


Abstract
Unintentional intraarterial injection of radiotracers may cause artifacts leading to difficulties in accurately interpreting PET/CT images. We report a case of a 73-y-old man with a history of metastatic colon cancer who underwent a PET/CT scan for restaging. In the PET scan, there was intense and diffuse distribution of 18F-FDG in his left forearm and hand. This is a classic sign of an accidental intraarterial injection of 18F-FDG in the antecubital region. Similar phenomena after inadvertent intraarterial injection of other radiotracers are reviewed. The associated risk factors, preventive measures, and radiation dose to the arm are discussed.
Unintentional intraarterial injection of radiotracers, including 99mTc-methylene diphosphonate, 99mTc-sestamibi, and 201Tl-chloride, may cause artifacts leading to difficulties in accurately interpreting these functional images (1–7). Under these conditions, the images usually show intense uptake in the extremity distal to the injection site, in a pattern previously described as a hot forearm, a hot hand, or a glove phenomenon. Here, we present a patient with a similar phenomenon in his left forearm and hand on a PET/CT scan after an inadvertent intraarterial injection of 18F-FDG.
CASE REPORT
A 73-y-old man was diagnosed with stage IV adenocarcinoma of the cecum, with liver metastasis, one and a half years previously. He underwent a right hemicolectomy and partial hepatectomy. He then received multiple rounds of chemotherapy, including folinic acid, fluorouracil, and oxaliplatin, plus bevacizumab, capecitabine, irinotecan, and cetuximab. After his most recent round of therapy, he was referred for a restaging PET/CT scan.
When performing the intravenous injection of 18F-FDG, the technologist encountered difficulty obtaining intravenous access, possibly because of the multiple courses of chemotherapy and antiangiogenesis therapy. Once access was obtained, 535 MBq (14.46 mCi) of 18F-FDG were injected into the patient's left antecubital access. Approximately 120 min later, a PET/CT scan was obtained from mid thigh to skull base with a Discovery LS PET/CT system (GE Healthcare).
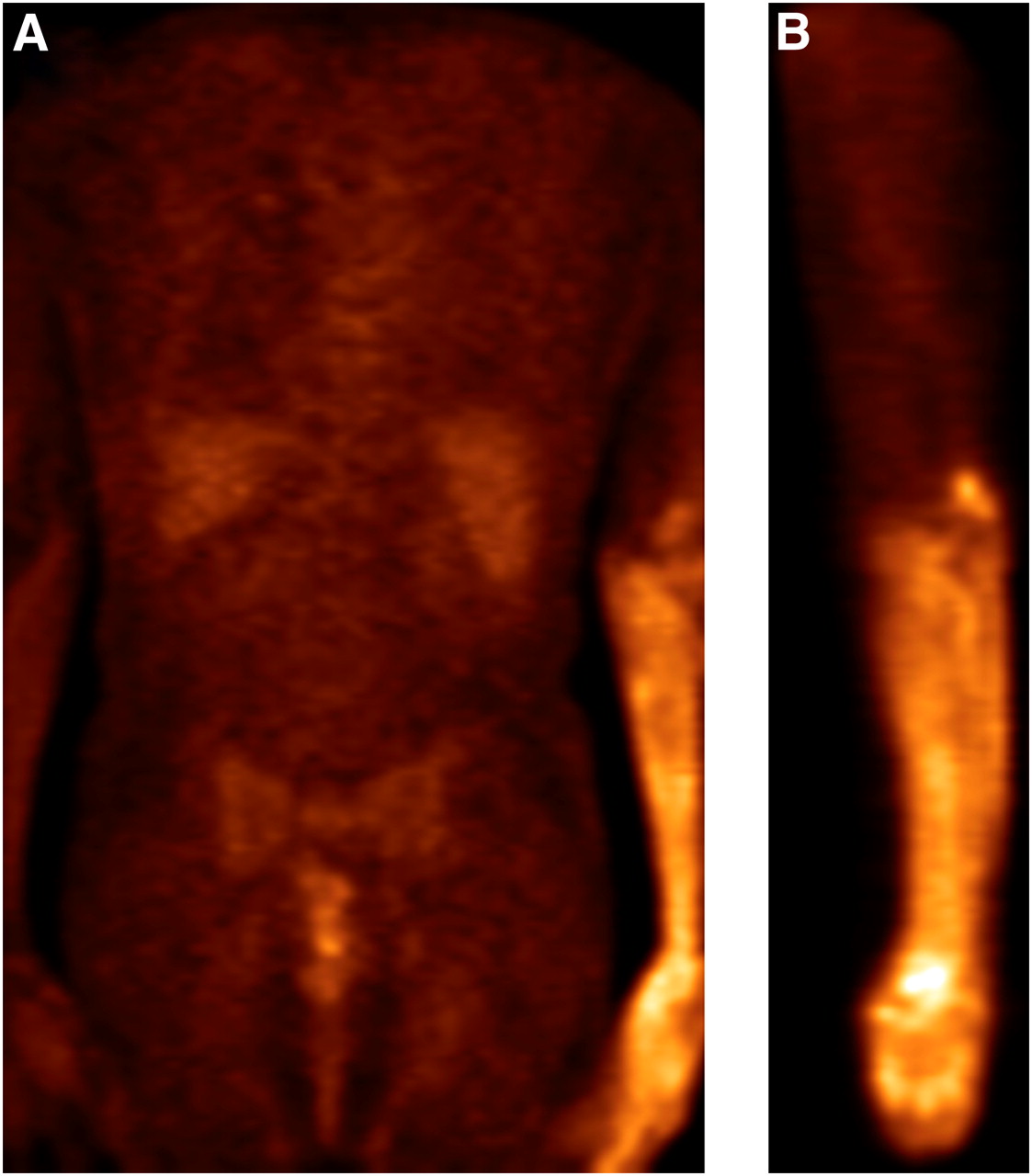
