


Abstract
Objective: The use of 18F-FDG for clinical PET studies increases technologist radiation dose exposure because of the higher γ-radiation energy of this isotope than of other conventional medical γ-radiation–emitting isotopes. Therefore, 18F-FDG imaging necessitates stronger radiation protection requirements. The aims of this study were to assess technologist whole-body and extremity exposure in our PET department and to evaluate the efficiency of our radiation protection devices (homemade syringe drawing device, semiautomated injector, and video tracking of patients).
Methods: Radiation dose assessment was performed for monodose as well as for multidose 18F-FDG packaging with both LiF thermoluminescence dosimeters (TLD) and electronic personal dosimeters (ED) during 5 successive 18F-FDG PET steps (from syringe filling to patient departure).
Results: The mean ± SD total effective doses received by technologists (n = 50) during all of the working steps were 3.24 ± 2.1 and 3.01 ± 1.4 μSv, respectively, as measured with ED and TLD (345 ± 84 MBq injected). These values were confirmed by daily TLD technologist whole-body dose measurements (2.98 ± 1.8 μSv; 294 ± 78 MBq injected; n = 48). Finger irradiation doses during preparation of single 18F-FDG syringes were 204.9 ± 24 and 198.4 ± 23 μSv with multidose vials (345 ± 93 MBq injected) and 127.3 ± 76 and 55.9 ± 47 μSv with monodose vials (302 ± 43 MBq injected) for the right hand and the left hand, respectively. The protection afforded by the semiautomated injector, estimated as the ratio of the doses received by TLD placed on the syringe shield and on the external face of the injector, was near 2,000.
Conclusion: These results showed that technologist radiation doses in our PET department were lower than those reported in the literature. This finding may be explained by the use of a homemade syringe drawing device, a semiautomated injector, and patient video tracking, allowing a shorter duration of contact between the technologist and the patient. Extrapolation of these results to an annual dose (4 patients per day per technologist) revealed that the annual extrapolated exposure values remained under the authorized limits for workers classified to work in a radioactivity-controlled area.
The setup of a PET scanner in a nuclear medicine department (PET/CT scanner) for 18F-FDG oncology imaging raised the issue of radiation dose exposure of technologists undertaking the preparation and administration of this radiopharmaceutical. Indeed, the higher γ-radiation energy of positron-emitting isotopes (511 keV) means that staff members could receive a higher whole-body dose than those working only with conventional nuclear medicine tracers. To date, however, few data have been published on technologist radiation doses received during work in dedicated PET departments (1,2). These studies measured whole-body doses received during 1 workday in a PET center using various positron-emitting isotopes (14.4 μSv) (2) or dose rates at various distances from patients injected with 370 MBq of 18F-FDG (the median exposure at 2 m from the patient at 1 h after injection was 2 μSv/h) (3). Some other studies aimed to evaluate hand doses received during 18F-FDG PET scanning and reported values of 710 μSv per technologist (4). All of these results are difficult to compare because radiation protection means are very dissimilar and because of differences in 18F-FDG packaging among suppliers (unit-dose [monodose] or multidose vials). Moreover, the dose measurements were recorded with electronic personal dosimeters (ED) worn at waist and wrist levels and did not provide information on the doses received by the fingers or with thermoluminescence dosimeters (TLD) worn around the second finger. Ring TLD have the disadvantage of a time lag measurement of the dose once per month because they cannot be changed at every step of 18F-FDG manipulation.
The aims of this study were, first, to inform technologists working with 18F-FDG about their whole-body and finger radiation doses and to compare our results with the maximum admissible doses prescribed by European Directive EURATOM 96/29 05/13/1996; second, to validate our radiation protection devices (especially our homemade syringe drawing device and a commercially available semiautomated injector); and third, to measure radiation doses corresponding to different kinds of 18F-FDG packaging.
MATERIALS AND METHODS
The Timone Hospital Nuclear Department PET/CT scanner is a dedicated Discovery ST scanner (GE Healthcare). Three technologists are assigned to cover a workday from 8:00 am to 6:00 pm. On an average day, the PET/CT scanner will image 10–13 patients. The study was conducted over a period of 6 mo, and measurements were recorded from the first PET examination of the day (n = 80), which corresponds to the highest multidose vial activity. All of the technologists were right handed.
18F-FDG Packaging
18F-FDG is supplied either in monodose vials (Cis-Bio Schering) or in multidose vials (4 doses; IBA) in lead containers with radioactivity per vial ranging from 450 MBq to 4 GBq.
