisual system. The technologist then left the uptake room and the “preview” mode started, to let the patient get used to the audiovisual content. This preview, lasting approximately 2 min, provided the patient with a small selection of the audiovisual content that was to be shown during the later “low-stimuli” operation mode. The short preview was stopped on 18F-FDG administration, and the system was switched to the “injection” mode. After the nuclear medicine physician had injected the 18F-FDG, the “very-low-stimuli” mode was started, allowing the patient to rest or sleep without distraction. This mode lasted 30 min and was applied to avoid potential 18F-FDG uptake in areas such as ocular muscles and the visual and auditory cortex, because most 18F-FDG is taken up by tissues in the first 30 min after administration. Subsequently, after this 30-min period, through a slow transition, the “low-stimuli” mode was started to relax the patient for the remainder of the resting time.
Operation Modes of Audiovisual Installation Throughout PET Uptake Procedure
Measurements
An overview of all measurements included in the study is provided in Table 3. Patient anxiety was measured by means of a shortened 8-item Dutch version of the STAI (using items 4, 5, 7, 10, 12, 15, 16, and 19 (30)), from which the state anxiety component was used to assess feelings of apprehension, tension, nervousness, and worry as experienced at the time of the assessment. Therefore, the high-anxiety STAI threshold of 40 points for the 20-item STAI (9) was converted to a threshold of (40/20 × 8 =) 16 points for the 8-item STAI used in the present work. STAI was administered twice; at the beginning of the uptake period and at the end of the uptake period.
Measurements
Several physiologic parameters were measured (Table 3). Electrophysiologic measurements were performed using the Nexus-10 recorder (TMS International BV). A 3-lead surface electrocardiogram was used, with Ag/AgCl electrodes placed on the patient’s thorax; the sample rate was 1,024 Hz. The electromyogram was obtained from the upper trapezius muscle, using 2 Ag/AgCl electrodes, placed in accordance with Cram's Introduction to Surface Electromyography (31). Electrodermal activity was measured using isotonic (0.5% saline) wet gel electrodes attached to the outer phalanges of the index and ring finger of the patient’s nondominant hand. After filtering (fourth-order Butterworth; pass band 10–400 Hz for electrocardiogram and electromyogram and low-pass 1 Hz for electrodermogram) of the raw physiologic data, parameters were calculated over 5-min epochs and all were normalized into z scores. Heart rate was calculated from the R-R intervals. Heart rate variability was calculated as the root-mean-square of the successive R-R interval differences. From the preprocessed electromyogram, the root-mean-square amplitude of the signal was calculated. For all electrophysiologic features, 2 epochs were selected; heart rate at the beginning of the uptake period and heart rate at the end of the uptake period. In addition to the electrophysiologic measurements, cortisol concentration was determined from 2 saliva samples; 1 at the beginning of the uptake period and 1 at the end of the uptake period. Cortisol samples were analyzed using a cortisol luminescence immunoassay (IBL International GmbH).
To analyze 18F-FDG uptake, scan images were acquired using an integrated PET/CT scanner (Gemini II; Philips). The interval between 18F-FDG administration and scanning was 60 ± 10 min. Generated images (PET/CT, low-dose CT, and PET) were displayed using an Osirix DICOM viewer in a Unix-based operating system (MAC OS X; MAC Pro; Apple) and were evaluated on the basis of 2-dimensional orthogonal reslicing. PET, fused PET/CT, and CT were analyzed side-by-side during a meeting of 3 experienced nuclear medicine physicians. Uptake of 18F-FDG in BAT and muscles was defined as the presence of 18F-FDG on PET images in the cervical, paraspinal, and trapezius areas. 18F-FDG uptake was visually evaluated by consensus, using a 4-point system: 0 = not distinguishable from normal surrounding background tissue, 1 = slightly more than background intensity, 2 = moderately intense, and 3 = very intense (22). Outdoor temperature was investigated as a possible nuisance factor, since it can influence uptake in BAT (32). Outdoor temperatures (i.e., mean temperature on day of PET examination at nearest measurement location) were gathered in retrospect (33). In addition, temperatures inside the intervention room and in one of the control rooms were measured throughout a period of 10 working days, several weeks after the experiment. Both measurements were done at a similar height in the room (i.e., close to the ceiling, to avoid theft and obstruction of the medical procedure) and at a similar distance from the door.
