


Abstract
PET/CT fusion of anatomic and functional imaging modalities is in evolution, with rapid clinical dissemination. The imaged field of view (FOV) selected for whole-body PET/CT protocols is not standardized and varies by institution. Misuse of the term whole body, as well as the pressure to increase the number of daily studies by reducing scanning time, contributes to the lack of standardization. The purpose of this study was to evaluate variations in the FOV and arm positioning selected for whole-body PET/CT protocols at private, as well as academic, PET centers. Methods: Two hundred consecutive whole-body 18F-FDG PET/CT studies were retrospectively reviewed for FOV: 50 studies from a private stationary site, 50 studies from 2 separate private mobile sites (25 consecutive studies from each), and 100 studies from a stationary university site: 50 before and 50 after implementation of a true whole-body protocol covering the top of the head through the bottom of the feet. Data were categorized into 5 different anatomic scan lengths: base of skull to upper thigh, base of skull to mid thigh, top of head to upper thigh, top of head to mid thigh, and true whole-body. Studies were further categorized into 2 patient arm positions: up and down. Results: The private stationary and mobile sites had only 2 categories of anatomic scan lengths identified: base of skull to mid thigh, and top of head to upper thigh. At the university site, before implementation of a true whole-body protocol, the 5 different anatomic scan lengths were identified; after implementation, only the true whole-body scan length was identified. Patients’ arms in the private stationary sites were down 100% of the time. At the private mobile sites, patients’ arms were up 72% of the time and down 28% of the time. At the university site, patients’ arms were up 54% of the time and down 46% of the time. The same site, after implementation of a true whole-body protocol, had patients’ arms up 58% of the time and down 42% of the time. Overall, patients’ arms were up 46% of the time and down 54% of the time. Conclusion: The continued use of the term whole body is misleading because frequently it may not include the brain, skull, or significant portions of the upper and lower extremities. PET/CT anatomic scan length varied not only from one site to the next but also within individual sites. The Centers for Medicare and Medicaid Services have different current procedural terminology codes distinguishing between base of skull to upper thigh and true whole-body covering the top of the skull to the bottom of the feet, thus underscoring the need to standardize the terminology used in describing PET/CT scan length.
With accuracies ranging from 80% to 90%, 18F-FDG PET diagnoses, stages, and restages many cancers and is often more accurate than anatomic imaging (1). The improvement in accuracy coupled with the convenience of presenting anatomic and functional information to physicians has rendered PET/CT the most important cancer imaging modality at the present time (2). Consequently, by 2006, the major vendors no longer offered PET-only systems, and by mid-2008, more than 3,000 combined PET/CT systems were in clinical operation worldwide (3). Furthermore, the use of PET/CT has been advocated as a first-line imaging modality for whole-body tumor staging, restaging, and assessing response to therapy in different types of cancer (4). However, the term whole body for anatomic scan length remains misleading because the most commonly used field of view (FOV) for PET/CT whole-body protocols covers only the base of the skull to the upper thighs and does not include the brain, skull, or significant portions of the upper and lower extremities. To our knowledge, no data are available on variations in the selected FOV for 18F-FDG PET/CT. The objective of the current study was to evaluate variations in FOV and arm positioning and to categorize each FOV into anatomic scan length variants at both private and university settings, all claiming to use PET/CT whole-body protocols.
MATERIALS AND METHODS
Patients and Sites
The current study was performed in the state of Missouri. According to the American Cancer Society, the most prevalent cancers in the state of Missouri include lung, breast, prostate, and colon. The remaining population of cancer patients accounts for a small percentage and includes those with melanoma, urinary bladder cancer, non-Hodgkin lymphoma, and other types of cancer (uterine, cervical, and leukemia). These data suggest that the population of cancer patients in the state of Missouri is comparable to the national average (5). Two hundred patients referred for clinical evaluation of known or suspected cancer who had undergone PET/CT at 1 of 4 sites were retrospectively evaluated between June and December of 2004 for anatomic FOV. Patients fasted at least 4 h before the PET acquisition and received an intravenous injection of 18F-FDG. Blood glucose level was measured immediately before 18F-FDG injection and was less than 200 mg/dL. Patients were seated for the subsequent 45–60 min of the 18F-FDG uptake phase and were allowed to breathe normally, without specific instructions, during image acquisition. Low-dose CT data were used for image fusion and the generation of a CT transmission map. No oral or intravenous contrast material was used.
