


Abstract
18F-FDG PET is emerging as a useful tool in the staging and restaging of many malignant neoplasms, such as lymphoma, lung cancer, colorectal cancer, head and neck cancer, breast cancer, and melanoma. To accurately interpret 18F-FDG findings one must be familiar with the normal physiologic distribution of the tracer, frequently encountered physiologic variants, and benign pathologic causes of 18F-FDG uptake that can be confused with a malignant neoplasm. The objectives of this article are to (a) describe the mechanism of 18F-FDG uptake, (b) list the patient preparation and pertinent patient history before 18F-FDG imaging, (c) describe the whole-body physiologic distribution of 18F-FDG, (d) list and discuss normal physiologic variants, and (e) list and discuss benign pathologic causes of 18F-FDG uptake.
PET with 18F-FDG is one of the fastest growing techniques in nuclear medicine today. 18F-FDG is an analog of glucose and, as such, a versatile radiopharmaceutical with major applications in oncology, neurology, and cardiology. Clinically, 18F-FDG PET is most widely used for cancer detection. 18F-FDG PET has proven its efficacy in general oncologic imaging. The clinical impact of 18F-FDG PET has been reported for many different tumor types, such as lung tumors, colorectal carcinomas, breast carcinoma, and lymphomas. In an extensive review of the 18F-FDG PET literature from 1993 to 2000 comprising 419 articles, the overall sensitivity and specificity was estimated to be 84% and 86%, respectively, and the results from 18F-FDG PET changed the management in approximately one third of the patients (1).
PET with 18F-FDG is approved by the Center for Medicare and Medicaid Services for diagnosing, staging, and restaging lung cancer, colorectal cancer, lymphoma, melanoma, head and neck cancer, and esophageal cancer.
Tumor imaging with 18F-FDG is based on the fact that malignant tumors with high metabolic rates take up greater amounts of glucose and 18F-FDG than surrounding tissues.
PET has several advantages over other imaging modalities in cancer detection. Many forms of cancer are systemic and whole- body imaging with 18F-FDG provides a way to monitor extent and progression of the disease. Also, because biochemical changes in a tumor occur before morphologic changes, PET has the potential to provide diagnostic information earlier than CT or MRI.
18F-FDG is administered intravenously and is then transported into cells by glucose transporter proteins in a fashion similar to that for unlabeled d-glucose. Numerous malignant tumors express higher numbers of specific membrane transport proteins, with greater affinity for glucose than normal cells, which permits increased glucose flow into the cancerous cells (2).
Subsequently, 18F-FDG is then phosphorylated by hexokinase to form 18F-FDG-6-phosphate. The cell membrane is impermeable to both glucose 6-phosphate and FDG-6-phosphate. However, the latter cannot be further degraded via the glycolysis pathway nor can it easily undergo dephosphorylation by glucose-6-phosphatase. Ultimately, 18F-FDG-6-phosphate remains trapped within the cell and the more 18F-FDG within the cells the more increased uptake within the tumor itself (3). To a certain extent, the increased localization usually correlates with more aggressive tumors and greater numbers of viable tumor cells (4,5).
Tumor cells are, however, not the only cells that exhibit an increased uptake of 18F-FDG. Recently, Maschauer et al. (6) have shown a contribution of the endothelial cells within the tumors and vascular lesions to 18F-FDG uptake, which can be enhanced by endothelial cytokine (vascular endothelial growth factor or VEGF). VEGF stimulates the proliferation and migration of vascularly derived endothelial cells and is overexpressed in a variety of tumors, including renal, breast, ovary, and colon cancer (6).
Multiple reports have shown that lesions with a high concentration of inflammatory cells, such as neutrophils and activated macrophages, also show increased 18F-FDG uptake, which can be mistaken for malignancy in patients with proven or suspected cancer (4). Animal studies have shown that inflammatory cells contribute significantly to 18F-FDG uptake in tumors (7–13). Using a tumor mouse model, Kubota et al. reported that 29% of 18F-FDG uptake was related to nontumoral tissue (11). This observation could explain why normal and noncancerous conditions, such as infection, inflammation, and healing tissues, can also show increased 18F-FDG uptake.
Not all malignant tissues have avidity for 18F-FDG. Some types of cancer tissues with low malignant potential, such as carcinoid tumor, bronchoalveolar cancer, and mucinous adenocarcinoma, use 18F-FDG at the same rate as normal surrounding tissues, leading to failure in identifying these sites of cancers (7–16).
To avoid as many confounding and potentially misleading issues as possible when interpreting the scan, certain prerequisites need to be fulfilled before performing any PET study. They are listed in Table 1. The relevant clinical data from the referring physicians and the patient must be collected and all other diagnostic radiologic investigations done before PET should be reviewed. Relevant history and data that must be collected before 18F-FDG PET are listed in Table 2. The oncologic consult should include the reason(s) for requesting the PET study and, in certain circumstances, a limited physical examination is requested to clarify some findings.
