


Abstract
PET is a molecular imaging modality used to assess metabolic activity. Little is known about the physiologic uptake of radiopharmaceuticals such as 18F-FDG in healthy subjects. This study was designed to identify and describe normal patterns of physiologic uptake of 18F-FDG in healthy adult subjects and to examine the influence of low-level muscle activity during the 18F-FDG uptake phase. Methods: Twenty healthy adults received an intravenous injection of 18F-FDG and were subsequently scanned with a combined PET/CT scanner. The CT scan was used to accurately identify the location of 18F-FDG uptake. Of the 20 subjects, 10 were randomly selected to perform a low-level muscle activity during the 1-h 18F-FDG uptake phase. The PET/CT images were fused, and the location and intensity of metabolic activity were described for all subjects. Results: Muscle activity during the 18F-FDG uptake phase affected the pattern of 18F-FDG distribution on PET scans. In addition, the tissue uptake of 18F-FDG, although variable, showed some consistency among tissue types. Conclusion: The data suggested that technologists should be aware of low-level muscle activity before and during uptake to avoid potential false-positive interpretations. The data also showed that there is some variability in the normal physiologic uptake of 18F-FDG across subjects. Finally, the results suggested that 18F-FDG uptake may be used for the evaluation of muscle activity.
PET is a molecular imaging modality used for the in vivo assessment of metabolic activity. Positron-emitting radiopharmaceuticals, such as 18F-FDG, permit the localization of metabolically active tissues, including tumors. Consequently, 18F-FDG PET has been widely accepted as a standard tool in cancer imaging. In oncology, whole-body (WhB) PET is typically performed from the eye level to the pelvic floor (1,2). The use of the term WhB is misleading because the most commonly used field of view (FOV) for “arms-up” PET WhB protocols includes only the base of skull to the upper thighs; the brain, skull, and significant portions of both upper and lower extremities are not included. This routinely used FOV results in limited knowledge about normal physiologic metabolic activity in a significant percentage of the body as well as potential underestimation of the true extent of disease because of missed metastases to areas outside those covered by typical limited WhB scans. Initial studies documenting the added value of true WhB (TWhB) 18F-FDG PET in some types of cancers are beginning to appear in the literature (3,4). Recent studies (4–6) showed that up to 8% of cancer lesions are missed with a truncated scanning field. The authors of these studies recommended the use of TWhB scans, from the tip of the head to the tip of the toes, as allowed by the scanner.
One challenge in TWhB PET is correctly differentiating uptake that is abnormal (true-positive result) and potentially pathologic from uptake that is physiologic and not associated with pathology (false-positive result). The fusion of PET scanning and CT scanning has improved the anatomic localization of PET abnormalities (7). However, few descriptions of the patterns of normal uptake of 18F-FDG in nonpathologic tissues are available. Yeung et al. (8) reported increased uptake of 18F-FDG in skeletal muscle and adipose tissue in the neck and shoulder regions. These authors stressed that recognition of this normal uptake is critical in avoiding false-positive interpretations. Recently, Jackson et al. (9) conducted a retrospective review of 1,164 PET scans of patients. According to the study, “A total of 146 of 1,164 patients (12.5%) had excessively increased muscle uptake detected on the PET scan that corresponded to the technologists' notes of muscle activity during the uptake phase or before 18F-FDG injection” (9). The authors concluded that awareness of muscle activity before or during uptake should be noted by technologists and reported to physicians to decrease the likelihood of false-positive readings.
Kilgore and Watson (10) also described “incidental, nontarget skeletal muscle uptake” in a series of 18F-FDG PET scans. These authors suggested that certain activity in patients during uptake resulted in the unexpected PET findings. Gradinscak et al. (11) described a case report in which asymmetric 18F-FDG uptake was visualized in the right upper extremity of a patient who had non-Hodgkin lymphoma. These authors found that 2 d before the examination, the patient had spent a few hours working in his garden, and they proposed that the increased uptake in the patient's dominant arm was a result of this muscle activity. Osman et al. (12) examined the TWhB scans of 70 patients with pathologically proven melanoma or non–small cell lung cancer and found physiologic uptake at the femoral origin of the anterior cruciate ligament, plantar fascia, subtalar joint, crural anterior compartment muscles, and vasculature of the lower extremity.
There are 2 concerns about the previous studies on the physiologic uptake of 18F-FDG. First, those studies were all retrospective, and second, the data were from patients with known or highly suspected cancer. No prospective study on the physiologic uptake of 18F-FDG in healthy subjects has been published. 18F-FDG PET was used to examine metabolic muscle activity in healthy subjects during running (13–15), walking (16), and bicycle exercise (17,18). These studies showed that PET can be useful as an alternative technique for evaluating muscle activity on the basis of muscle glucose uptake. However, images were acquired on dedicated PET systems in these studies and therefore lacked the definitive anatomic correlation currently available with modern PET/CT scanners.
