


Abstract
Obesity has reached epidemic proportions in the United States; hence, it is frequently encountered in patients undergoing 18F-FDG PET studies. The purpose of the current study was to present a technologist's perspective on the prevalence of obesity and the challenges and solutions in imaging obese patients in our PET facility. Methods: From October 2002 to October 2003, whole-body 18F-FDG PET was performed on 1,164 patients with a known or suspected malignancy. Images were acquired 45–60 min after 18F-FDG injection (7.4 MBq [0.2 mCi]/kg, with a maximum of 925 MBq [25 mCi]) on a PET scanner using a 4-min emission and 3-min transmission time per bed position. A database was maintained of patient height and weight, and body mass index (BMI) was calculated. Patient obesity was classified as overweight (BMI ≥ 25 kg/m2), obese (BMI ≥ 30 kg/m2), or malignantly obese (BMI ≥ 40 kg/m2). In addition, PET technologists recorded any problems and attempted solutions related to the patient weight. Results: BMI calculations showed that 528 patients (45.4%) were overweight or obese (322 men and 206 women; mean age, 55 y). Of those, 201 (38%) were overweight, 270 (51%) were obese, and 57 (11%) were malignantly obese. Problems encountered in these patients included difficult intravenous access (15%), difficult patient positioning (10%), patient motion (7%), an incomplete study (emission only) (1%), and potentially higher radiation exposure to the technologist because of extra time spent near the patient. Attempted solutions included adjusting the schedule to allow more time per patient, adjusting the dose based on body weight, using varied positioning techniques, dividing the study to allow a respite between different image combinations, and dividing time spent with obese patients among the technologists involved. Conclusion: Excessive body weight and related problems have commonly been encountered in our PET facility. 18F-FDG PET studies of obese patients represent an ongoing challenge, which requires patient-tailored solutions to avoid compromising image quality and risking higher radiation exposure to the technologists.
Most patients imaged in a PET center come for the diagnosis or work-up of cancer and, therefore, can be more challenging than the patients in a general nuclear medicine department. These challenges are related to the disease state and its therapy. Often, patients have additional problems, such as claustrophobia, arthritis, recent surgery, diabetes, anxiety, and obesity. Obesity is currently one of the most important public health problems in the United States. An estimated 65% of U.S. adults are overweight or obese, with 112,000–280,000 deaths annually attributed to obesity (1–3). Imaging obese patients presents several challenges to the technologists acquiring the images and the physicians interpreting them. These challenges have been described for various imaging modalities, including mammography, ultrasound, SPECT, and CT (4–8). PET has become a standard diagnostic tool in the management of cancer patients. 18F-FDG PET is used to diagnose, stage, and restage many types of cancer, with an accuracy that ranges from 80% to 90% and is often better than that of anatomic imaging (9). Obesity in the United States has reached epidemic proportion; therefore, it is frequently encountered in patients referred for 18F-FDG PET evaluation of known or suspected cancer. However, to the best of our knowledge, problems encountered in the imaging of obese patients with 18F-FDG PET have not been reported. The aim of our study was to evaluate the prevalence of obesity in patients undergoing PET in our facility and the challenges and attempted solutions in imaging these patients.
MATERIALS AND METHODS
Patients
From October 2002 to October 2003, 1,164 consecutive 18F-FDG whole-body PET scans were performed in our institution on patients with known or suspected cancer. The technologists recorded the height and weight of each patient. Body mass index (BMI) was calculated (weight in kilograms divided by the square of height in meters), and the presence of excessive body weight was categorized according to the guidelines of the National Institutes of Health, whereby a BMI of 25–29.9 kg/m2 is classified as overweight, 30–39.9 kg/m2 as obese, and 40 kg/m2 or more as malignantly obese (10).
