


Abstract
The goal of this article is to delineate indications for 18F-FDG PET/CT pertaining to inflammation in the pediatric population, with emphasis on those that have been described in the literature. The limitations of 18F-FDG PET/CT in this type of evaluation are also described, and the importance of using as low a dose as feasible is discussed. After reading this article, the reader should be able to list several clinical situations in which 18F-FDG PET/CT may be appropriate, describe some limitations of 18F-FDG PET/CT, and explain why dose is particularly important in the pediatric population.
The use of 18F-FDG PET/CT for various oncologic indications is increasing. The mechanism for the success of 18F-FDG PET/CT in this setting is the accumulation of 18F-FDG in tissues with a high rate of glycolysis, as is typical in neoplastic tissues. Because 18F-FDG is a structural analog for 2-deoxyglucose, 18F-FDG is taken up by mammalian cells that use glucose (1). Infection and inflammation result in activated leukocytes, which also use glucose as an energy source after activation during the metabolic burst. One hypothesis is that glucose transporter receptors are stimulated, with the resultant uptake of glucose and its analogs (2). Therefore, this clinical scenario is also ideal for the accumulation of 18F-FDG.
THE PROS AND CONS
Among the advantages of 18F-FDG PET/CT is the combination of functional imaging and precise anatomic localization. Also, both acute and chronic processes can be detected. In comparison to other nuclear imaging such as radiolabeled white blood cell scans, 18F-FDG PET/CT requires less time, is less labor-intensive, and provides higher-resolution images. Thus far, the literature has shown some promising results.
Disadvantages of 18F-FDG PET/CT include its lack of availability and the cost for the examination. In addition, because the uptake of radiotracer is not specific to inflammatory processes, a neoplastic process cannot be discriminated from infection solely on the basis of the imaging findings.
INFECTION AND INFLAMMATION
Fever of Unknown Origin
One challenge in clinical medicine is the difficulty in diagnosing fever of unknown origin. This entity has varied definitions, ranging from fever lasting longer than 1 wk that remains unexplained even after an extensive work-up in children, to any fever lasting 3 wk; the term fever without source is also used. Most often, the etiology is infectious, but rheumatologic or neoplastic issues may also give rise to this clinical scenario.
Part of the challenge in diagnosing fever of unknown origin is the subtlety of the pathologic changes. These may therefore not be detectable by conventional imaging, which typically relies on anatomic changes to enable detection. The clinical findings too, may provide little insight into the etiology of the fever. The work-up of these patients has been described in many publications and is beyond the scope of this review, varying with the child's age but always beginning with an extensive history and physical examination.
There are several publications illustrating the utility of 18F-FDG PET/CT in the setting of pediatric infection or inflammation. In a study by Jasper et al., 69 children underwent 18F-FDG PET or 18F-FDG PET/CT for fever of unknown origin or inflammation without fever (3). Most of the patients who received a final diagnosis were aided by this imaging. Another study demonstrates a specific clinical situation in which children with fever of unknown origin can benefit from 18F-FDG PET (4). Children with liver failure who are awaiting transplantation sometimes develop fever of unknown origin. Systemic infection is a contraindication to the transplantation that they need. Sometimes the fever may be due to infection within the diseased liver, in which case the transplantation would be feasible and potentially curative. Children who have an abnormal accumulation of 18F-FDG exclusively in their liver undergo the curative transplantation. In some others, the site of infection can be localized and then treated successfully. The ability of 18F-FDG PET to localize the site of infection in these patients significantly affects the clinical care of these patients. 18F-FDG PET/CT has also been shown to identify pneumonia, bronchitis, cytomegalovirus, infection in the spleen, disseminated candidiasis, colitis, and chronic osteomyelitis in children (5–7) (Fig. 1). 18F-FDG PET provides much better spatial resolution in less time than 67Ga-citrate imaging, which is often used in questions of infection or inflammation.