On the PET/CT images, multiple focal lesions were found in the mesentery, liver, and both lungs, with standardized uptake values (SUVs) ranging from 2.2 to 6.9, indicating possible metastasis of colon cancer. There were also 2 tumors with SUVs of 3.0 and 7.5 at his left tonsil and left upper neck, respectively, which were later diagnosed to be a second primary squamous cell carcinoma of the tonsil with spread to the regional lymph nodes. Moreover, his whole left forearm, left hand, and fingers showed intense and diffuse 18F-FDG uptake consistent with the blood distribution of a brachial artery (Fig. 1), with a maximum SUV of 8.8. The maximum SUV of the contralateral forearm and hand was approximately 1.1. There was no special finding in this region in either the previous PET/CT scan 3 mo earlier or a follow-up PET/CT study 3 mo later. Our inference is that the radiotracer was inadvertently injected into the brachial artery rather than an antecubital vein in our present study, and the images showed a typical hot hand and hot forearm sign.

18F-FDG PET images (coronal [A] and sagittal [B]) show distribution pattern indicative of accidental injection of 18F-FDG into left brachial artery rather than antecubital vein.
The average SUV in the hot forearm was about 6 times higher than the average SUV in the contralateral forearm. The normal dose to forearm (other organs) from the injected 18F-FDG is 0.55 μSv/MBq (8). Assuming that the main contribution to the forearm dose is from the activity in the forearm itself, the dose to the hot forearm was estimated using this conversion factor (scaled by 6) and found to be approximately 1.8 mSv. This is significantly below the 20-mSv organ dose specified by the Nuclear Regulatory Commission for defining misadministration.
DISCUSSION
It is well established that an unintentional intraarterial injection of 99mTc-methylene diphosphonate can produce a hot forearm or hot hand sign characterized by a pronounced soft-tissue uptake distal to the arterial distribution, which is also called the glove phenomenon in some reports (1–4). When the increased 99mTc-methylene diphosphonate uptake is restricted only to the ipsilateral bones and periarticular regions, it can also mimic a reflex sympathetic dystrophy (5). These phenomena are different from extravascular leakage (9,10).