Patient Preparation
Relevant Patient History and Data
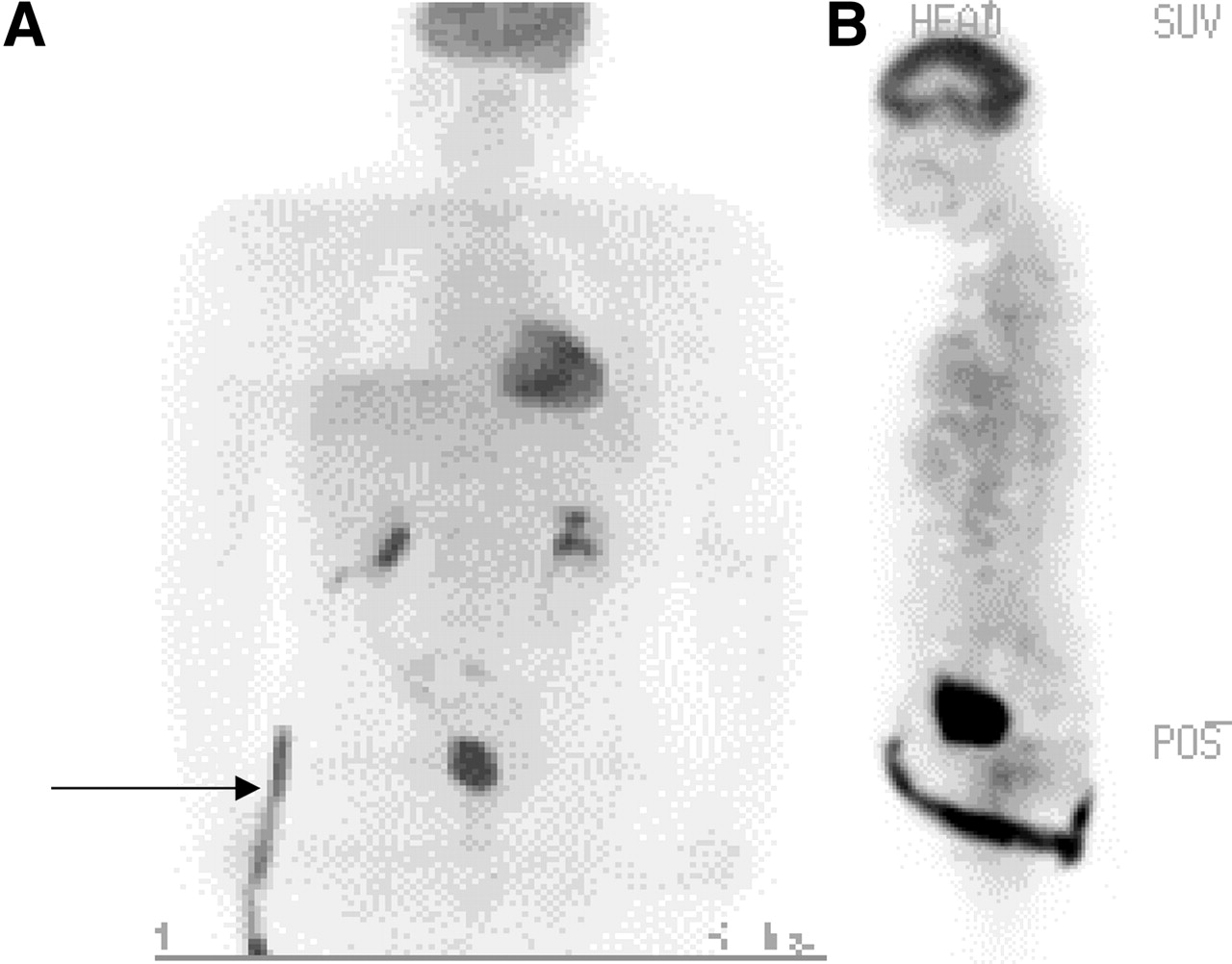
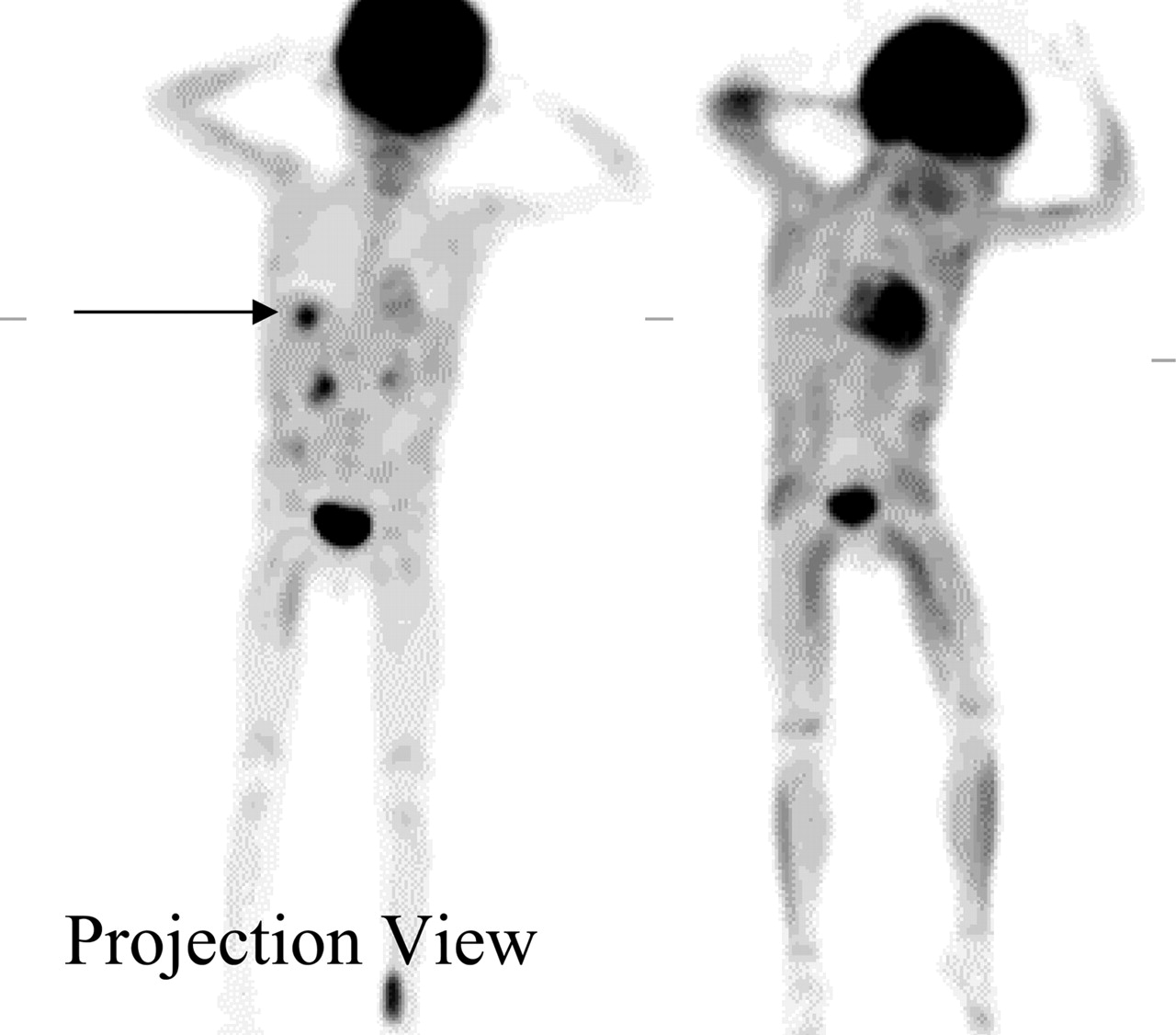
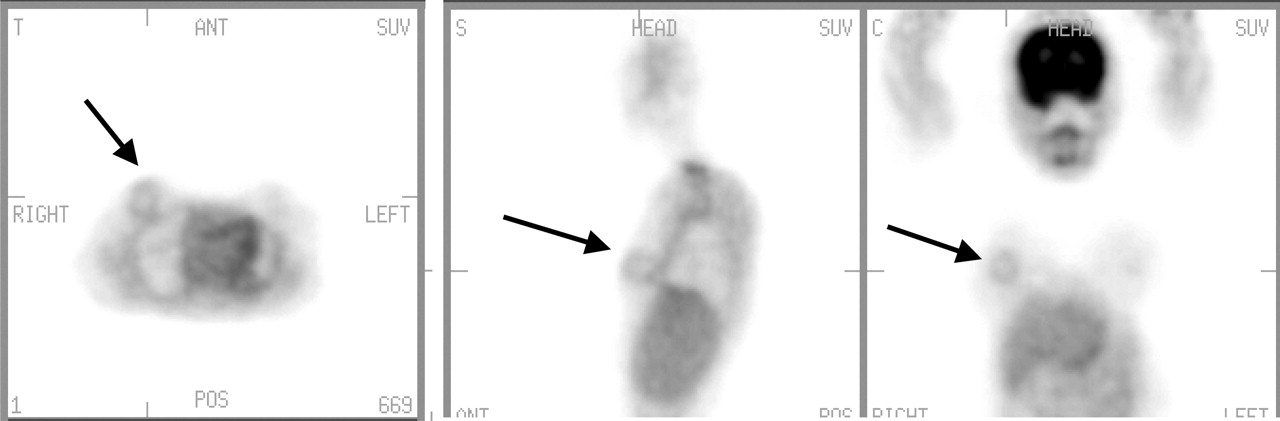
Proper quality control, imaging, and reconstruction are essential for optimal resolution and scan interpretation. The technologist performing the scan should note and record any excessive patient motion. Consider using a head holder to reduce possible motion in head and neck cancer imaging (Fig. 1). Also, consider increasing the acquisition time for both emission and transmission scans in overweight patients to improve the image quality.