Image Acquisition
All whole-body scans were acquired on a dedicated PET scanner (Advance; GE Healthcare) with a patient port of 60 cm. The patients fasted at least 4 h before the PET acquisition and received an intravenous injection of approximately 7.4 MBq/kg (0.2 mCi/kg) of 18F-FDG, with a maximum dose of 925 MBq (25 mCi). The blood glucose level was measured immediately before 18F-FDG injection and was less than 200 mg/dL in all imaged patients. Patients were instructed to sit in a quiet room without talking during the 45- to 60-min uptake phase after 18F-FDG injection. 68Ge transmission scans were acquired for 3 min per bed position. The transmission scans were acquired to generate an attenuation correction map to correct the emission images. Emission scans were acquired for 4 min per bed position. The field of view was typically from the base of the skull to the mid thigh, with the exception of melanoma patients, who were imaged from the top of the head to the bottom of the feet. The 2-dimensional whole-body acquisition parameters consisted of a 128 × 128 matrix and a 15-cm field of view with a 3-slice overlap. For processing, ordered-subsets expectation maximization was applied, using 21 subsets and 2 iterations.
Data Analysis
The technologists' records for all patients were retrospectively reviewed to select those with a BMI greater than 25 kg/m2, and patients were grouped into the 3 categories of excessive body weight. For those patients, the technologists' records and PET scans were reevaluated and the prevalence and patterns of obesity were tallied. In addition, problems encountered before or after the 18F-FDG injection or during image acquisition, and attempted solutions, were noted and recorded.
RESULTS
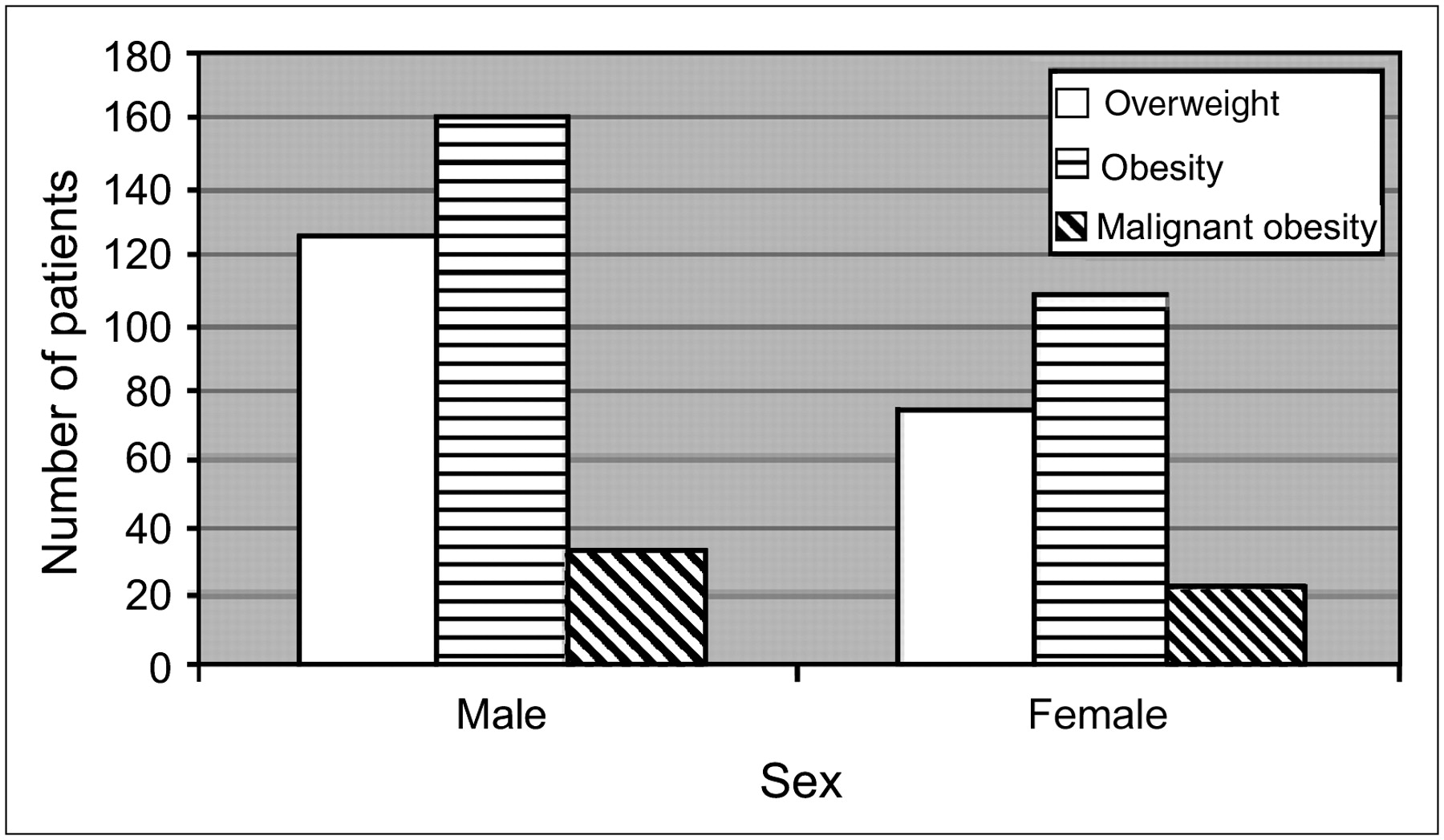
For the 1,164 imaged patients, BMI averaged 27.6 kg/m2 and ranged from 8 to 67 kg/m2. Based on BMI calculations, 528 patients (45.4%) were overweight or obese (322 men and 206 women; mean age, 55 y). Of those, 201 (126 men and 75 women) (38%) were overweight, 270 (162 men and 108 women) (51%) were obese, and 57 (34 men and 23 women) (11%) were malignantly obese (Fig. 1).