18F-FDG Manipulation and Protection Devices
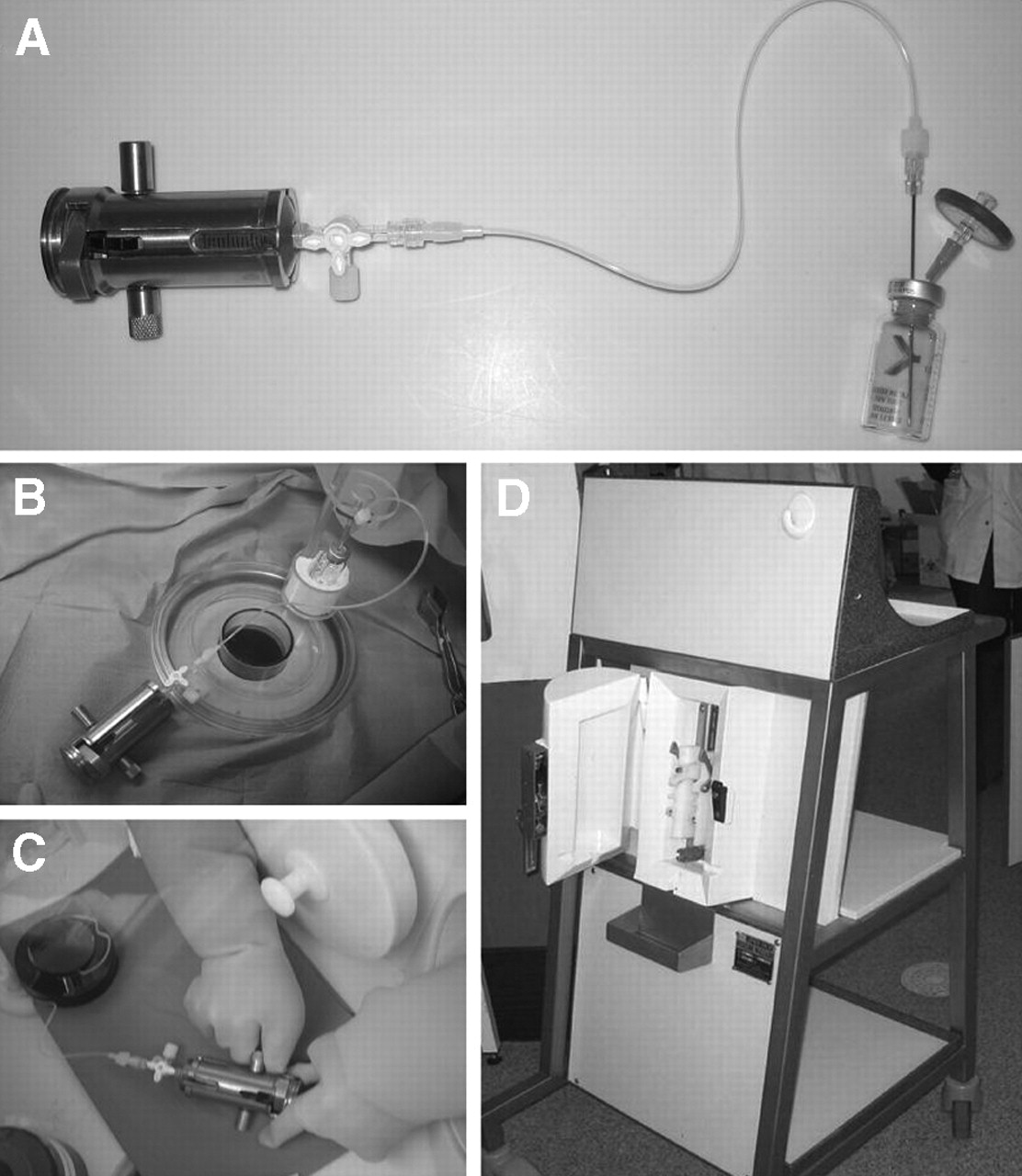
The 18F-FDG PET procedure was divided into 5 working steps. The first step is receipt of the 18F-FDG containers. The radiotracer is handled within a dedicated “hot” laboratory, being drawn up behind a large bench-mounted 60-mm-thick lead shield that has a 55-mm lead-equivalent glass insert (Lemer Pax). The dramatic high activity of 18F-FDG multidose vials led us to develop a homemade drawing device to allow syringe filling without direct contact with the vial, which remains in the hole of the dosimeter (Figs. 1A–1C). The second step is measurement of the total activity of the vial and the drawing up of the 18F-FDG dose (5 MBq/kg) in a syringe placed inside a 10-mm tungsten syringe shield (Lemer Pax). The third step is placement of the syringe in its shield into a semiautomated injector surrounded by a 30-mm-thick lead shield to avoid manual handling of the syringe. The fourth step is infusion of the 18F-FDG dose into the patient through a catheter that is withdrawn 40 min later. The last step includes the time spent in collecting the patient 1 h after the tracer infusion, escorting the patient to the PET room, positioning within the camera and, finally, after image acquisition, escorting the patient out of the department.