Asymmetric salivary gland uptake (projection view). Note increased 18F-FDG uptake in right face/salivary gland and region (arrow) as compared with contralateral side. Patient’s head moved during acquisition. SUV = standardized uptake value.
HEAD AND NECK
Brain cortex generally has an intense uptake because glucose is the only source of energy in the brain. 18F-FDG accumulation in the brain is fairly constant and consistent as the brain is known to account for as much as 20% of total-body glucose metabolism in the fasting state. Low-to-moderate 18F-FDG uptake occurs in the tonsils and at the base of the tongue because of physiologic activity associated with the lymphatic tissue in Waldeyer’s ring.
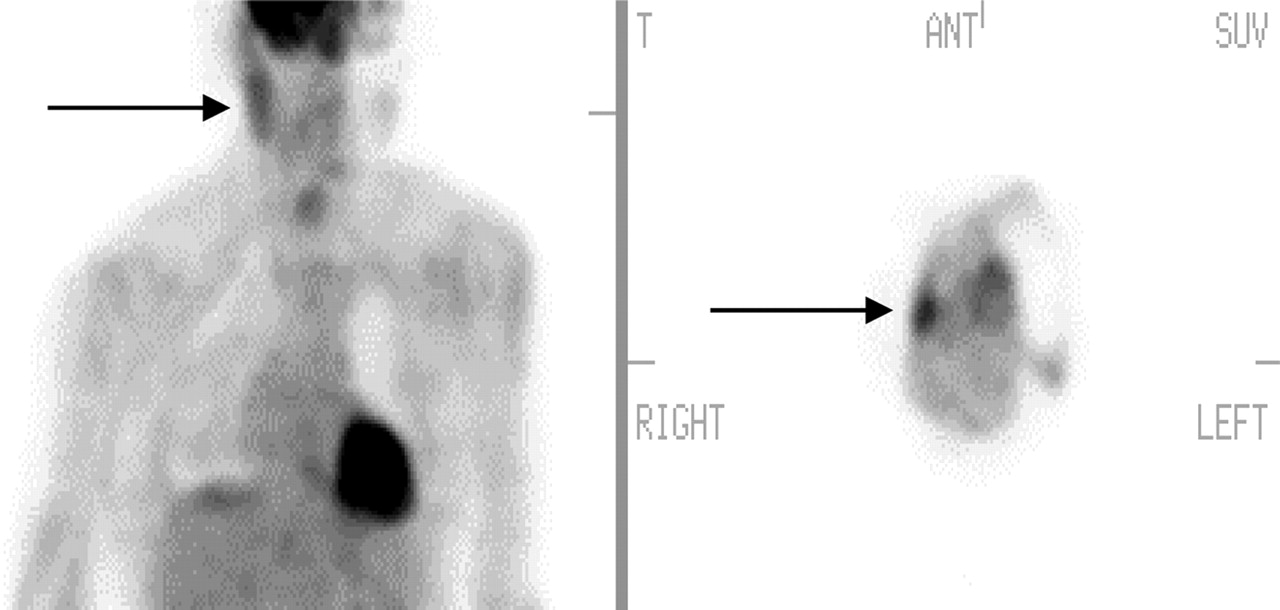
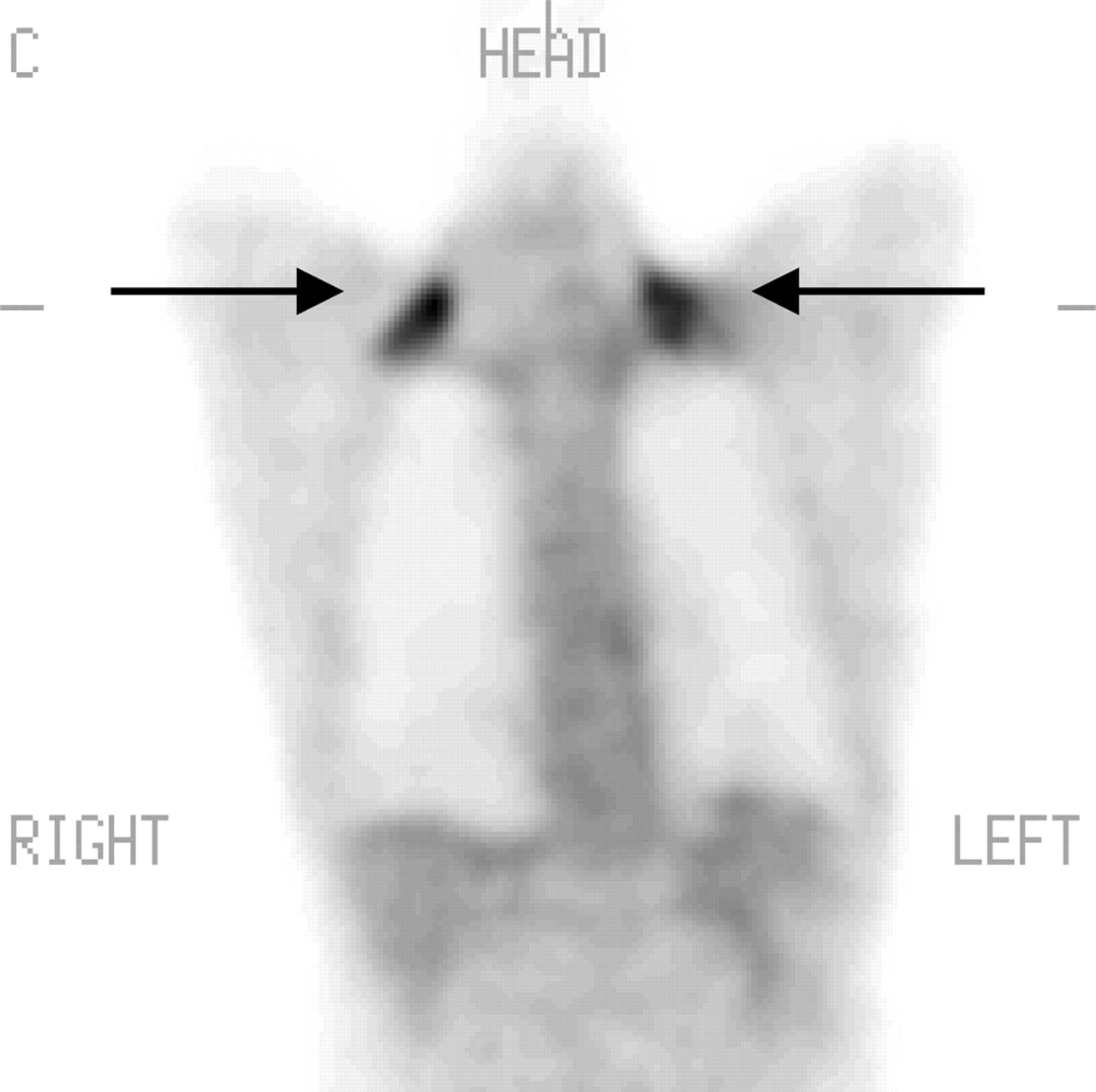
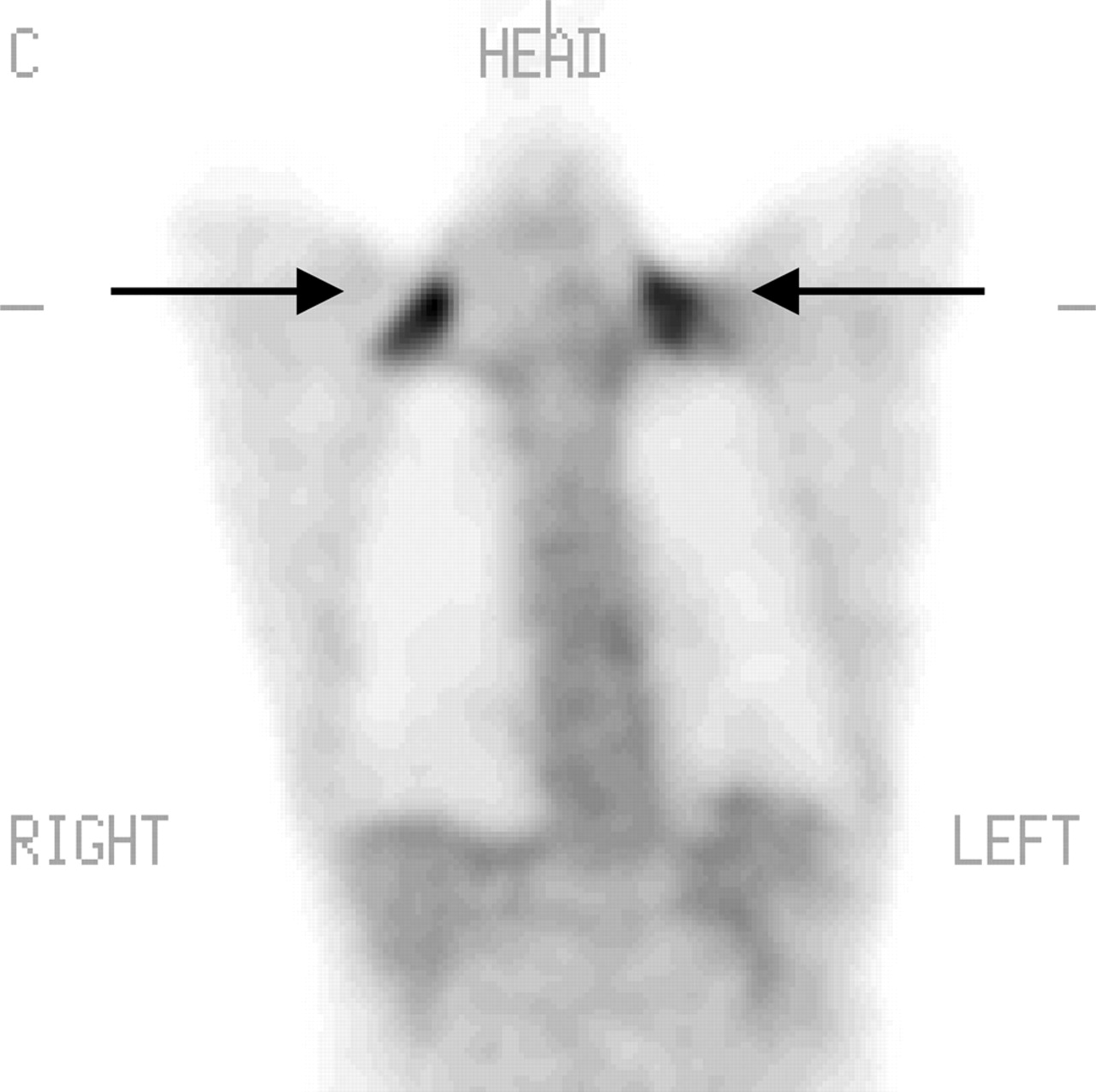
The presence of 18F-FDG uptake is highly variable (mild or intense) in the salivary glands, including the parotid, submandibular, and sublingual glands (17) (Fig. 2). Salivary gland uptake may be symmetric or asymmetric. Asymmetry in the salivary glands could be positional or could be due to surgical or postradiation therapy inflammatory-induced changes. Radiotherapy can decrease the uptake on the irradiated side.