More serious interferences have been observed when 99mTc-sestamibi or 201Tl-chloride for myocardial perfusion scintigraphy was accidentally injected into the artery (6,7). These kinds of tracers accumulate preferentially in the skeletal muscles, with the region of intense uptake extending from the forearm and hand to the upper arm and even to the shoulder (6). Moreover, the quality of the reconstructed cardiac images deteriorates remarkably as the skeletal muscle absorbs most of the radioactivity.
The incidence of inadvertent intraarterial injection of 18F-FDG is likely underestimated because the hands and forearms are often not included in the PET/CT images. It might also have been ignored or considered as a leakage of radioactivity in some cases. Usually, when 18F-FDG is mistakenly injected into a brachial artery, the image quality of PET is still suitable for visual interpretation (11,12). However, the SUVs of the lesions may be underestimated as indicated by the lower SUVs in liver or mediastinal soft tissues, in comparison to other normally injected patients. SUV correction techniques for 18F-FDG injection with venous leakage or extravasation have been investigated, and a similar technique may be applicable in instances of intraarterial injections (13).
Assessment of risk factors before a venipuncture is important. An intravenous injection for patients referred for a PET/CT scan or a bone scan is sometimes challenging because they may have a history of malignancy and the superficial veins may have shrunk after multiple courses of chemotherapy. In addition, for those patients referred for myocardial scintigraphy, the superficial veins may not be clearly visualized because of the obesity and diabetes that are commonly encountered in these patients. In addition, elderly patients with dehydration or vessel disease are also more prone to accidental arterial puncture. Under these conditions of high risk, an intravenous injection should be performed with care to avoid either accidental intraarterial injection or radioactivity leakage.
A good understanding of the normal anatomy and variations of the vessels is important to avoid an inadvertent intraarterial injection. Taking the antecubital fossa venipuncture as an example, there are 3 main veins commonly used, including the basilic vein, the median cubital vein, and the cephalic vein. The brachial artery and its 2 main branches, the ulnar artery and the radial artery, may run right beneath these superficial veins (14). Under difficult conditions, careful observation of the color and movement of blood return would be helpful to ensure accurate venous access.
After this incident, all our technologists received in-service training from hospital intravenous nurses. The variability of the venous anatomy was discussed; catheter insertion techniques and angles were the main discussion points. Visual assessment after catheter placement was emphasized, as was rechecking before tracer administration. The technologists were enjoined not to administer the tracer if pulsation of the catheter is observed. Also, they were asked to obtain a second opinion if there was uncertainty about the catheter placement. Since the training, we have not had any arterial injections.
In summary, the first-pass effect contributed to a different distribution pattern of a radioactive tracer when it was inadvertently injected into an artery. A tracer that is more susceptible to uptake by the forearm or hand is more likely to produce the hot forearm or hot hand sign. The variation of image pattern is related to the involved artery and its perfusion, as well as the extraction ability of the corresponding tissues for a specific radiotracer. In fact, in radionuclide assessment of peripheral arterial diseases, intraarterial injection of 99mTc-labeled human serum albumin microspheres was used as a noninvasive method before exercise plus intravenous injection of 99mTc-sestamibi had been established (15,16).
As reported in many clinical cases, mistaken delivery of certain intravenous medications via arterial access has led to serious sequelae, including paresthesias, severe pain, motor dysfunction, compartment syndrome, gangrene, and even limb loss (17). Although the consequences are much less serious for radionuclide imaging, the personnel who administer the intravenous injections should be aware of this potential problem to minimize its impact.
CONCLUSION
Intraarterial injection of 18F-FDG can result in artifacts such as hot hand or hot arm in PET images. Knowledge of the normal anatomy and its variations can help to reduce the incidence of such injections.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 24, 2011.
REFERENCES
- Received for publication February 8, 2011.
- Accepted for publication June 16, 2011.





{kind=link}