In summary, more information about normal physiologic glucose uptake in PET is needed to better differentiate abnormal findings. One major advantage of combined PET/CT is precise anatomic location of areas of increased uptake of 18F-FDG.
The purposes of this research were to identify and describe normal patterns of physiologic uptake of 18F-FDG in healthy adult subjects with PET/CT and to examine the influence of low-level muscle activity during the 18F-FDG uptake phase.
MATERIALS AND METHODS
This study was approved by the Saint Louis University Institutional Review Board, including a review by the institution's Radiation Safety Committee. Healthy adult subjects were recruited to undergo a combined PET/CT TWhB scan. To be included in the study, subjects were required to be healthy ambulatory adults between the ages of 30 and 65 y. Exclusion criteria were ages under 30 y old or over 65 y old; obesity (body mass index of >30 kg/m2); height exceeding 1.8 m (6 ft) (scanner size limitation); inability to voluntarily contract muscle; personal history of cardiac, pulmonary, muscular, skeletal, or metabolic disease; cancer history; pregnancy; or lactation. The purposes and potential risks of the study were explained to the subjects, and their questions were answered. Informed consent was obtained, and the rights of the subjects were protected. If no exclusion criteria existed, each subject completed a personal health history form and was scheduled for a PET/CT scan. Scans were provided at no cost to the subjects. All scanning was done in the summer months to avoid the problem of uptake in brown adipose tissue, which is more commonly seen in colder months as a nonshivering mechanism for generating heat (19).
Scanning Preparation
Patients fasted for at least 4 h before tracer injection and received an intravenous injection of 18F-FDG at approximately 5.18 MBq/kg (0.14 mCi/kg), with a maximum of 444 MBq (12 mCi). The blood glucose level was measured immediately before 18F-FDG injection and was less than 200 mg in all studied patients. Subjects were instructed to sit in a comfortable chair for 45 min before the scan. The 20 subjects were randomized into 2 groups, a control (resting) group and a low-level exercise group. The 10 subjects in the control group remained completely at rest during the 45-min uptake phase. The other 10 subjects were randomly assigned to 1 of 2 tasks: 20 repetitions of active ankle dorsiflexion or plantar flexion with the dominant leg every 2 min for the first 20 min after the injection or 20 repetitions of dominant-hand finger drumming every 2 min for the first 20 min after the injection. These activities were chosen to simulate “nervous activities” that are observed in some patients during the rest time before PET. All subjects were under observation during the entire uptake phase to ensure compliance with the assigned motor tasks or rest. All scans were acquired with a PET/CT scanner (Gemini; Philips) that had an axial coscan range of 193 cm, enabling head-to-toe (TWhB) imaging in one sweep in subjects less than 1.8 m (6 ft) tall.
CT
The CT portion of the PET/CT scanner consisted of a 16-slice multidetector helical CT scanner. The gantry allowed for a patient port of 70 cm. The parameters for 12 or 13 bed acquisitions (from the top of the head to the bottom of the feet) were as follows: 120–140 kV and 33–100 mAs (based on body mass index), 0.5 s per CT rotation, pitch of 0.9, and 512 × 512 matrix. CT acquisition was performed before emission acquisition. CT data were used for image fusion and generation of a CT transmission map. For all patients, arms were placed at their sides. No oral or intravenous contrast medium was used. No separate CT interpretation was performed because the CT scan was of suboptimal quality.
PET
Emission data were acquired for 12 or 13 bed positions (193-cm coverage, identical to CT protocol). Emission scans were acquired at 3 min per bed position. The FOV for all patients was TWhB. The 3-dimensional TWhB acquisition parameters were as follows: 128 × 128 matrix, 18-cm FOV, and 50% overlap. Processing was done with the 3-dimensional row-action maximum-likelihood algorithm method.
Image Analysis
TWhB PET/CT images were evaluated on a Syntegra workstation (Philips) by both investigators for regions of increased physiologic uptake, and uptake regions were anatomically localized by use of the PET/CT fusion images. The investigator who was a board-certified nuclear medicine physician was masked with regard to group assignment in the reading of the scans. 18F-FDG uptake was classified as intense, moderate, or mild on the basis of the expert opinion of the nuclear medicine physician.
RESULTS
Twenty apparently healthy adults (16 women and 4 men) volunteered to participate in the study. All subjects completed the scanning protocol without any adverse events. The characteristics of the subjects, organized by experimental groups, are shown in Table 1]. There were no significant differences in the characteristics of the subjects between the 2 groups.