Private Stationary Site
Fifty patients from a private stationary site were retrospectively evaluated. All 50 scans were acquired using a 2-dimensional PET/CT scanner (Discovery ST; GE Healthcare) with an axial co-scan range of 160 cm after an injection of approximately 7.4 MBq (0.2 mCi)/kg of 18F-FDG, with a maximum dose of 740 MBq (20 mCi).
Two Private Mobile Sites
Fifty patients from 2 private mobile sites, 25 patients from each site, were retrospectively evaluated. All 50 scans were acquired using a Discovery ST scanner with an axial co-scan range of 160 cm after an injection of approximately 7.4 MBq (0.2 mCi) of 18F-FDG, with a maximum dose of 740 MBq (20 mCi).
Stationary University Site
One hundred consecutive patients from a stationary university site, 50 patients before and 50 after implementation of a true whole-body protocol, were retrospectively evaluated. All 100 scans were acquired using a 3-dimensional PET/16-slice CT scanner (Gemini; Philips) with an axial co-scan range of 193 cm after injection of approximately 5.18 (0.14 mCi)/kg of 18F-FDG, with a maximum dose of 444 MBq (12 mCi).
Image Analysis and Data Collection
Whole-body PET/CT images were retrospectively evaluated on either a Xeleris (GE Medical Solutions) or Syntegra (Philips) workstation by a board-certified nuclear medicine technologist. FOV was categorized into 5 anatomic scan lengths: category A, base of skull to upper thigh; category B, base of skull to mid thigh; category C, top of head to upper thigh; category D, top of head to mid thigh; and category E, top of head to bottom of feet (true whole-body) (Fig. 1). A log was kept tallying variations in FOV. All studies were further categorized into 2 patient arm positions: up and down.