Schematic representation of our homemade drawing device. (A) Global view of device. (B) Positioning of 18F-FDG vial in hole of dosimeter. (C) Syringe filling. (D) Shielded semiautomated injector.
The technologists spend most of the scanning time in the control room, with a direct view of the patient through lead glass and a video link. The time spent in each step, the 18F-FDG activity injected, and the identified technical incidents are systematically monitored.
Dosimetry
18F-FDG Multidose Vials.
ED (Siemens EPD mk2.3) placed in the upper left pocket of technologist overalls allowed measurement of the whole-body individual dose at the end of each step of the 18F-FDG and patient manipulations. These dosimeters were calibrated twice each year by the Commissariat à l’Energie Atomique. The whole-body dose also was determined with 3 cylindric LiF TLD (diameter, 4.5 mm; thickness, 0.8 mm; GR200A; Société Fimel) placed in the upper left pocket of overalls worn by 3 agents during an entire PET center workday. The dose received by the irradiated TLD was determined with a PCL3 thermoluminescence reader (Société Fimel) according to manufacturer instructions. Measurements were recorded from 50 preparations. The values obtained were divided by the number of patients undergoing PET scans (mean of 12 patients per day) to confirm more accurately the whole-body dose received per patient. The dose reported for each pack of 3 TLD was the mean of the 3 measurements.
The dose received by the fingers during the first 3 steps of 18F-FDG manipulation was assessed with 2 of the TLD placed on the inside of the second finger of each hand. The TLD were selected and calibrated after exposure to 160 mGy of 60Co irradiation (1000 IEC 60Co generator; Theratron). Measurements were recorded from 50 preparations. The dose reported for each pair of TLD was the mean of the 2 measurements.
18F-FDG Monodose Vials.
Because the difference in exposure related to the manipulation of monodose or multidose vials of 18F-FDG is related only to steps 1 and 2, we compared the values obtained for whole-body irradiation and finger irradiation during these first 2 steps with monodose or multidose vials of 18F-FDG. Measurements were recorded from 30 preparations.
To estimate the protection afforded by the semiautomated injector, 3 TLD were placed directly on the syringe shield, and 3 other TLD were placed on the external face of the injector. Ten pairs of TLD were used for this determination.
Statistical Analysis
All values are reported as mean ± SD. The Mann–Whitney test was performed to statistically compare values obtained with TLD for whole-body and finger exposures during the first 2 steps with each 18F-FDG package and whole-body doses obtained with TLD and ED. A P value of <0.05 was considered significant.
RESULTS
The effective doses measured during steps 1 and 2 with TLD and ED were negligible (step 1, ED: 0.29 ± 0.4 μSv; step 2, ED: 0.10 ± 0.1 μSv); therefore, Table 1 shows only the mean ± SD for whole-body doses during steps 3, 4, and 5 of manipulation of multidose vials of 18F-FDG, as recorded by ED and TLD worn in the upper left pocket of the overalls (n = 50). The mean ± SD total effective doses received by technologists during all of the steps of 1 18F-FDG dose preparation were 3.24 ± 2.1 and 3.01 ± 1.4 μSv for ED and TLD, respectively (345 ± 84 MBq injected). These 2 groups of values (ED and TLD) did not differ significantly.
Mean ± SD (n = 50) Whole-Body Doses During Steps 3, 4, and 5, as Estimated by ED and TLD Worn in Upper Left Pocket of Overalls
Table 2 shows the mean ± SD for finger irradiation during the first 3 steps of manipulation of 18F-FDG multidose vials (n = 50). The mean ± SD total doses received at the finger level were 231.9 ± 36 and 206.3 ± 32 μSv for the right hand and the left hand, respectively. The mean ± SD total doses received at the finger level during the first 2 steps of 1 18F-FDG dose preparation were 204.9 ± 24 and 198.4 ± 23 μSv, respectively, for the right hand and the left hand, respectively (mean ± SD vial activity: 3,240 ± 1,102 MBq; mean ± SD syringe activity: 345 ± 93 MBq).