Subject Characteristics
Table 2 shows the results for organ uptake. 18F-FDG uptake was consistently observed in the brain, heart, kidneys, and bladder. These results were expected on the basis of the metabolic activity of the brain and the heart, as well as the clearance of 18F-FDG through the urinary system. Mild uptake was observed in the liver and spleen in all subjects and in the testicular tissue in males, and most subjects exhibited mild colon uptake. Inconsistent mild to moderate uptake was observed in the parotid gland, stomach, and lymphatic tissues. Diffuse mild breast uptake was noted in some subjects; focal moderate or equivocal uptake was noted in one subject. Concordant with the study protocol, this subject's personal physician was notified of the findings; subsequent mammography results were negative.
Organ Uptake of 18F-FDG
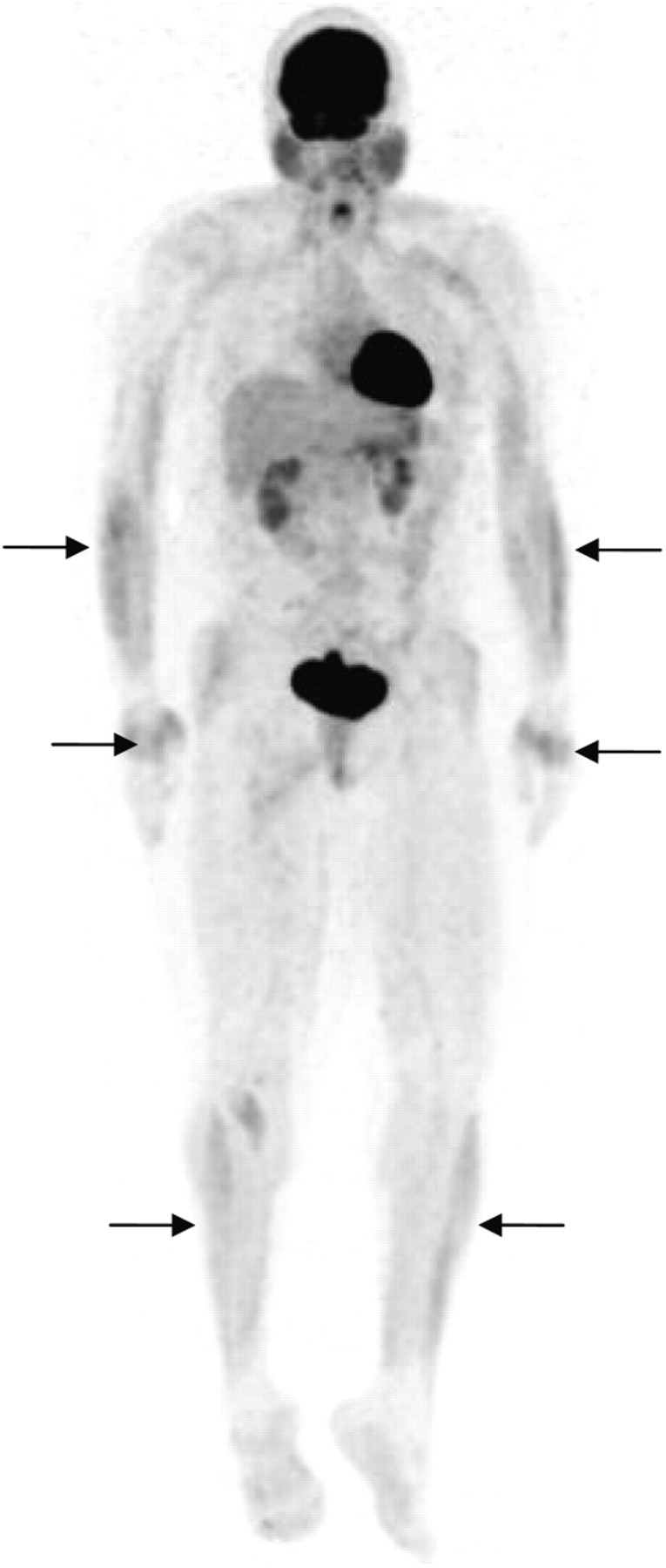
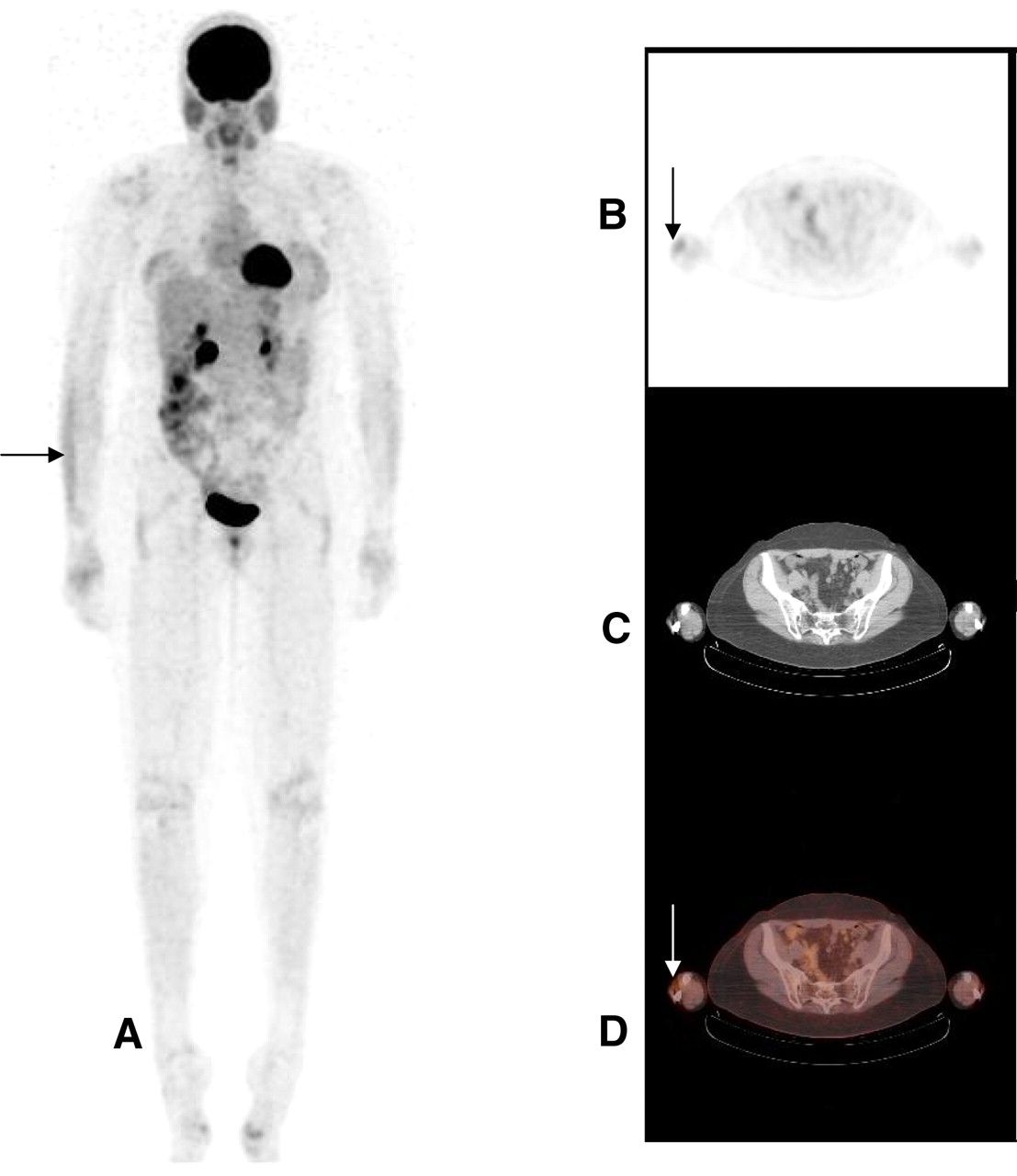
The muscle activity results are shown in Table 3. 18F-FDG uptake was common in the following muscle groups: the vocal cords, the wrist or finger extensor muscles in the posterolateral compartment of the forearm, and the ankle dorsiflexor muscles in the anterior compartment of the leg. All of these muscle groups are routinely involved in activities of daily living, including speaking, grasping and holding, and gait. Figure 1 shows an example of symmetric muscle uptake in a control subject. All subjects were questioned before the scans about any moderate to strenuous physical activity in the preceding 48 h. Among the 10 control group subjects, asymmetric 18F-FDG muscle uptake was observed in 6 subjects—5 with uptake in the wrist or finger extensor muscle group in the forearm and 1 with uptake in the anterior compartment of the leg. Images of one of the control subjects with asymmetric muscle uptake in the wrist or finger extensor muscle group are shown in Figure 2. None of the subjects reported any moderate to strenuous activity involving the observed muscle groups in the 48 h before scanning.