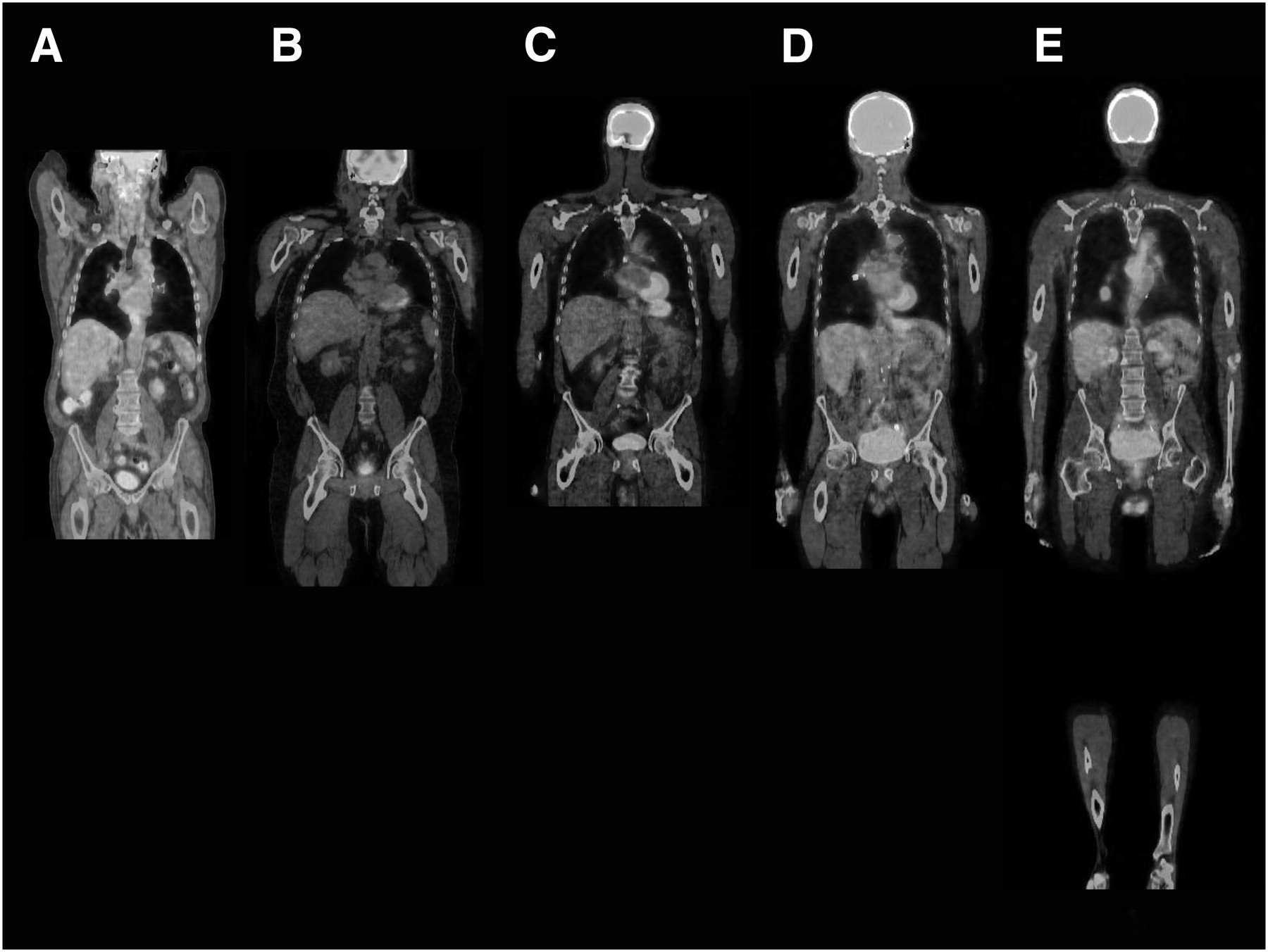
FOVs were categorized into 5 anatomic scan lengths: base of skull to upper thigh (A), base of skull to mid thigh (B), top of head to upper thigh (C), top of head to mid thigh (D), and top of head to bottom of feet (true whole-body) (E). (A color version of this figure is available as a supplemental file online at http://tech.snmjournals.org/.)
RESULTS
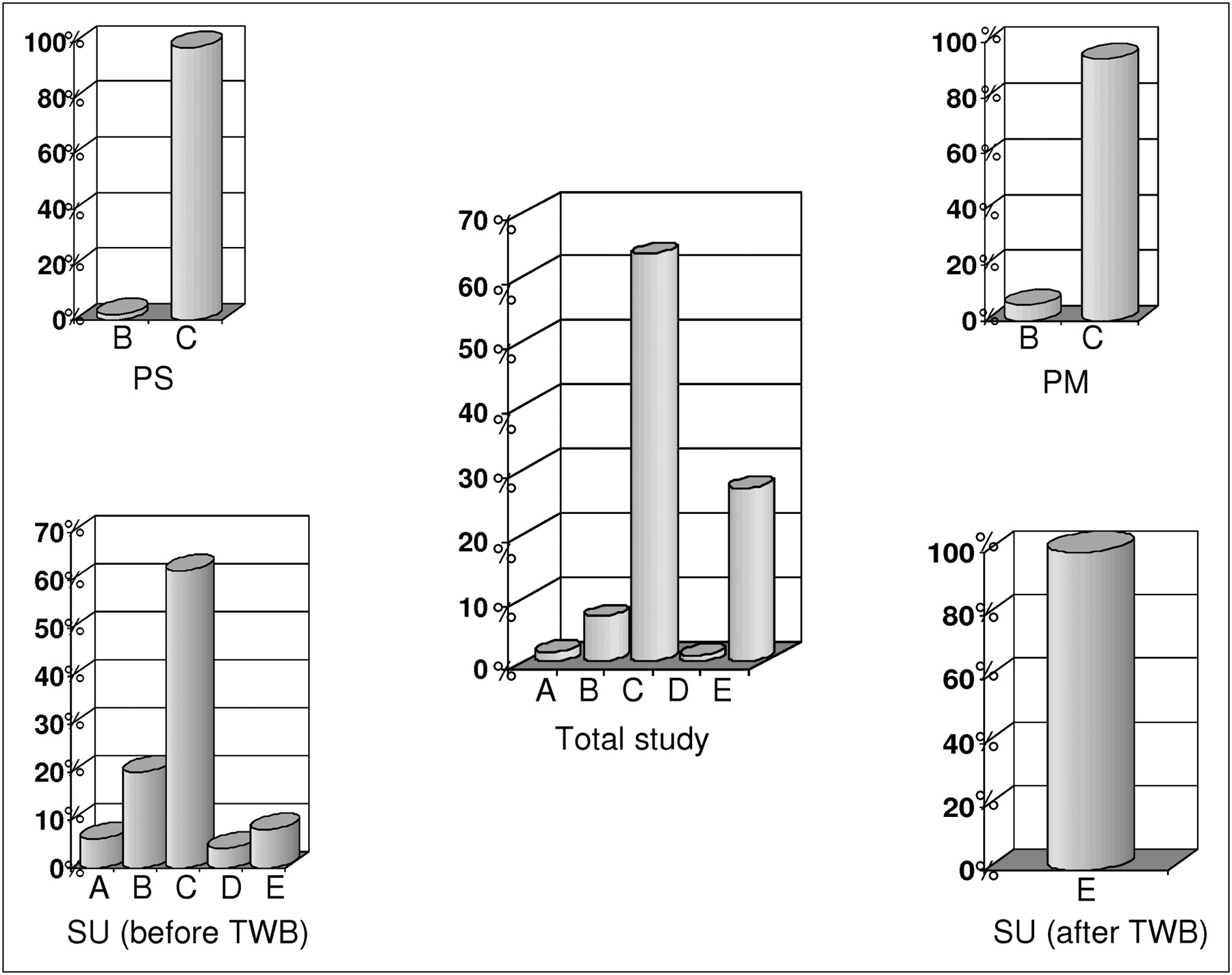
Of the 50 patients from the private stationary site, 98% fell into category C, with the remaining 2% falling into category B. Of the 50 patients from the private mobile sites, 94% fell into category C, with the remaining 6% falling into category B. Of the 50 patients from the university site, before implementation of the true whole-body protocol, 6% fell into category A, 20% into category B, 62% into category C, 4% into category D, and 8% into category E; after implementation, all patients fell into category E. A summation of all 200 studies found that 1.5% were category A, 7% category B, 63.5% category C, 1% category D, and 27% category E (Fig. 2).

Percentages of patients scanned in the 5 anatomic scan length categories: category A, 27%; category B, 1%; category C, 63.5%; category D, 7%; and category E, 1.5%. PM = private mobile site; PS = private stationary site; SU = stationary university site.