Mean ± SD (n = 50) Finger Irradiation During First 3 Steps of Manipulation of 18F-FDG Multidose Vials
Table 3 shows the mean ± SD finger doses during the first 2 steps of manipulation of monodose vials of 18F-FDG (n = 30). The mean ± SD total doses received at the finger level for 1 18F-FDG dose preparation were 127.3 ± 76 and 55.9 ± 47 μSv for the right hand and the left hand, respectively (mean ± SD vial activity: 405 ± 22 MBq; mean ± SD syringe activity: 302 ± 43 MBq).
Mean ± SD (n = 30) Finger Doses During First 2 Steps of Manipulation of 18F-FDG Monodose Vials
The mean ± SD irradiation rates for TLD positioned either directly on the syringe shield or on the external face of the injector are shown in Table 4 (n = 10). The mean ± SD ratio of the dose received by the syringe TLD and the dose received by the injector TLD was 1,852 ± 860, a value that corresponds to nearly complete protection.
Mean ± SD (n = 10) Dose Rates Measured by TLD Positioned Either on Syringe Shield Inside Injector or on External Face of Injector
The mean ± SD dose received by TLD worn in the upper left pocket of the overalls by 3 agents during an entire PET center workday, determined in relation to the number of patients undergoing PET scans (n = 48), was 2.98 ± 1.8 μSv. The mean ± SD activity injected into the patients was 294 ± 78 MBq.
Technical problems occurring throughout the 18F-FDG manipulations dramatically increased the doses received by the technologists and are shown in Table 5.
Whole-Body and Finger Doses Related to Technical Problems Occurring Throughout 18F-FDG Manipulation
DISCUSSION
Numerous studies (5–11) have reported the effective doses received by nuclear medicine technologists, but few have considered specifically positron-emitting tracers. The results presented in our study show that, for 12 mo in succession, the radiation exposure at the whole-body and finger levels of technologists during 18F-FDG manipulation in our PET center is dramatically lower than the maximum values allowed in European Directive EURATOM 96/29 05/13/1996 (whole-body effective dose: <20 mSv/y; equivalent finger dose: 500 mSv/y).
During step 1, the doses received by the left hand were obviously significantly higher when multidose vials were used than when monodose vials were used (135.2 ± 192 μSv vs. 14.9 ± 20 μSv) because of close contact with the 18F-FDG vial, whose activity is near 3.5 GBq at the time of supplying.
During step 2, right-hand exposure was significantly higher than left-hand exposure, as the right hand was close to the tubing of the drawing device filled with 18F-FDG (Fig. 1C). This discrepancy was more evident when multidose vials were used than when monodose vials were used (211.3 ± 180 μSv vs. 43.4 ± 39 μSv) because of the higher volumic activity (multidose: 555 MBq/mL; monodose: 250 MBq/mL). Shielding of the tubing has been considered, but it would impede visual control of syringe filling.
However, the higher doses received with multidose vials than with monodose vials must be balanced for 2 reasons: first, the mean time spent during step 1 (177 ± 111 and 112.7 ± 41 s for multidose and monodose vials, respectively) must be repeated for each patient with monodose vials, whereas with multidose vials, the procedures are performed every 4 patients; second, the total activity of the multidose vials decreases according to the 18F-FDG half-life.
It is difficult to strictly compare PET centers because of variability in protocols, acquisition times, injected activity, and radiation protection devices used, but we can nevertheless compare the effective dose measured during the entire PET procedure in our study with those reported in the literature. Published data on the radiation exposure of technologists during 18F-FDG PET scanning are very sparse. Chiesa et al. (1) and Benatar et al. (2) reported similar technologist effective doses per whole-body 18F-FDG PET scanning of 5.9 μSv (500 MBq per patient) and 5.5 μSv (14.4 μSv/d; 320 MBq per patient; 2–3 patients per day), respectively. However, Linemann et al. (4) in Germany reported a mean total personal dose of at least 10 μSv per technologist.
The technologist exposure doses reported above are higher than our ED or TLD measured doses. In the study of Chiesa et al. (1), the higher injected activity could partly explain this difference (500 MBq vs. 345 MBq). Moreover, less close contact with the radioactive source in the present study than in the study of Benatar et al. (2) (9.2 min per technologist per patient vs. 13.9 min per technologist per patient), the use of a semiautomated injector, and the video and audio tracking of the injected patients could be involved in the lower radiation exposure in the present study.