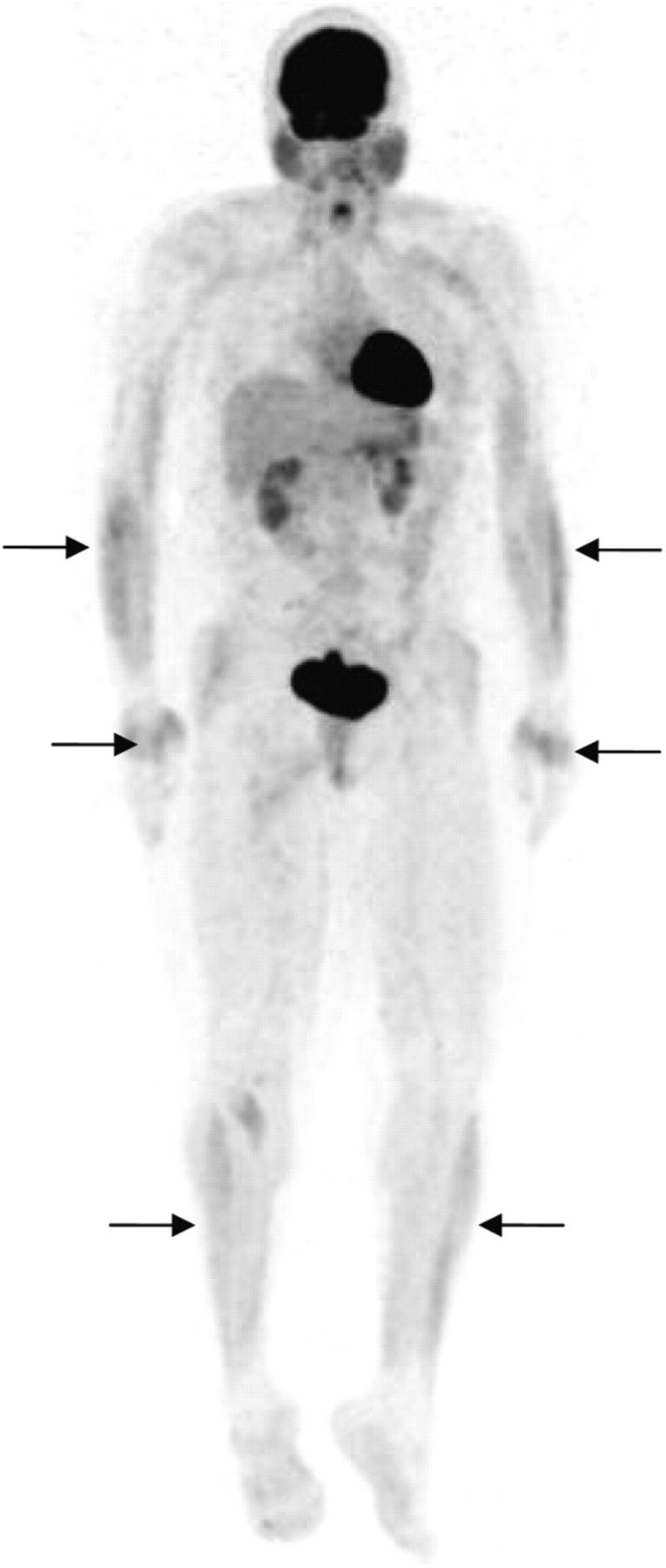
Representative 8F-FDG PET scan in coronal view of symmetric muscle uptake in forearms (arrows), hands (arrows), and anterior crural compartments (arrows) in control subject.