At the private stationary site, patients’ arms were down 100% of the time. The private mobile sites had patients’ arms up 72% of the time and down 28% of the time. The university site before implementation of the true whole-body protocol had patients’ arms up 54% of the time and down 45% of the time. The same site after implementation of the protocol had patients’ arms up 58% of the time and down 42% of the time. Overall, patients’ arms were up 46% of the time and down 54% of the time (Fig. 3).
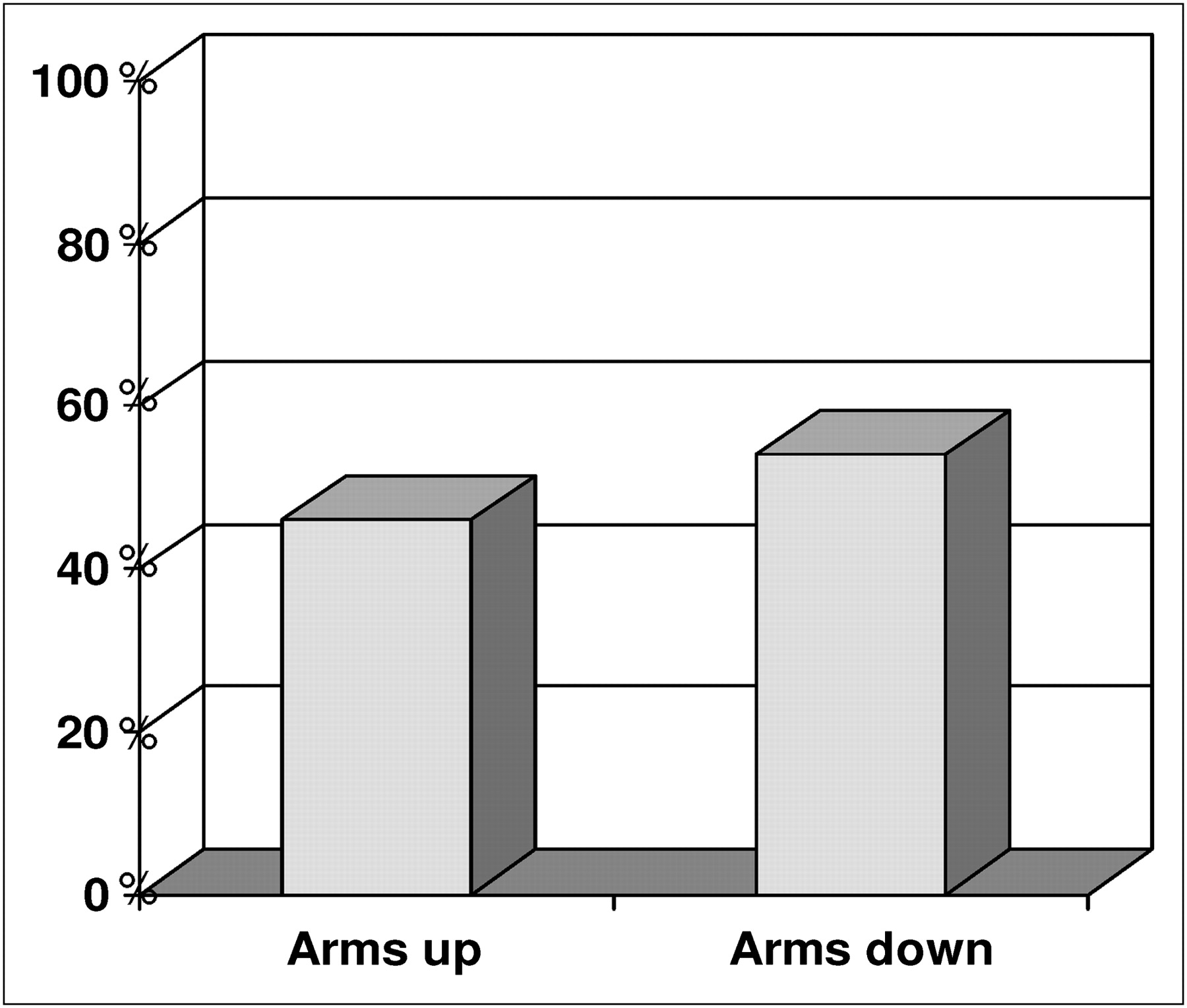
Summary of arm positions in all studied centers. Patients’ arms were up 46% of the time and down 54% of the time during scanning.
DISCUSSION
In the late 1990s, Townsend's group pioneered the concept of near-simultaneous imaging of molecular and anatomic information (6,7). Since then, numerous studies have shown that this whole-body dual-modality imaging is better than PET or CT alone for staging and restaging most cancers (2). However, the FOV for the widely used whole-body PET/CT of cancer patients is still not standardized. In oncology, the most commonly used FOV for arms-up PET/CT whole-body protocols covers only the head to the pelvic floor, the so-called eyes-to-thighs or lips-to-hips protocol (8). Such an FOV may underestimate the true extent of the malignancy. To underscore this same issue, Wagner raised the question of what is meant by whole-body imaging during both his 2004 and his 2005 Society of Nuclear Medicine highlights lectures (9,10). Thus, both Dr. Wagner's presentation and the current study's results show that the term whole-body is somewhat misleading because it does not include the brain, skull, or significant portions of the upper and lower extremities, and the FOV used in each “whole-body” acquisition varies not only by type of cancer but also by institution. In this study, we included both mobile and fixed sites, as well private and academic sites. In so doing, we aimed to provide a true representation of variation in selected FOV in various settings for PET centers (Fig. 1).
Searches for the phrases WB FDG PET and whole-body FDG PET on PubMed (title and abstract, limited to humans) produced 1,715 references in November 2009. It is likely that the term WB in these references rarely meant true whole-body. The axial co-scan range is vendor-dependent; however, both anatomic scan length and imaged FOV are selected by the PET/CT center on the basis of axial co-scan range, capability of the scanner, and type of cancer being evaluated. Currently, the co-scan range for combined CT and PET is approximately 145 cm for most of the PET/CT scanners offered by major vendors of medical imaging equipment (11). Therefore, true whole-body PET/CT may require 2 separate acquisitions with timely patient repositioning in between. This hardware and software limitation would explain the reluctance to perform true whole-body imaging and thus may lead to use of the misnomer whole-body when a limited eyes-to-thighs protocol is actually performed.