Excess body weight by sex.
Problems encountered during the studies included relatively difficult intravenous access (15%), difficult patient positioning (10%), patient motion (7%), an incomplete study (because the patient was uncomfortable on the table, only the emission scan was acquired) (1%) (Fig. 2), and concerns about potentially higher radiation exposure to the technologists because of the longer time spent near the patients during injection or positioning. Although difficult intravenous access was the most frequent problem, patient positioning was the most troublesome. Solving this problem required creativity. The different positioning techniques attempted included arms up (Fig. 3), one arm up (Fig. 4), left decubitus (Fig. 5), prone (Fig. 6), and dividing the study to allow respite between different combinations of bed positions. Other solutions included adjusting the 18F-FDG injected dose and clinic schedule to allow sufficient time for obese patients. Also, in an attempt to equally distribute the radiation exposure, time spent with these patients was divided among the technologists involved.
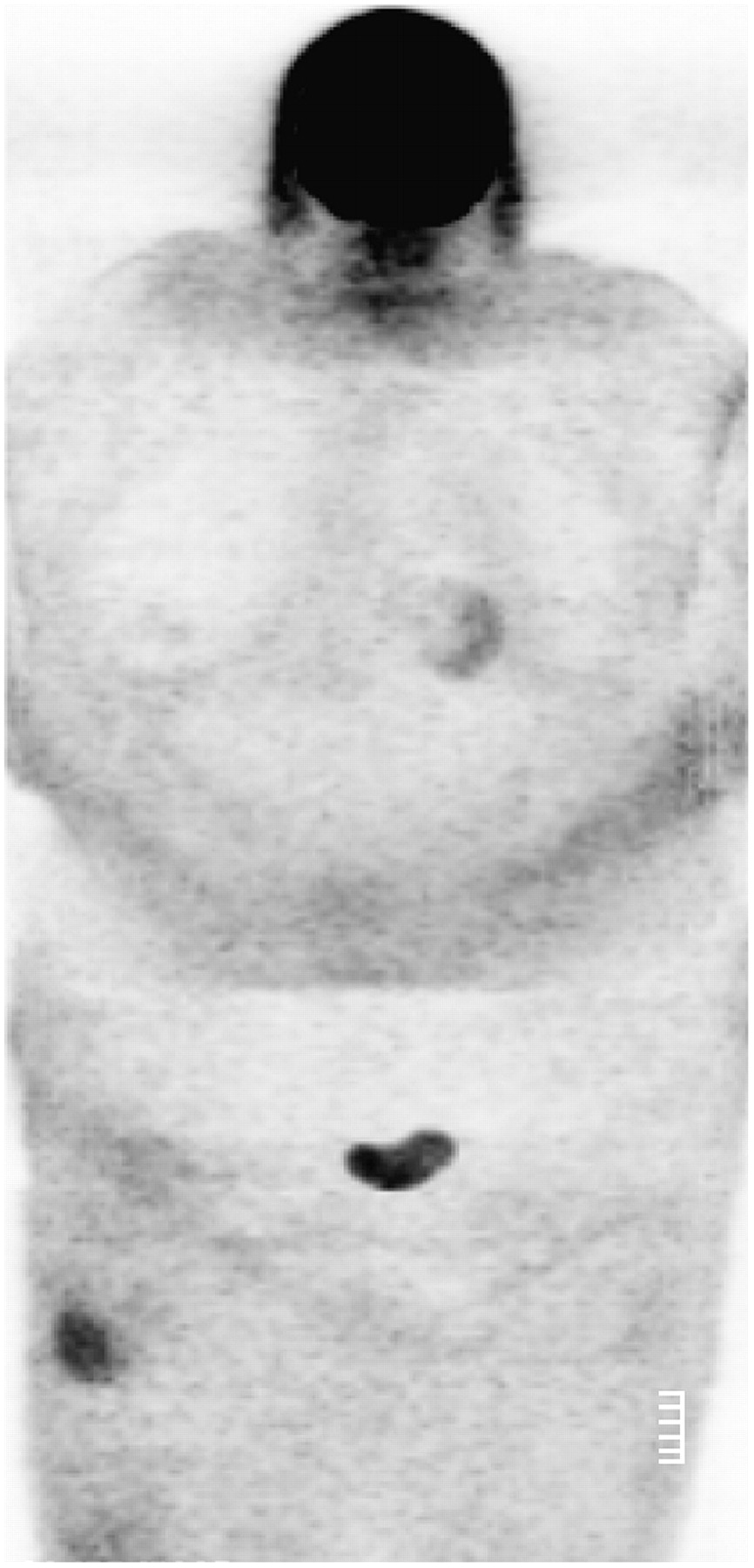
Coronal PET maximum-intensity projection of 132-kg (290-lb) 49-y-old woman (BMI, 42; blood glucose level, 104 mg/dL) with history of melanoma in whom only emission images were obtained. She refused transmission portion of scan because of being uncomfortable.

Coronal PET maximum-intensity projection of 159-kg (350-lb) 50-y-old man (BMI, 48; blood glucose level, 93 mg/dL) with history of melanoma who was imaged with arms up. Images are normally acquired with arms down, but because of body habitus, this patient would fit in scanner only with arms up.

Coronal PET maximum-intensity projection of 158-kg (348-lb) 61-y-old man (BMI, 47; blood glucose level, 165 mg/dL) with history of pancreatic cancer who was imaged with only right arm up because of shoulder pain in left arm.