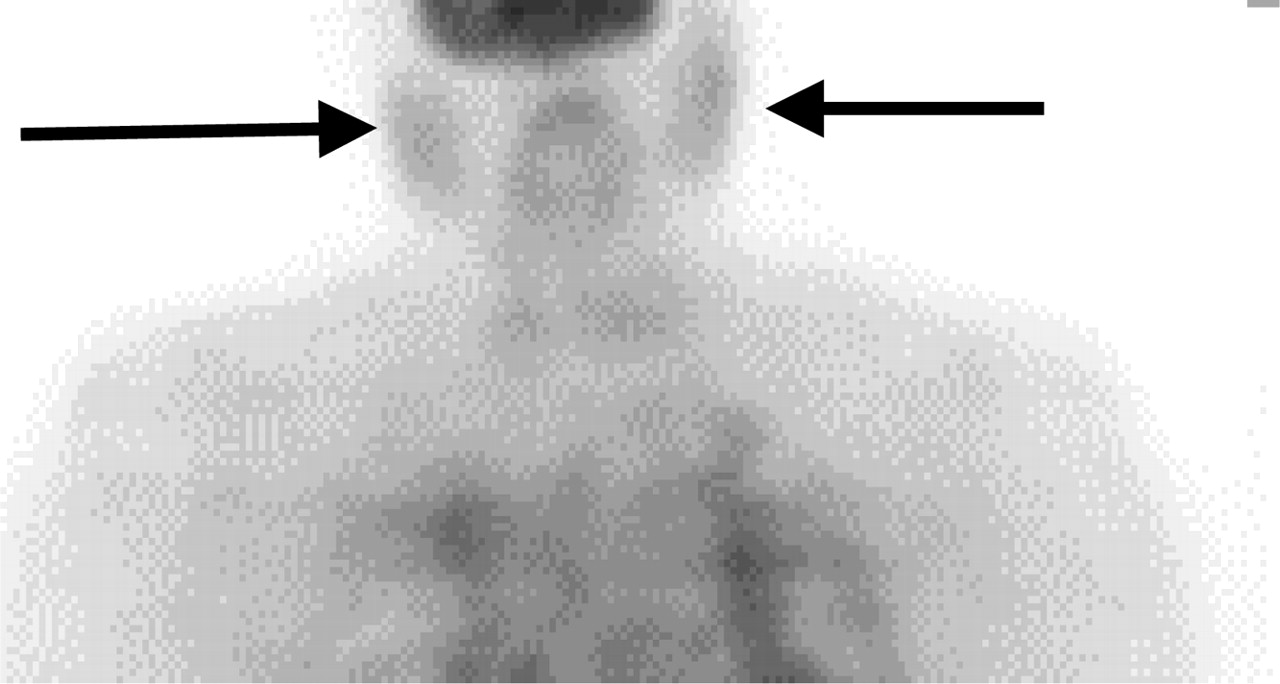
Symmetric salivary gland uptake (projection view; arrows) shows mild uptake.
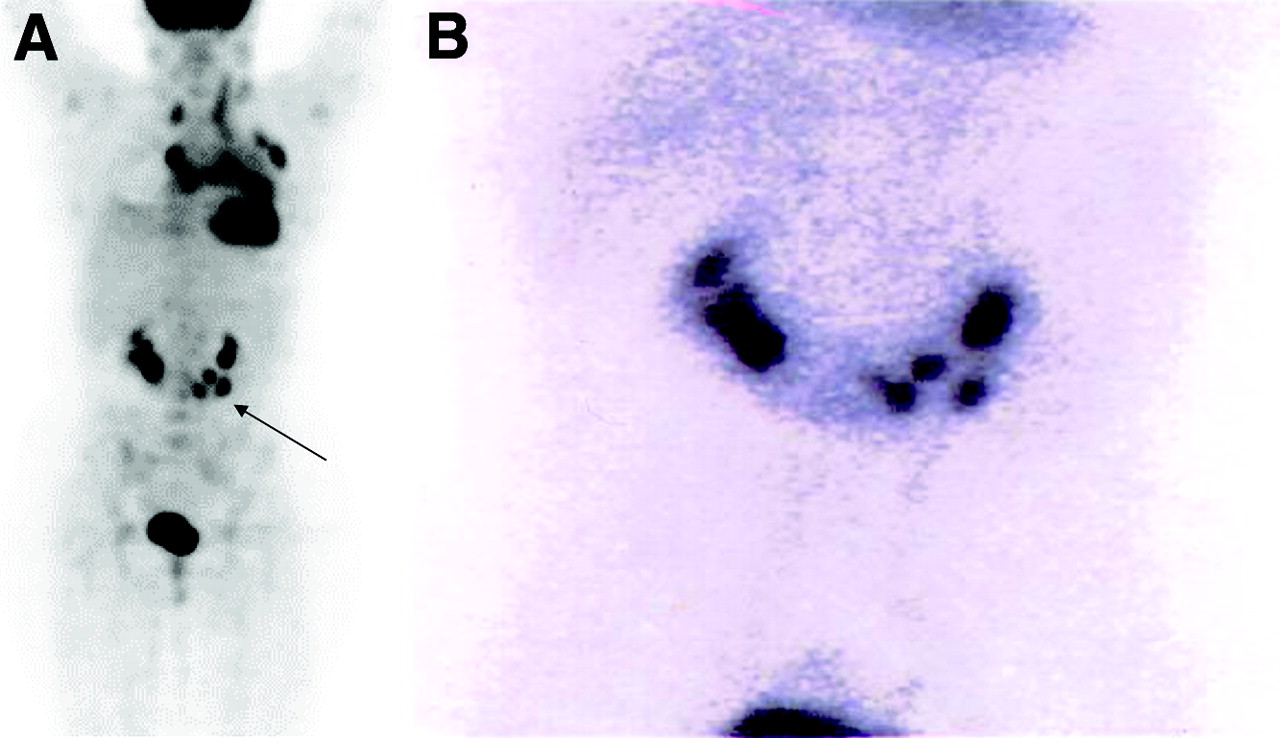
The extraocular muscles, muscles of the oral cavity, and laryngeal muscles accumulate 18F-FDG with varying degrees. A moderate amount of uptake can be seen in the anterior part of the floor of the mouth due to the genioglossus muscle, which prevents the tongue from falling back in supine patients. If a patient grinds the teeth or chews, the muscles of mastication may appear very prominent. Excessive talking after injection can cause prominent 18F-FDG uptake within the larynx. The laryngeal uptake is normally very subtle, appearing in the form of an inverted V shape. Focal unilateral uptake within the larynx could be due to muscle overuse as in the case of contralateral vocal cord paralysis (18) (Fig. 3).