Because indoor temperature measurements were not done during the actual experiment, this factor could not be directly controlled for. Instead, we investigated indirectly whether room temperature may affect the interpretation of the statistical analysis. Blankets were provided to all patients.
Statistical Analysis
Statistical analysis was performed using SPSS version 17 for Windows (Microsoft). From all measurements except 18F-FDG uptake, delta values were calculated by subtracting the beginning epoch value from the ending epoch value. For example, the change in STAI resulted from subtracting STAI at the end of the uptake period from that at the beginning of the uptake period. Paired-samples t tests were used to analyze the overall changes during the uptake period (e.g., comparing STAI at the end and beginning of uptake over all conditions). Independent-samples t tests were performed to analyze the effects of the intervention (e.g., comparing the change in STAI for the intervention cohort with that for the control cohort). Pearson correlation tests were performed to assess the correlations between STAI and the physiologic parameters.
18F-FDG uptake was analyzed by comparing presence–absence ratios between cohorts; presence meaning a patient was given an evaluation score of at least 1 in at least 1 of the evaluated body areas (22). The resulting presence–absence ratios were analyzed using Fisher exact tests. In the 18F-FDG analysis, outdoor temperature (as a potential nuisance factor) was controlled for by estimating a binary logistic model in which the binary response indicated whether there was BAT uptake and the predictor terms were intervention and outdoor temperature. Effects were flagged as statistically significant if P was less than 0.05.
RESULTS
Between the 2 rooms without intervention, no significant differences were found in patient anxiety or physiology. Therefore, the results of these 2 rooms were aggregated. The experimental cohort and control cohort were found comparable (i.e., not significantly different) in terms of age, body mass index, sex, visit number, diazepam use, and anxiety level (STAI) at the beginning of uptake. Of all patients, 32% were administered diazepam.
On the basis of the STAI scores at the beginning of uptake, and using the STAI threshold described in the “Materials and Methods” section, 59% of all patients could be classified as highly anxious. First-time visitors to the PET facility were significantly more anxious than return visitors in terms of the beginning STAI score. However, no differences were found regarding the change in STAI between the first-time and return visitors.
In the first stage, only 2 technologists were involved: 1 experienced and 1 less experienced. No significant differences in patient anxiety were found between the data gathered by the 2 technologists. Therefore, in the second stage of the study, 5 more technologists were allowed in the study execution.
Overall Changes Throughout the Uptake Period
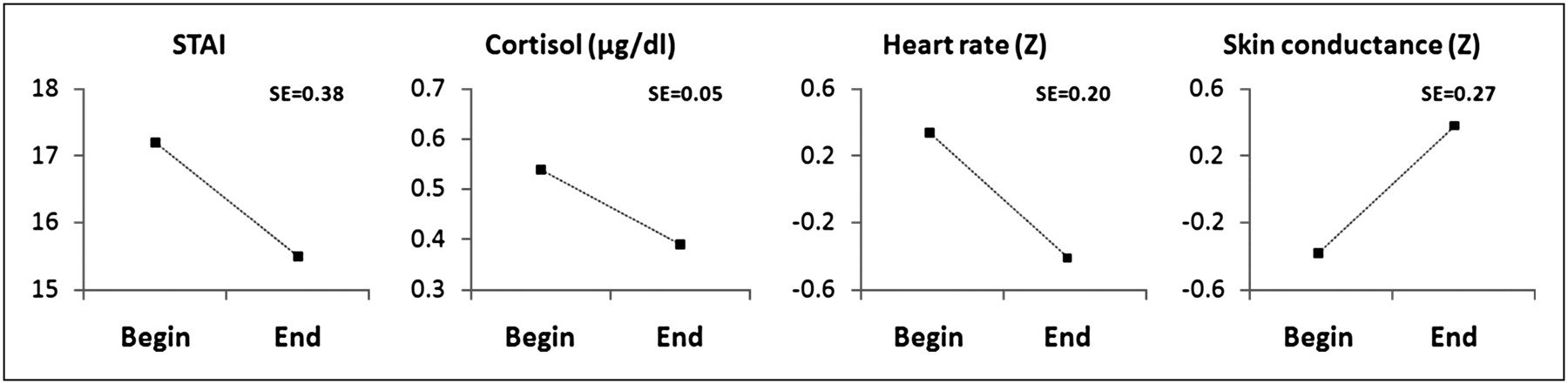
When considering all included patients, regardless of the intervention, changes were found in several measurements during the uptake period (Fig. 2; Table 4): STAI, cortisol, and heart rate were all congruent with a significant reduction in patient anxiety during the uptake period. Skin conductance, on the other hand, increased significantly—a change that is incongruent with a reduction in anxiety. The other measured parameters did not change significantly over time.