Coronal PET maximum-intensity projection of 168-kg (370-lb) 51-y-old man (BMI, 52; blood glucose level, 138 mg/dL) with suggestive lung nodule who was imaged in left decubitus position. Images were limited by vast size of this patient's abdomen.

Coronal PET maximum-intensity projection of 170-kg (375-lb) 72-y-old man (BMI, 55; blood glucose level, 98 mg/dL) with lung nodule who was imaged prone with both arms extended over his head. Note heart position.
DISCUSSION
Recently, a large, prospective study revealed that obesity was strongly associated with the risk of death in both men and women in all racial and ethnic groups and at all ages (11). Furthermore, the incidence of obesity is rising in the United States (12). With this increasing incidence, the problem of obesity in the arena of diagnostic imaging is also increasing, as is the number of habitus-limited radiology reports. Regardless of the modality—CT, ultrasound, MRI, or PET—imaging of obese patients may be difficult or even impossible, and images can be suboptimal and difficult to interpret. In cancer patients, the therapeutic options and prognosis strongly depend on accurate imaging that encompasses the entire body. The most challenging aspect of imaging obese patients is ensuring that the entire anatomy can be visualized. Radiation in CT can be limited by inadequate penetration; ultrasound waves may not penetrate a large body, and MRI of obese patients suffers from a low signal-to-noise ratio. Because of higher photon attenuation and scatter fractions in PET of obese patients, image quality is suboptimal to that in patients with a normal BMI. Also, the appropriate 18F-FDG dose may vary depending on the type of crystal and whether the detector is operating in 2-dimensional or 3-dimensional mode. Too much 18F-FDG may increase dead time and decrease image quality. Regardless of the modality or detector type, it is important for each institution to adopt specific protocols for obese patients.