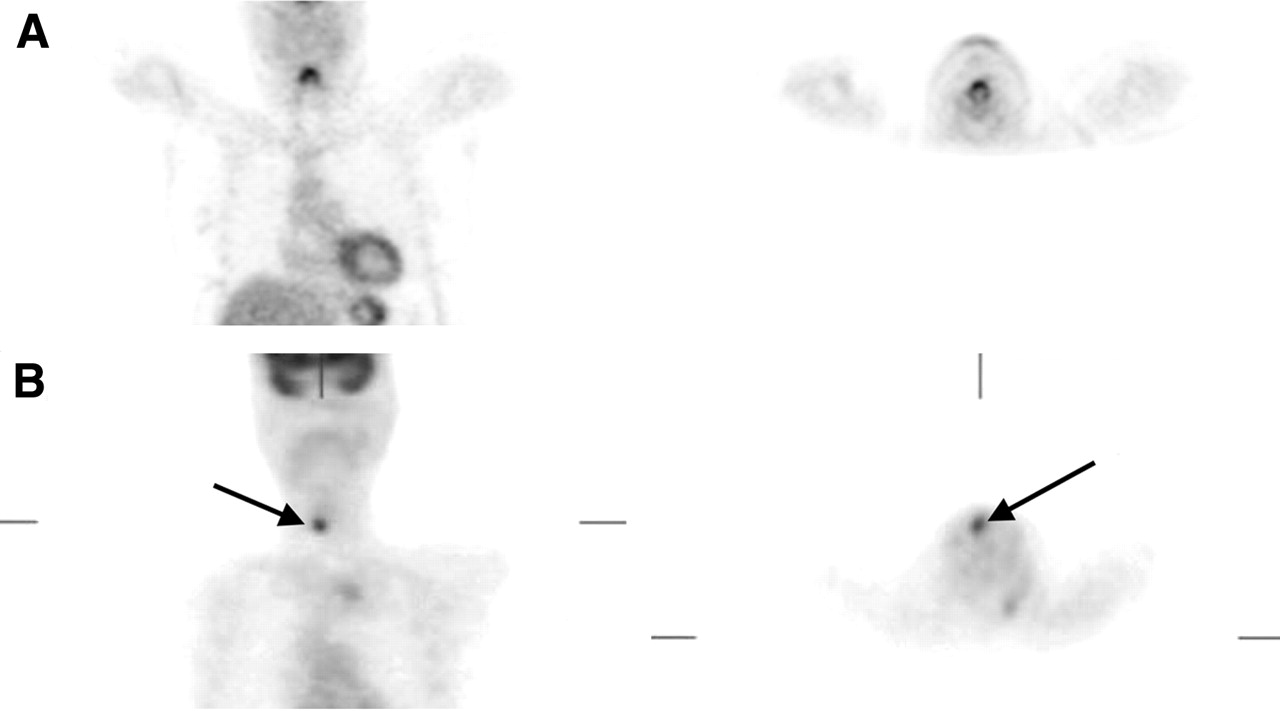
Laryngeal uptake. (A) Normal symmetric uptake in larynx. (B) Focal unilateral (arrows). Coronal view on left; transaxial view on right.
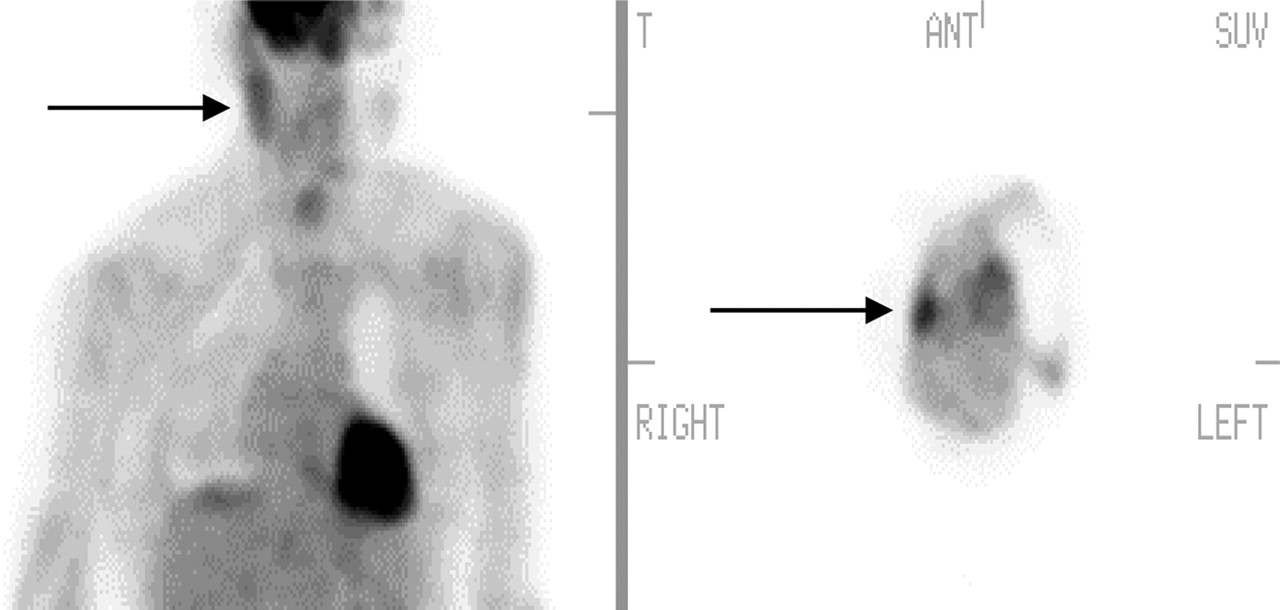
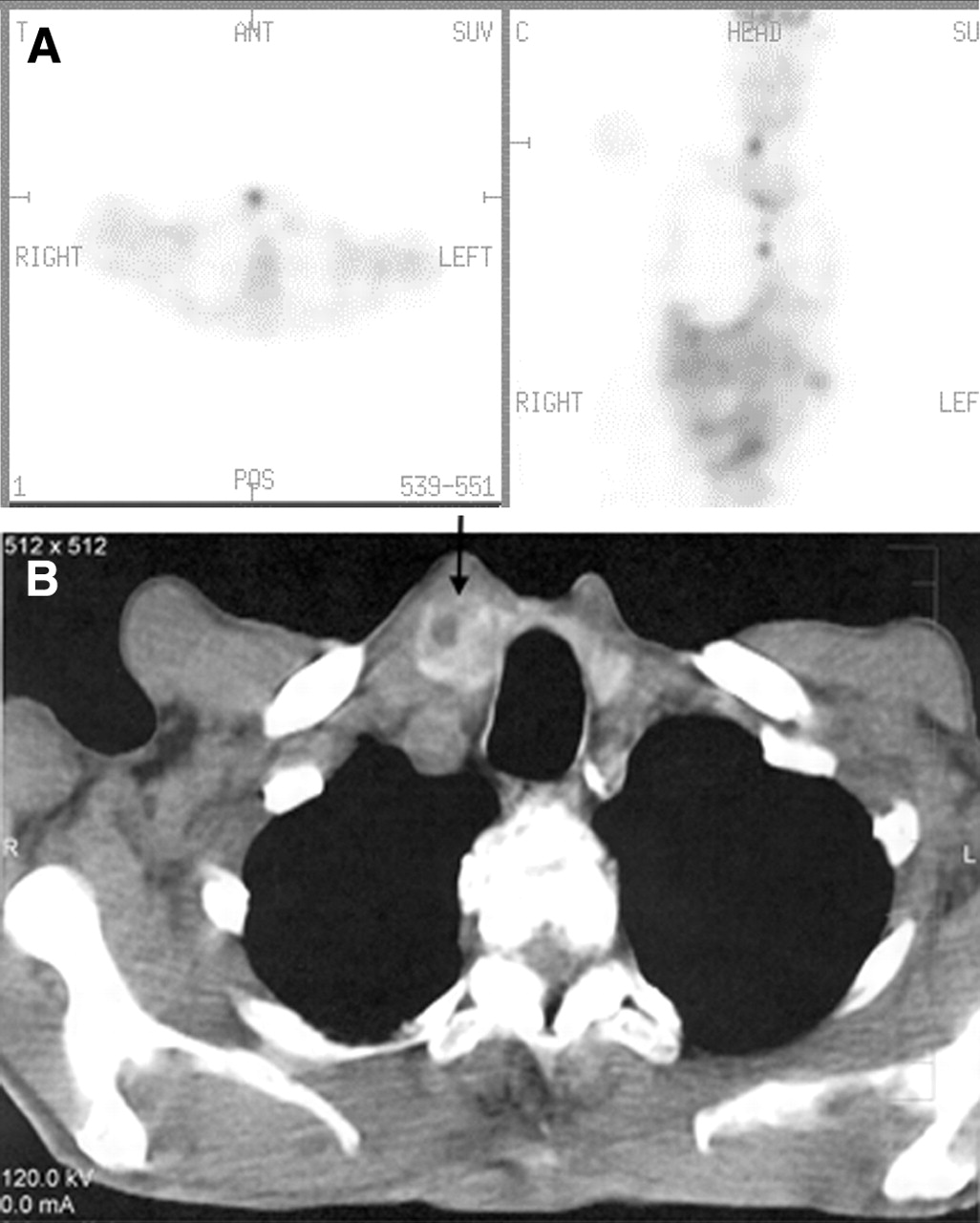
Usually the thyroid uptake is negligible; ranging from no accumulation to mild uptake. Incidental increased 18F-FDG uptake in the thyroid can be seen in about 2% of scans (19). Such uptake could be diffuse as in