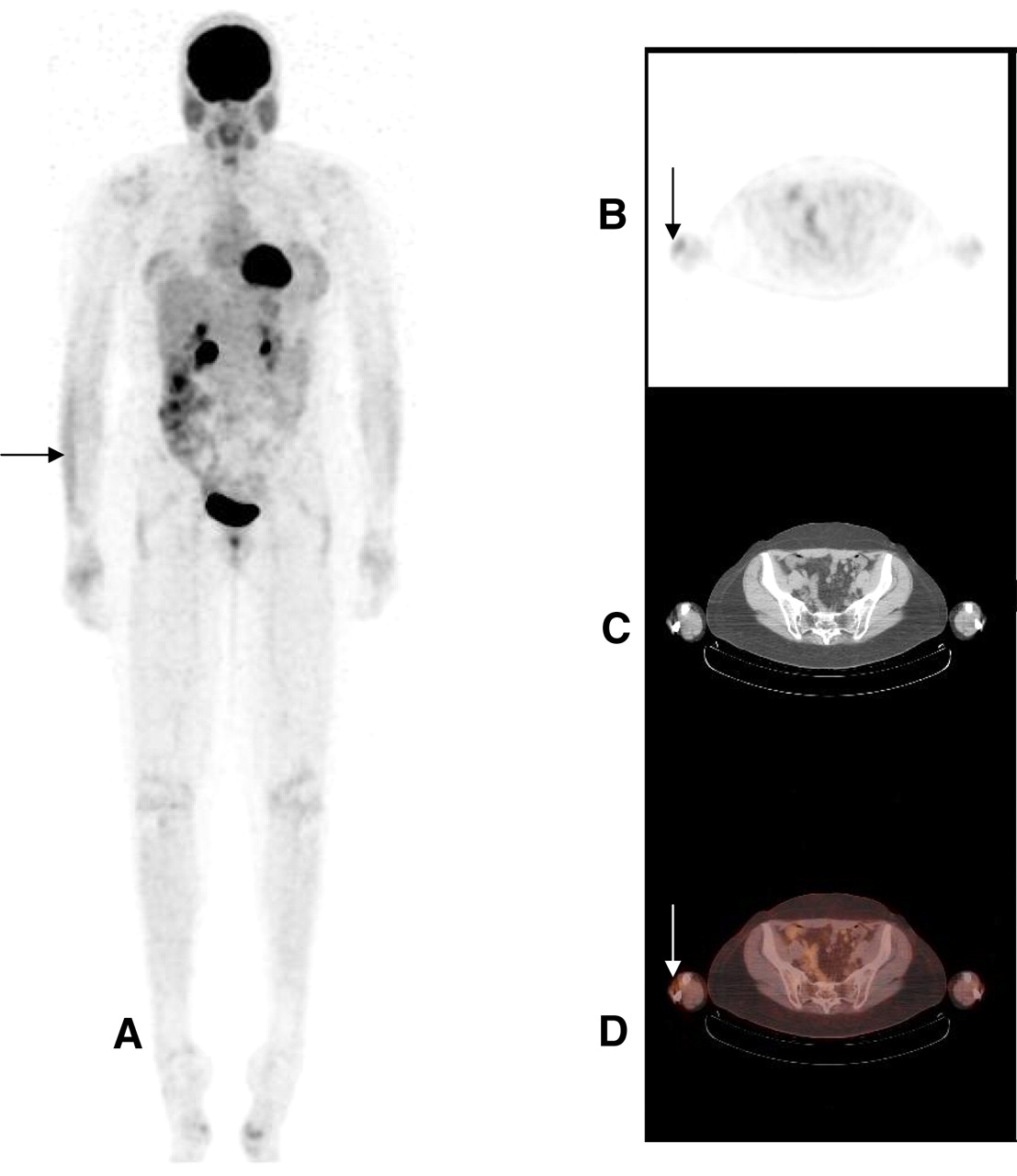
Representative 18F-FDG PET scan in coronal view (A) and transaxial view (B) of asymmetric muscle uptake in wrist or finger extensor muscles (arrow) in control subject. (C) Transaxial CT image used for muscle identification. (D) Fused PET/CT image showing asymmetric muscle uptake in wrist or finger extensor muscles (arrow).
Muscle Uptake of 18F-FDG Across Subjects
The 10 subjects who performed low-level muscle activity during the uptake phase had interesting scan results. Of the 10 subjects, 8 had asymmetric scan results for the involved muscle groups. One subject assigned to each of the 2 activities—ankle pumping and finger drumming—showed no difference in muscle uptake between the active and inactive sides. Although 4 of the 5 subjects assigned to finger drumming showed some differences between the active and inactive forearms, the differences were generally minor and similar to the differences observed between the forearms of several control subjects. An example of obvious asymmetric muscle uptake associated with ankle pumping is shown in Figure 3.