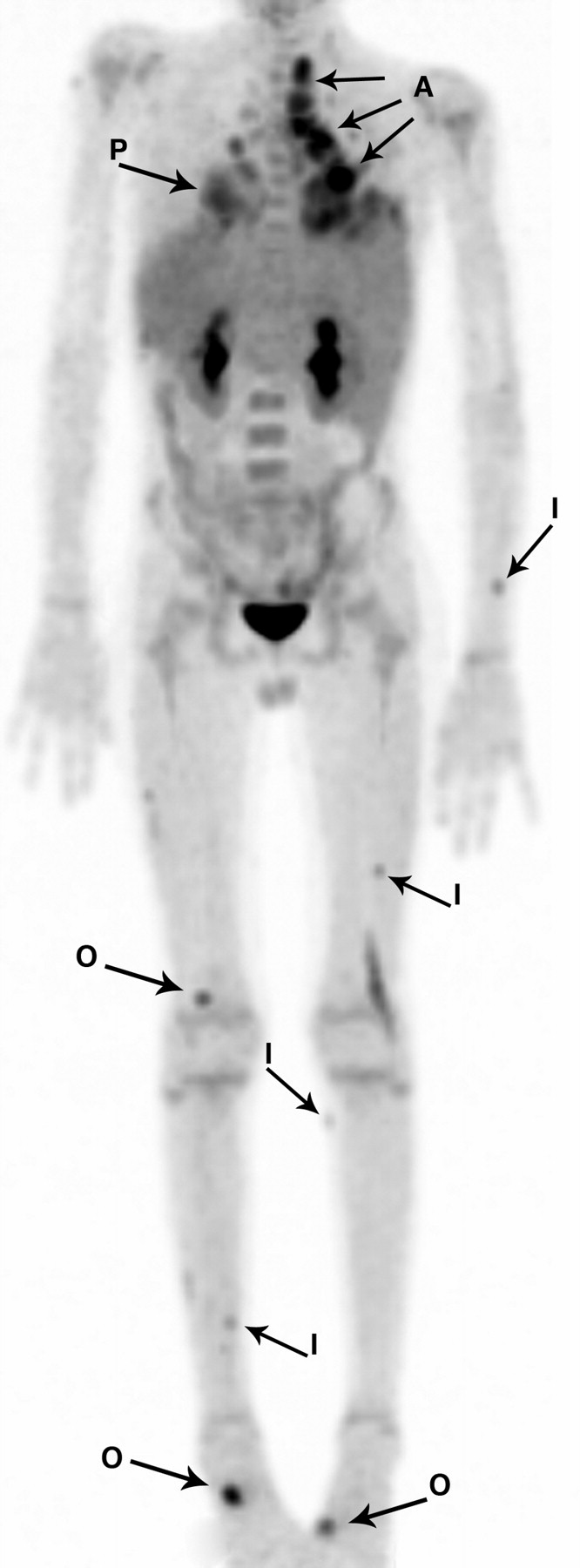
An 11-y-old boy with history of X-linked chronic granulomatous disease who underwent 18F-FDG PET/CT as part of his work-up. Coronal PET image demonstrates several areas of osteomyelitis (both feet and distal right femur) (O), several soft-tissue sites of inflammation (left forearm, left femur, and both shins) (I), pneumonia (P), and paratracheal and hilar adenopathy (A).
Gastrointestinal
Inflammatory bowel disease—increasingly diagnosed in children—is another condition that can be identified with 18F-FDG PET/CT. A publication dating back to 1999 demonstrated the ability of PET to reveal inflammation from Crohn disease in children (8). More recently, a retrospective study of 23 children with varied forms of inflammatory bowel disease or enteritis were evaluated with PET, endoscopy, histology, and sonography, with PET showing excellent sensitivity (9). In a prospective study, 65 children with Crohn disease or ulcerative colitis underwent PET, fluoroscopic small-bowel follow through, and colonoscopy, with good results (10). The ability to diagnose inflammation and its location can aid in the treatment of children with symptoms of inflammatory bowel disease and potentially end the growth and development issues that may also stem from the disease.
Musculoskeletal
Musculoskeletal inflammation and infection can also be detected with PET (11–13). Langerhans cell histiocytosis, which most often presents as osseous disease in children, is due to overproduction of a white cell (Langerhans cell). Although the exact mechanism is not understood, the process is hypothesized to be reactive or neoplastic. Most patients who are less than 2 y of age and have disseminated disease will succumb to their illness. Several publications have demonstrated the utility of 18F-FDG PET/CT in the care of these patients (14–16). More lesions can be detected on 18F-FDG PET than on radiography or 99mTc-methylene diphosphate bone scanning (14,16). 18F-FDG PET is purported to be the modality of choice in evaluating the effectiveness of Langerhans cell histiocytosis treatment in children.