To compensate for the increased BMI, some have advocated that the injected dose or acquisition time be adjusted; however, these strategies typically yield limited improvement and may be difficult to routinely implement. For example, it has been suggested that a 120-kg person should be scanned 2.3 times longer than a 60-kg person to obtain the same signal-to-noise ratio (13). Others have suggested that poorer image quality in larger patients can be overcome by increasing the injected dose in proportion to patient weight (14).
In the current study, we did not adjust the acquisition time; however, the 18F-FDG dose was 7.4 MBq (0.2 mCi)/kg, with a maximum of 925 MBq (25 mCi). Furthermore, the bore size or maximum table weight of the PET scanners may limit the size of patients who can undergo PET scans. In our institution, patient weight and body habitus are investigated up front, by telephoning the patient 24 h before 18F-FDG injection, to ensure that the weight is less than the maximum cutoff limit for the table. Also, before 18F-FDG injection, if we are uncertain that the patient's body habitus meets the parameters of the scanner, we use a hula hoop that matches the 60-cm size of the scanner bore. If the patient can fit through the hoop, then he or she will fit in the scanner.
On the one hand, obesity and being overweight increase the risk of several forms of cancer (15). On the other hand, cancer and its related therapy may lead to weight loss. In our study, obesity was surprisingly present in 45.4% of our studied population. It was also more prevalent in men than women (322 men [61%] and 206 women [39%]) (Fig. 1); however, this difference could be related to selection bias. In these patients, the problems we encountered included difficult intravenous access and patient positioning, an incomplete study, and patient motion. The radiation exposure of technologists is generally higher in PET than in conventional nuclear medicine (16). However, attempted solutions to address the difficulties in imaging obese patients may lengthen the time for which the PET technologist is near the obese patient, compared with a patient with a normal BMI. Thus, the issue of radiation exposure is even more of a concern in acquiring PET images of heavy patients. In our experience, optimal planning of the clinic schedule; enforcement of the time, distance, and shielding rules; and close monitoring of radiation doses help minimize technologists' radiation exposure. Furthermore, patient-tailored solutions may help avoid having to cancel studies, as well as minimize image degradation, although suboptimal images in heavy patients are not uncommon, particularly in those who are malignantly obese (Figs. 2–6⇑⇑⇑⇑).
Malignant obesity is rapidly increasing, particularly in the United States (17). PET/CT now accounts for more than 90% of current PET sales, and further growth in the PET/CT market share is anticipated. Therefore, PET/CT manufacturers are attempting to address the growing market for scanners that accommodate obese patients by increasing the bore size and weight tolerance of the scanners. The first generation of PET/CT scanners had a patient port of 70 cm for CT, tapering to 60 cm for PET, and a maximum body weight of 170 kg (375 lb). Subsequent generations of scanners have a 70-cm patient port for both the PET and the CT portions, and a maximum body weight of 193–204 kg (425–450 lb), thus accommodating not only a heavier weight but also a larger body habitus. Furthermore, researchers continue to optimize imaging protocols for obese patients (18), and new generations of PET scanners promise faster image acquisition, higher intrinsic performance, and potential advantages for the imaging of heavy patients (19).
Our study was not without limitations. First, we did not compare the frequency of the problems encountered in obese patients with the frequency of the same problems in patients with a normal BMI. However, our goal was not to do such a comparison but rather to underscore the growing problem of obesity and related problems in the PET population. Second, our study was limited to PET and did not include PET/CT. In our institution, a similar study regarding obesity and related problems in patients undergoing PET/CT is in progress. Third, we could not tally the 18F-FDG PET studies that were ordered but were not acquired because of prohibitively excessive body weight or habitus; such data were not available. Also, although we acknowledge that these problems do exist in normal-weight patients, we have found the problems to be more frequent in obese patients. Last, the impact of obesity-induced suboptimal PET studies on lesion detectability and diagnostic accuracy was beyond the scope of the current study.
CONCLUSION
Overweight and obesity were commonly seen (45.4%) in our studied population. 18F-FDG PET of obese patients represents an ongoing challenge, which requires patient-tailored solutions to minimize compromised image quality. Advancements in both the hardware and the software technology of newer PET/CT scanners are needed to cope with the obesity epidemic in the United States.
Acknowledgments
We thank technologists Penny Yost and Stephanie Anastas for their technical support.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 19, 2006.
- Accepted for publication February 15, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}