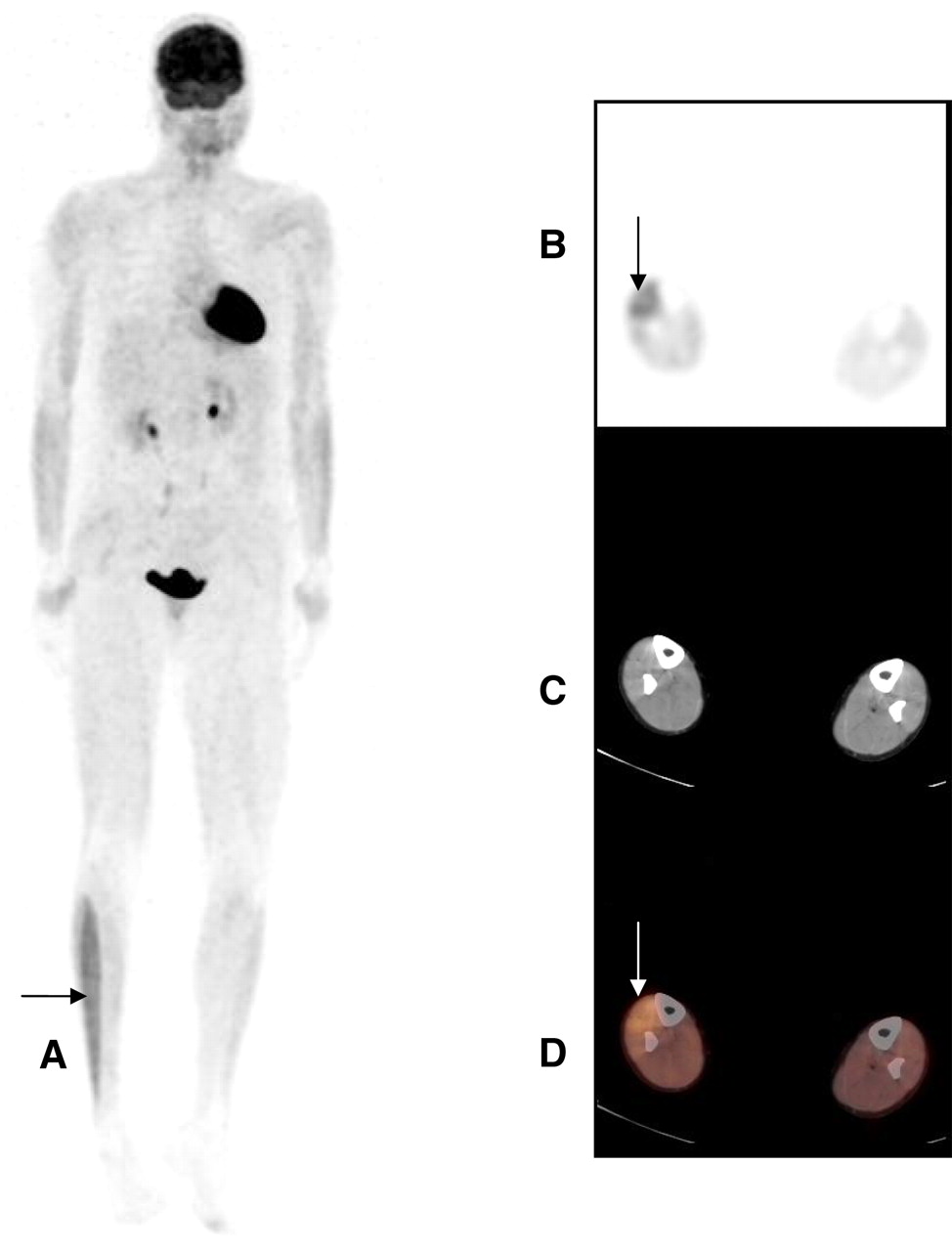
Representative 18F-FDG PET scan in coronal view (A) and transaxial view (B) of asymmetric muscle uptake in anterior crural compartment (arrow) in subject in activity group. (C) Transaxial CT image used for muscle identification. (D) Fused PET/CT image showing asymmetric muscle uptake in anterior crural compartment (arrow).
DISCUSSION
The purposes of the present study were to investigate the physiologic uptake of 18F-FDG in healthy adult subjects and to examine the influence of asymmetric low-level muscle activity during the 18F-FDG uptake phase. After intravenous injection, 18F-FDG is rapidly taken up into tissue and, over a period of 1 h, is trapped in proportion to the rate of glucose metabolism. The normal 18F-FDG distribution includes the brain, heart, kidneys, bowel, and urinary tract. Approximately 6% of the injected dose is taken up by the brain, 4% is taken up by the myocardium, and 20% is taken up by the bladder (20). In our study, organ uptake in all subjects was as expected on the basis of metabolic activities or physiologic clearance, with the uptake being most intense in the brain and bladder, moderate to intense in the kidneys, and variable in the heart. Uptake in the myocardium was variable but typically lower in the fasting state than in the nonfasting state. In accordance with our standard protocol, subjects were asked to fast for at least 4 h before imaging; however, uptake was intense in 13 of 20 subjects (65%). This percentage is higher than the previously reported 20% of patients undergoing PET/CT and showing homogeneous myocardial uptake (21). The consistently mild uptake in the liver and spleen was as expected. Furthermore, the variable uptake and intensity in bowel, parotid gland, testicular, vaginal, breast, and stomach tissues also were as expected. The false-positive breast uptake in one subject underscores a potential risk of using 18F-FDG PET as a screening test in healthy subjects. Understandably, 18F-FDG PET may detect subclinical cancers in some individuals; however, its use as a screening tool should be limited to high-risk patients (22).