Osteomyelitis is a frequent indication for imaging. Most commonly used in the pediatric population is MRI, which has the benefit of not requiring any ionizing radiation while providing excellent diagnostic results. In 1998, Guhlmann published a study demonstrating the effectiveness of 18F-FDG PET in diagnosing chronic osteomyelitis (17), and there have been many studies in adults since then. We have seen 18F-FDG PET scans positive for osteomyelitis in children (Fig. 1), but additional investigation is required to demonstrate utility in the pediatric population, particularly in comparison to bone scans.
Vessels
Vasculitis can affect arteries and veins of any size and, in children, is found in conditions such as Henoch-Schonlein purpura, Kawasaki disease, infantile polyarteritis nodosa, and Takayasu disease. Diagnosis typically relies on biopsy, conventional angiography, ultrasound, or MR angiography. However, PET has been shown capable of revealing vasculitis in adults (18). At our institution, we have seen 18F-FDG PET scans positive for vasculitis in pediatric patients (Fig. 2).

A 13-y-old girl with Takayasu's vasculitis as demonstrated by this PET image showing uptake bilaterally in superficial femoral arteries (arrows). This patient also underwent CT angiography, MR angiography, and ultrasound demonstrating arterial wall thickening in same areas as seen on PET. She was treated with prednisone and responded well.
PATIENT PREPARATION
For the scan to be successful, appropriate patient preparation is crucial. Any patient can be anxious before any procedure, including imaging. Therefore, age-appropriate information about what will happen during the examination is critical. Fasting before 18F-FDG PET is necessary to ensure that the blood glucose level is less than 150 mg/dL. Both for comfort and for improved image quality, the patient should empty the bladder before the examination starts. The patient should be kept warm before receiving the injection and while in the scan room to decrease uptake in brown fat, as well as for patient comfort. The patient cannot talk or chew gum after the injection of 18F FDG and during the uptake period, or there will be uptake in jaw muscles and vocal cords. To prevent uptake in other muscles, no exercise or activities that require even minor motion, such as handheld video games or texting devices, should be allowed.
LIMITATIONS
18F-FDG PET/CT has several limitations. Physiologic activity interferes with the specificity of 18F-FDG uptake and can make interpretation of the scans challenging. Uptake may result from talking or a cold environment. Unavoidably, there will be uptake in the central nervous system and urinary tract. Gastrointestinal and reactive lymph nodes may also cause false-positive findings. Conversely, small lesions may not be detected by 18F-FDG PET/CT. Radiation dose is a particular concern in the pediatric population, and therefore, examinations that do not use ionizing radiation may be preferred.
“IMAGE GENTLY”
Radiation dose is a concern for all our patients but is of particular importance in our youngest patients. Children are growing and have rapidly dividing cells, which are replicating DNA. Ionizing radiation can damage DNA, and this damage can potentially be passed along to all further copies of DNA, therefore causing children to be more sensitive to the effects of ionizing radiation than adults. Also, there is often a latency period before the deleterious effects of ionizing radiation are manifest, and given that children have a longer life expectancy than adults, they have a longer time to manifest these deleterious effects. The fact that radiation dose is cumulative over an individual's lifetime also puts children in greater jeopardy.
Historically, CT has been one of the biggest culprits in contributing unnecessarily high doses of radiation to children due to its increasing use in the pediatric population, particularly for such conditions as appendicitis. In addition, the same CT parameters that were used for adults were used in children, despite the child's smaller cross-sectional area. Many publications have described these issues, and a publication in 2001 estimated that a 1-y-old child had a 0.18% risk of dying from cancer due to a single abdominal CT scan (19).
The Pediatric Nuclear Medicine Dose Reduction Workgroup established a consensus of dose ranges for 11 radiopharmaceuticals appropriate for use in children, and the Society of Nuclear Medicine in partnership with the Society for Pediatric Radiology and the American College of Radiology endorsed these dose ranges (20). In a recent publication on 18F-FDG PET/CT doses in children, the authors made several recommendations on keeping dose as low as feasible (21).
CONCLUSION
The role of 18F-FDG PET/CT continues to evolve and has been shown to affect children who have infection or inflammation. Recognizing that children are particularly sensitive to the effects of radiation is important when one is recommending an imaging examination, but 18F-FDG PET/CT can help in the care of children and potentially obviate additional imaging. As more studies are performed in this arena, we will likely see more changes in the use of 18F-FDG PET/CT.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH SEPTEMBER 2013.
Published online Jul. 27, 2011.
REFERENCES
- Received for publication January 23, 2011.
- Accepted for publication April 15, 2011.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.