Overall Changes (i.e., “Delta” Values) Throughout the Uptake Period
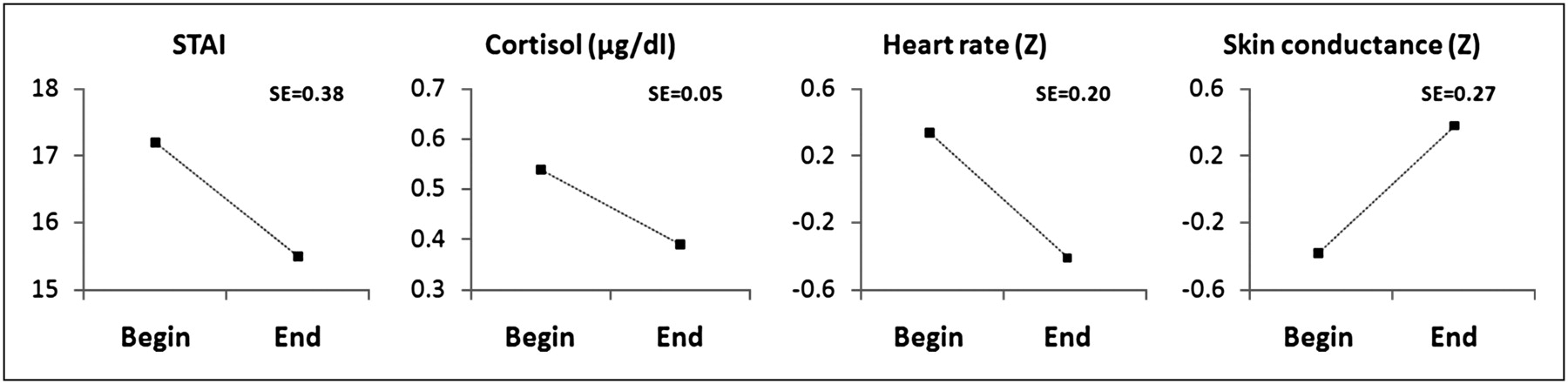
Changes in anxiety and physiology during uptake period for whole cohort, including both control and intervention groups. SE = SE of within-person differences.
Effect of the Intervention
On the basis of STAI, the intervention significantly lowered patient anxiety (Fig. 3; Table 5). None of the physiologic parameters correlated significantly with STAI (regarded as the anxiety benchmark), and therefore STAI was considered the only valid measurement of patient anxiety.
Effect of the Intervention
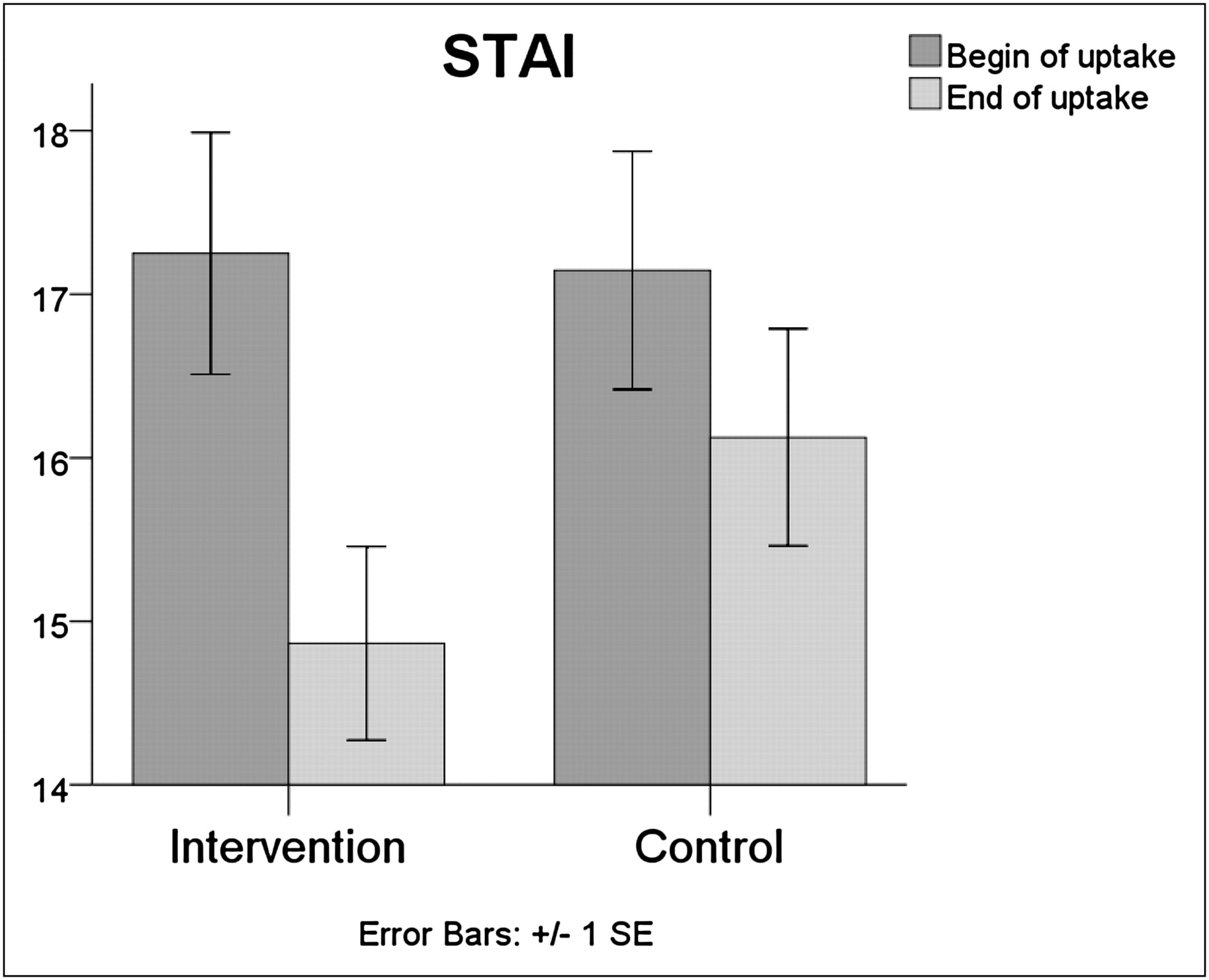
Intervention significantly lowers patient anxiety.
18F-FDG uptake in normal tissue is presented in Table 4. No significant differences were found in false-positive 18F-FDG uptake in the evaluated muscle areas. In contrast, significant differences were found for uptake in BAT; the intervention group showed significantly less uptake in BAT. The intervention cohort also had significantly less BAT uptake when we controlled for outdoor temperature. That is, in the binary logistic regression model, the factor “Intervention” was significant and the covariate “Outdoor Temperature” was not significant. The average outdoor temperature was 6.8°C (SD, 5.4) for the invention cohort and 4.6°C (SD, 4.1) for the control cohort. The average temperature measured in the intervention room (at ceiling level) was 26.5°C (SD, 0.2), and the temperature in the control room was 26.9°C (SD, 0.1).
DISCUSSION
The results of this study indicate that many patients (59%) enter the PET uptake room with high anxiety and that many patients demonstrate unwanted 18F-FDG uptake in normal tissues, emphasizing the need for a solution. To our knowledge, the only previous study of patient anxiety in a PET context is that of Westerman et al. (34) reporting lower levels of anxiety. However, several methodologic differences exist between their study and the present work. For instance, Westerman et al. used the Hospital Anxiety and Depression Scale (35), targeting patient anxiety experienced over the 7 d before the examination, as opposed to STAI used in the present work, targeting anxiety at the time of the examination.