The muscle activity component of the present study revealed several interesting findings. Asymmetric muscle uptake was observed in some individuals who were inactive during the uptake phase and who denied any moderate to strenuous activity in the 48 h before scanning. This result was not related to handedness. There are 2 possible explanations for this asymmetric uptake. First, factors other than activity during or before the uptake phase can influence muscle uptake. Second, it is possible that the subjects were performing unintentional low-level muscle activity during the uptake phase, although this possibility is unlikely because the subjects were observed throughout the uptake phase by a research assistant.
Most subjects who performed low-level muscle activity showed asymmetric uptake, that is, uptake in the muscles that were active during the motor task. Both upper- and lower-extremity motor tasks were low-level activities and did not involve the application of external resistance. These activities were chosen to simulate unintentional nervous activities that patients may perform during the uptake phase. Even with such low-level muscle activity, asymmetric muscle uptake resulting in increased areas of metabolic activity was observed. These findings are consistent with the results of retrospective research by Jackson et al. (9); in that study, 18F-FDG muscle uptake was identified as a result of patients' activities during the uptake phase.
18F-FDG uptake was observed in the anterior leg compartment in 11 of the 20 subjects, including 4 of the 5 subjects who performed ankle dorsiflexion and plantar flexion and 7 of the remaining 15 subjects. The anterior compartment includes the tibialis anterior and toe extensor muscles. These muscles are active during walking and running (13,15,16) because they decelerate the movement of the foot to the ground after initial heel contact, and they also function concentrically to bring the foot into dorsiflexion during the swing phase of gait. Because all subjects ambulated independently into the clinic for their PET/CT scans, anterior compartment muscle activity occurred in all subjects immediately before the scans. We speculate that most of the subjects probably would not have identified walking into the clinic as a moderate to strenuous physical activity, but all subjects had engaged in some degree of walking, although the distance walked and the pace of walking were variable. Normal gait is a symmetric bilateral activity; therefore, we would expect bilateral 18F-FDG uptake as a result of gait activities. Ten of the 11 subjects with anterior compartment uptake showed bilateral uptake.
One other issue regarding the pattern of muscle uptake with active ankle motion was the conspicuous absence of posterior calf muscle uptake. The subjects performed ankle motion while sitting in a recliner chair. The motion of dorsiflexion was against gravity and therefore required a concentric contraction of the anterior compartment muscles. However, the movement into plantar flexion was assisted by gravity and therefore did not require active contraction of the plantar flexor muscles; instead, it required eccentric contraction of the dorsiflexor muscles. The same was true of the upper-extremity task, in that wrist and finger extension was performed against gravity and wrist and finger flexion was assisted by gravity.
In their retrospective review of 1,164 18F-FDG PET scans of patients with known or suspected cancer, Jackson et al. (9) reported that 12.5% of patients had muscle uptake of 18F-FDG. The most common sites of uptake were the head and neck, followed in incidence by the chest wall, forearms, hands, and legs. These researchers recommended that patients be contacted a minimum of 48 h before a PET scan and advised to refrain from significant physical activity until the scan is completed. They also recommended that technologists instruct patients to minimize all muscle activity during the uptake phase. The results of the present study agree with those reported by Jackson et al. (9), although our findings suggested that muscle uptake sometimes cannot be explained by patients' recollection of muscle activity.
Bojsen-Moller et al. (23) studied the effect of low-intensity tensile loading on the uptake of 18F-FDG in the Achilles complex. In that study, subjects performed unilateral voluntary ankle plantar flexion at approximately 13% of the maximal voluntary contraction force. Although the primary purpose of that study was the examination of uptake in tendon tissue, the authors did report and provided representative images of asymmetric 18F-FDG uptake in the plantar flexor muscles. These results coincide with our finding of asymmetric muscle uptake as a consequence of unilateral motor activity. It is not clear, however, why asymmetric muscle uptake was observed in some control subjects.
CONCLUSION
The present study demonstrated that low-level muscle activity during the 18F-FDG uptake phase can affect the pattern of 18F-FDG distribution on PET scans. Technologists should be aware of this effect and should record activities during the uptake phase and report them to the reading physician to avoid potential false-positive interpretations. Furthermore, observation of pathology may be masked by muscle activity in some areas; therefore, it may be necessary for physicians to intentionally instruct patients to avoid nonessential physical activity before and during the uptake phase to appropriately visualize potential pathology. The results of the present study also showed that there is significant variability in the normal physiologic uptake of 18F-FDG across subjects. Finally, the present study demonstrated the potential kinesiologic use of PET/CT to examine muscle activity associated with motor tasks. However, such scanning must be done with awareness of the radiation exposure that accompanies this imaging modality.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication June 6, 2008.
- Accepted for publication October 30, 2008.





{kind=link}
{kind=link}
{kind=link}