Because the measured values were subdivided into separate contributions from each phase of the manipulation of 18F-FDG, it is possible to compare step by step the whole-body and finger doses measured with the very sparse published data.
Concerning the effective dose, as a consequence of the maximum shielding of the hot cell, the first 2 steps of 18F-FDG manipulation led to negligible values comparable to ours (<1 μSv) (4). In contrast, steps 3, 4, and 5 induced greater radiation exposure, which is highly dependent on the radiation protection means used, especially a shielded automated injector or a lead screen for injection and a video link to avoid close contact with the injected patients. None of the published data evaluated radiation exposure during the transfer of the syringe from the hot cell to the patient. According to the work of Linemann et al. (4), the effective dose measured during the injection step led to about 3 μSv per injection, a value that is higher than the values measured by our ED (1.08 ± 1.6 μSv) or TLD (0.81 ± 1.0 μSv) during this step. It is worth noting that these authors did not describe the protection devices used for injection; the discrepancies in effective doses measured are probably attributable to the use in our study of the shielded semiautomated injector, which afforded nearly complete protection. In our PET center, where patients are located in rooms without direct communication with the hot laboratory, this automated injector is very useful for transferring the dose from the hot laboratory to the injection rooms.
The only published study focusing on the dose received by the hands, estimated by TLD, was that of Linemann et al. (4), who reported a mean finger exposure of 710 μSv during syringe preparation from 18F-FDG multidose vials. Under these conditions, if we sum the right and left hand doses from our first 3 steps, whatever the 18F-FDG packaging used, the mean values obtained are at least 3 times lower (mean ± SD finger dose from steps 1, 2, and 3 for multidose vials: right hand = 231.9 ± 36 μSv and left hand = 206.3 ± 32 μSv; mean ± SD finger dose from steps 1, 2, and 3 for monodose vials: right hand = 157.3 ± 67 μSv and left hand = 78.2 ± 43 μSv). These differences probably can be explained by the use of our homemade drawing device, which avoids close contact between the technologist’s hands and the 18F-FDG vial and which appears to be more effective than the grip used by Linemann et al. (4). Moreover, the use of the shielded semiautomated injector, which avoids syringe handling during the injection, also may contribute to the reduction in hand exposure.
In parallel, we identified some technical problems (Table 5). The first problem occurred during syringe filling (step 2) and was attributable to syringe disconnection from its shield protection, which led to a longer dose preparation time and to higher finger doses. Several other problems led to an increase in the duration of the dose transfer from the hot cell to the semiautomated injector. These problems included expelling air from the syringe, handling the syringe near the technologist’s chest, or difficulties with the syringe interlocking with the semiautomated injector. Moreover, the semiautomated injector got jammed once and therefore caused a longer duration of the injection and an increase in the TLD whole-body dose. One case of a noncompliant patient also occurred, making it necessary to spend more time on positioning and therefore causing an increase in the TLD whole-body dose.
CONCLUSION
It can be concluded from this study that, in our PET center, whatever the 18F-FDG packaging supplied, the use of our homemade drawing device in association with a shielded semiautomated injector and video tracking of patients led to lower technologist radiation exposure at the whole-body and finger levels than the published values. The use of 18F-FDG multidose vials obviously led to higher finger exposure during receipt of the 18F-FDG containers and syringe filling, but this exposure was associated with packaging containing 4 18F-FDG doses and so required only 1 receipt step and drawing device installation every 4 patients. Moreover, for 12 mo in succession and for technologists scanning 4 patients per day, the doses measured with either monodose or multidose vials were always lower than the maximum acceptable values reported in European Directive EURATOM 96/29 05/13/1996, even with the technical problems encountered during 18F-FDG manipulation.
Footnotes
For correspondence or reprints contact: Pascale Pisano, PhD, Unité de Radiopharmacie, Service Central de Médecine Nucléaire, CHU Timone, 254 Rue Saint-Pierre, 13005 Marseille, France.
E-mail: ppisano{at}mail.ap-hm.fr





{kind=link}
Jump to section
Related Articles
Cited By...
- The Effects on Technologist Occupational Exposure in PET/CT Departments When Working with Students at Various Levels of Supervision
- Technologist Approach to Global Dose Optimization
- Comparison of 3 Devices for Automated Infusion of Positron-Emitting Radiotracers
- Occupational Radiation Dosimetry Assessment Using an Automated Infusion Device for Positron-Emitting Radiotracers
- Radiation protection in fixed PET/CT facilities--design and operation
- Assessment of Patient Exposure to X-Radiation from SPECT/CT Scanners