Although patient anxiety decreases spontaneously during the stay in an uptake room, we found that an additional intervention with audiovisual stimuli further reduces patient anxiety and benefits image quality with respect to unwanted uptake of 18F-FDG in BAT. Therefore, the presented audiovisual intervention may be considered for implementation in the PET (or PET/CT) uptake procedure instead of, or in addition to, pharmacologic means to lower patient anxiety or 18F-FDG uptake in BAT. We were able to show the reduction in patient anxiety using the STAI, but the physiologic measurements did not correlate with the STAI. This noncorrelation may, to an extent, be explained by other processes influencing physiology, such as thermoregulation. This is of particular relevance because the temperature inside the uptake room is relatively high compared with the temperature outside the uptake room. The extra influences may explain why, from an anxiety perspective, the physiologic results appear somewhat discrepant. For example, controlled lab studies typically report that lowered anxiety yields a decrease in skin conductance (36), as opposed to the increase in skin conductance over time found in the present study. In addition, STAI and the physiologic measurements differ in their temporal scope. STAI focused on patient anxiety as experienced at the current time, whereas, for example, cortisol changes are known to occur over a 60-min epoch after stressor onset, peaking about 30 min after onset (37). Because of these factors, STAI was considered the only valid anxiety measurement.
The experiment was not fully masked; patients in the intervention group might have been treated previously in a control room. Nevertheless, the factor “Visit Number” did not influence the intervention’s anxiety-reduction effect. There also was no difference in anxiety between the patients with and the patients without diazepam. From the latter, however, no causal relationship can be inferred because diazepam was not distributed randomly over the groups. Although there was a clear beneficial effect on uptake in BAT, no effects were found with respect to 18F-FDG uptake in the evaluated muscular areas. We conclude that muscle relaxation is adequate in a resting room. In view of the fact that BAT is stimulated by the sympathetic nervous system (7) and used for thermogenesis, the differences in BAT uptake may have been due to differences in patient anxiety (i.e., less sympathetic nervous system activity) (6). Therefore, additional temperature analyses were performed. The differences in BAT uptake between cohorts were also found when outdoor temperature was taken into account. Regarding indoor temperature, from the literature we expect that if indoor temperature has any effect, then a lower temperature will cause a larger degree of uptake in BAT (22–24). We, however, observe the opposite effect in the present study, with the intervention room having been 0.4°C colder. In sum, the intervention cohort showed lower BAT uptake when we controlled for outdoor temperature. Given our retrospective room temperature measurements, we consider it unlikely that room temperature differences can explain this result.
Further research is needed to investigate the effects of the audiovisual installation on false-positive 18F-FDG uptake, particularly BAT uptake, in more detail. Several possibly confounding factors can be monitored or controlled for, including skin temperature, room temperature on the day of measurement, use of blankets, exact outdoor temperature, transportation means (e.g., transportation by bike or taxi to the PET facility), and time spent in the waiting room. These factors may help to provide more information regarding the exact influence of temperature on the effect of the intervention on BAT uptake,
Besides further examination of the effects on 18F-FDG uptake, the effectiveness of the intervention itself may be increased in several ways. For example, providing the patient with a choice of audiovisual content may increase the patient’s satisfaction and sense of control. Another way to increase the effectiveness of the intervention is by separately analyzing the effect of all features in the audiovisual installation (video, audio, lighting) to determine the optimal combination of features. Furthermore, the 30-min very-low-stimuli safety buffer (Table 2) may be reduced. That is, the video may start earlier since the intervention did not seem to increase 18F-FDG uptake. The introduction of more stimuli in the first 30 min would, however, require more detailed analyses focusing on false-positive 18F-FDG uptake in relevant tissues. These would include mainly the brain (the visual and auditory cortex) and ocular muscles.
CONCLUSION
The investigated audiovisual intervention helps to lower patient anxiety in the PET uptake room and can lower false-positive 18F-FDG uptake in BAT, without the disadvantages associated with pharmacologic interventions.
Acknowledgments
We thank the following persons for their contribution to this study: Colinda Vroonland and Minette Romano-Vraai from The Netherlands Cancer Institute–Antoni van Leeuwenhoek Hospital, Jan Engel and Jan Willem Bikker from CQM Statistics, Richard van der Wolf and Bram de Regt from MiPlaza Hi-Tech Services, and Cor Datema from Philips Healthcare. This study was the result of a balanced research collaboration between The Netherlands Cancer Institute–Antoni van Leeuwenhoek Hospital and Philips Research Laboratories Europe. The authors have or had no financial or other relationship that can be construed as a conflict of interest in this respect.
Footnotes
Published online May 8, 2012.
REFERENCES
- Received for publication September 6, 2011.
- Accepted for publication January 13, 2012.





{kind=link}
{kind=link}
{kind=link}