At the university site, the Gemini PET/CT scanner has a unique axial co-scan range of 193 cm in a single sweep, thus enabling the operator to acquire true whole-body images from the top of the skull to the bottom of the feet in most patients (patient height being the outstanding issue). In a previous clinical study from this same site, true whole-body image acquisition revealed the presence of new, previously unidentified malignant sites outside the typical limited whole-body FOV in 4% of patients (12). The detection of those sites had a direct impact on patient management through upstaging and detection of new secondary primaries. Despite the obvious benefit, adopting true whole-body instead of limited whole-body PET/CT of cancer patients is not without a price. Scanning time increases by 30%–40%; thus, the daily clinic schedule needs to be reduced at no additional compensation. Furthermore, although the 18F-FDG dose is kept the same, the radiation dose to the patient from the low-dose, unenhanced CT is slightly higher because additional portions of the body are included.
Effective January 1, 2005, the current procedural terminology codes of the Centers for Medicaid and Medicare Services were changed from a single code blanketing all oncology PET protocols to 6 distinct codes specifying 3 varying FOVs, as well as differentiating between PET and PET/CT (Table 1). The implementation of these codes was an important stride toward the standardization of protocol terminology.
Current Procedural Terminology Codes for Oncology PET Protocols
In our study, in addition to nonstandardized FOVs for whole-body protocols, a lack of standardization was found for patient arm position. In oncology, the arms should be elevated over the head except in head and neck cancers, for which arms should be positioned along the side (13). Often, because of patient body habitus and scanner aperture diameter alone, scanning with arms down may not be physically achievable. Yet when a choice is available between arms up or arms down, the decision depends on several factors. Scanning with the patient's arms up optimizes abdominal and thoracic imaging by alleviating possible attenuation, truncation, and streak artifacts due to shadowing of the arms (14,15). Inversely, having the arms up may cause artifacts in images of the skull, neck, and upper thorax, as well as putting strain on the patient's arms and shoulders, possibly resulting in unwanted patient motion. Scanning with the patient's arms down optimizes skull, neck, and shoulder imaging and ensures greater patient comfort, limiting artifacts due to motion, yet may cause artifacts over the thorax and abdomen, often making interpretation of adrenal gland involvement difficult. In addition, positioning of the arms up may remove portions of the forearm, wrist, and hands from the FOV. Finally, with advancements in the hardware and software of newer PET/CT scanner designs, the time required for true whole-body acquisitions will continue to decrease and the co-axial scan range will continue to expand. For example, we are currently using a 64-slice PET/CT scanner with time-of-flight technology, which enables us to acquire a true whole-body scan in 20 min in patients with a normal body mass index. Of importance, the Medicare reimbursement rates for limited whole-body imaging and true whole-body imaging have equal technical fees ($1,037.34) and a difference of only $2.94 in professional fees ($124.80 vs. $127.74). Data from the National Oncologic PET Registry showed that 18F-FDG PET changed management for 38% of cases (95% confidence interval, 37.6%–38.5%) across cancer types, proving that the use of PET should not be restricted to cancer type or testing indication (16). One might argue that the selected FOV in the whole-body 18F-FDG PET scans of the National Oncologic PET Registry data varied by participating PET center and that such variation and its impact on the final analysis is yet to be determined. A recent follow-up publication revealed that the PET FOV was not mentioned in 8.4% of PET/CT reports evaluated by the National Oncologic PET Registry (17).
The scope of this retrospective study, limited to assessing variations in the FOV selected for whole-body 18F-FDG PET/CT, did not aim at analyzing diagnostic significance. Furthermore, data on FOV variations were collected from a limited number of sites, all from a single geographic location. For example, the percentage of true whole-body imaging is likely overestimated in this study because of the university site's routine use of true whole-body imaging as the standard of care. However, the purpose of this study was to document the variation rather than accurately estimate the percentage of each FOV.
CONCLUSION
Although each site claimed to use a whole-body protocol, the results indicate several variations in FOV. With 63.5% of patients found to be scanned from eyes to thighs, one might assume that most sites accept such a definition for whole-body PET/CT. Yet when an order is received for a whole-body bone scan versus a limited bone scan, there is little question as to the FOV desired. Whole-body 18F-FDG PET/CT should mirror this standardization of whole-body bone scanning. The current procedural terminology codes distinguish between the various types of billable scan lengths; following this terminology should aid in the standardization process.
REFERENCES
- Received for publication November 30, 2009.
- Accepted for publication May 10, 2010.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.