thyroiditis or Graves’ disease (Fig. 4). Focal uptake can occur with autonomously functioning thyroid nodules and thyroid malignancies. Patients with focal uptake in the region of the thyroid should be further evaluated because of a higher risk of the finding being associated with malignancy (20) (Fig. 5).
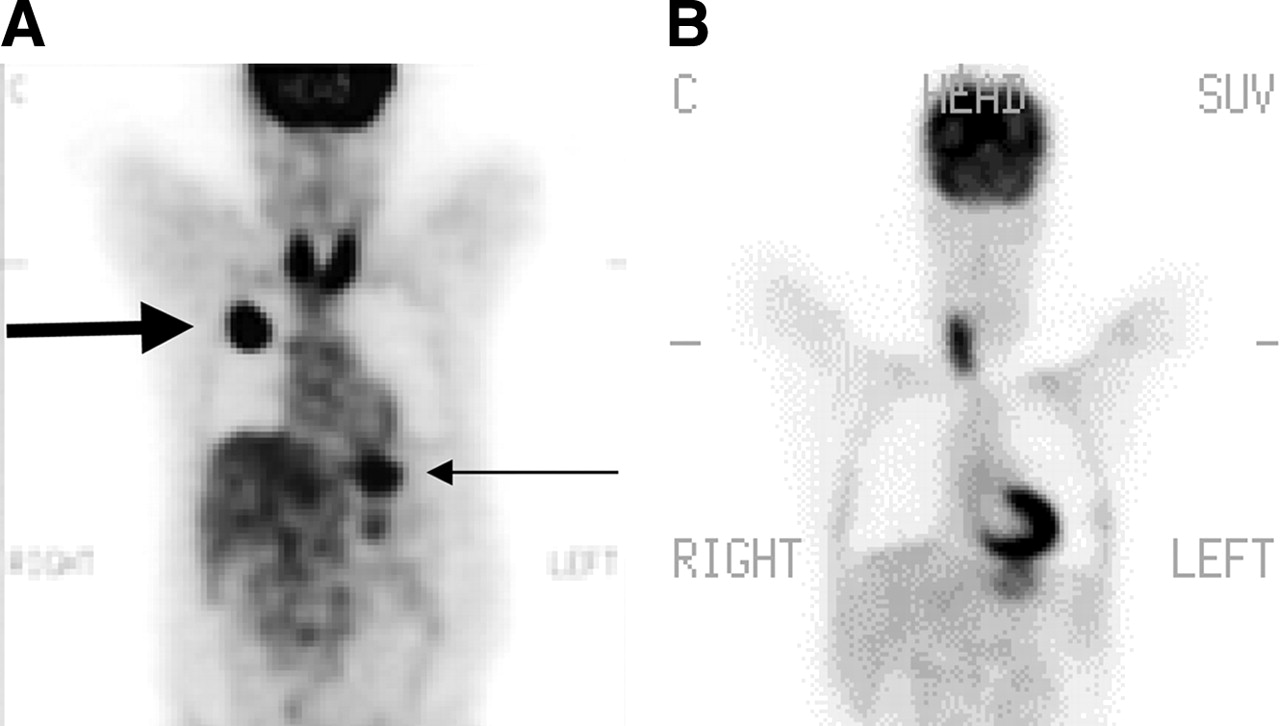
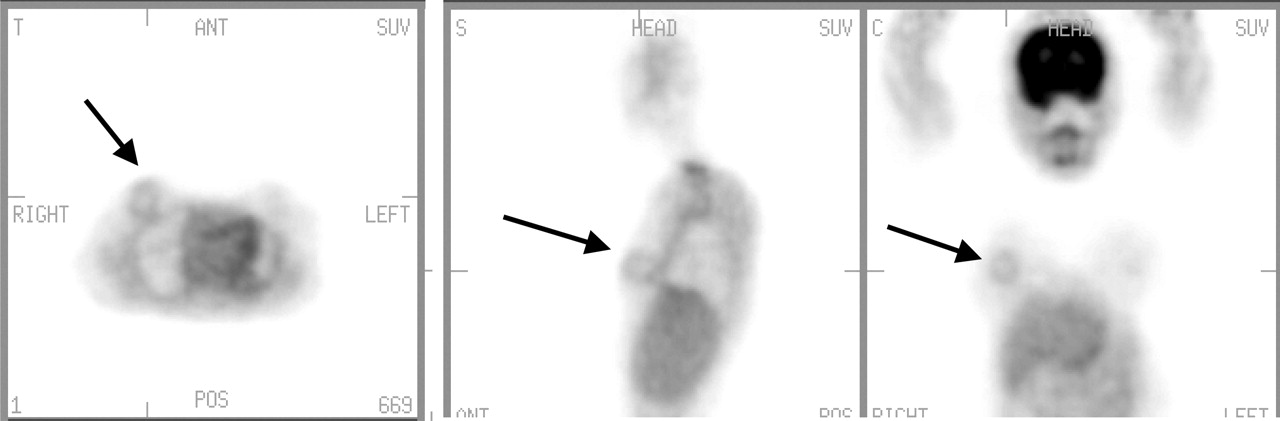
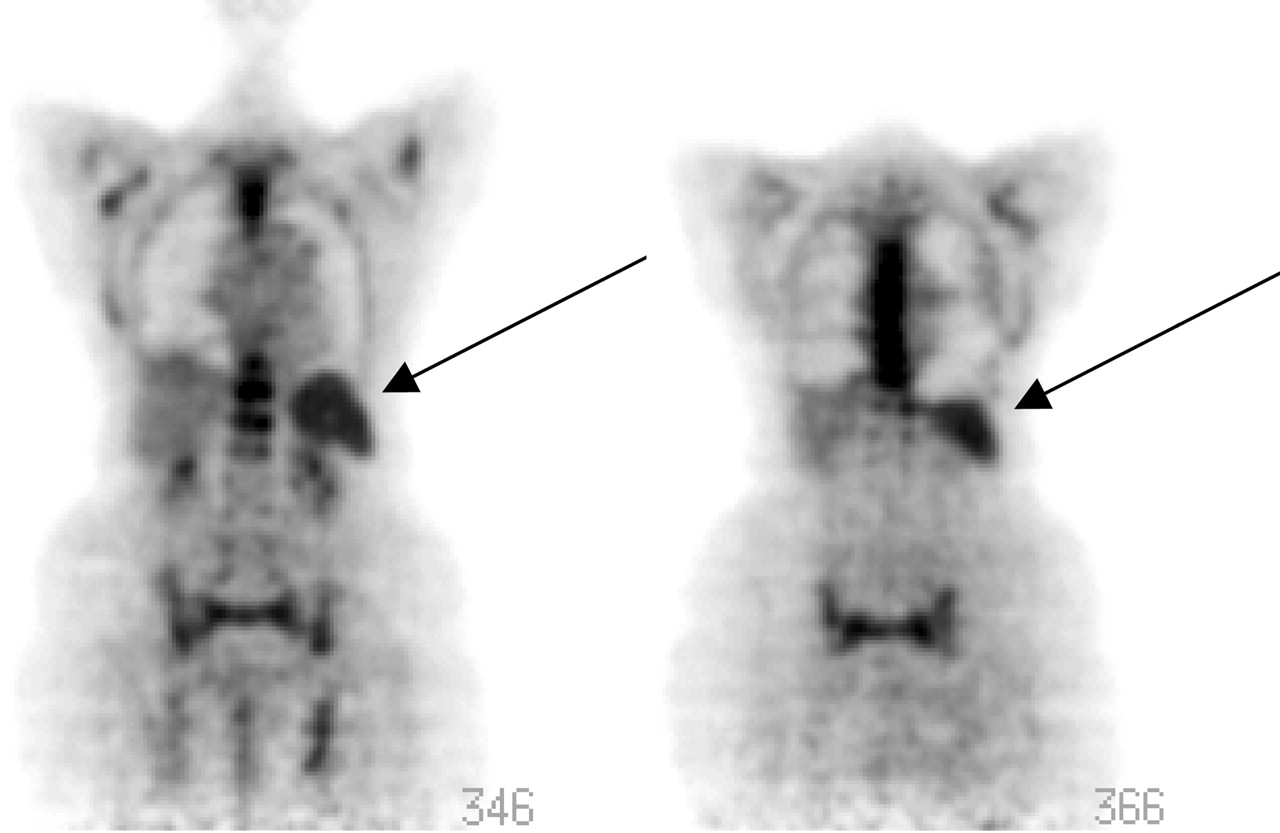
Thyroid inflammation. (A) Patient with known squamous cell carcinoma of upper lobe of right lung (thick arrow) who was being evaluated for initial staging. Note intense thyroid uptake due to Hashimoto’s thyroiditis. Also note normal stomach uptake (thin arrow). (B) A 57-y-old woman with history of breast carcinoma and left thyroidectomy who was being evaluated because of rising levels of tumor markers. Neck uptake was due to Hashimoto’s thyroiditis, which could easily have been mistaken for nodal uptake. C = coronal.
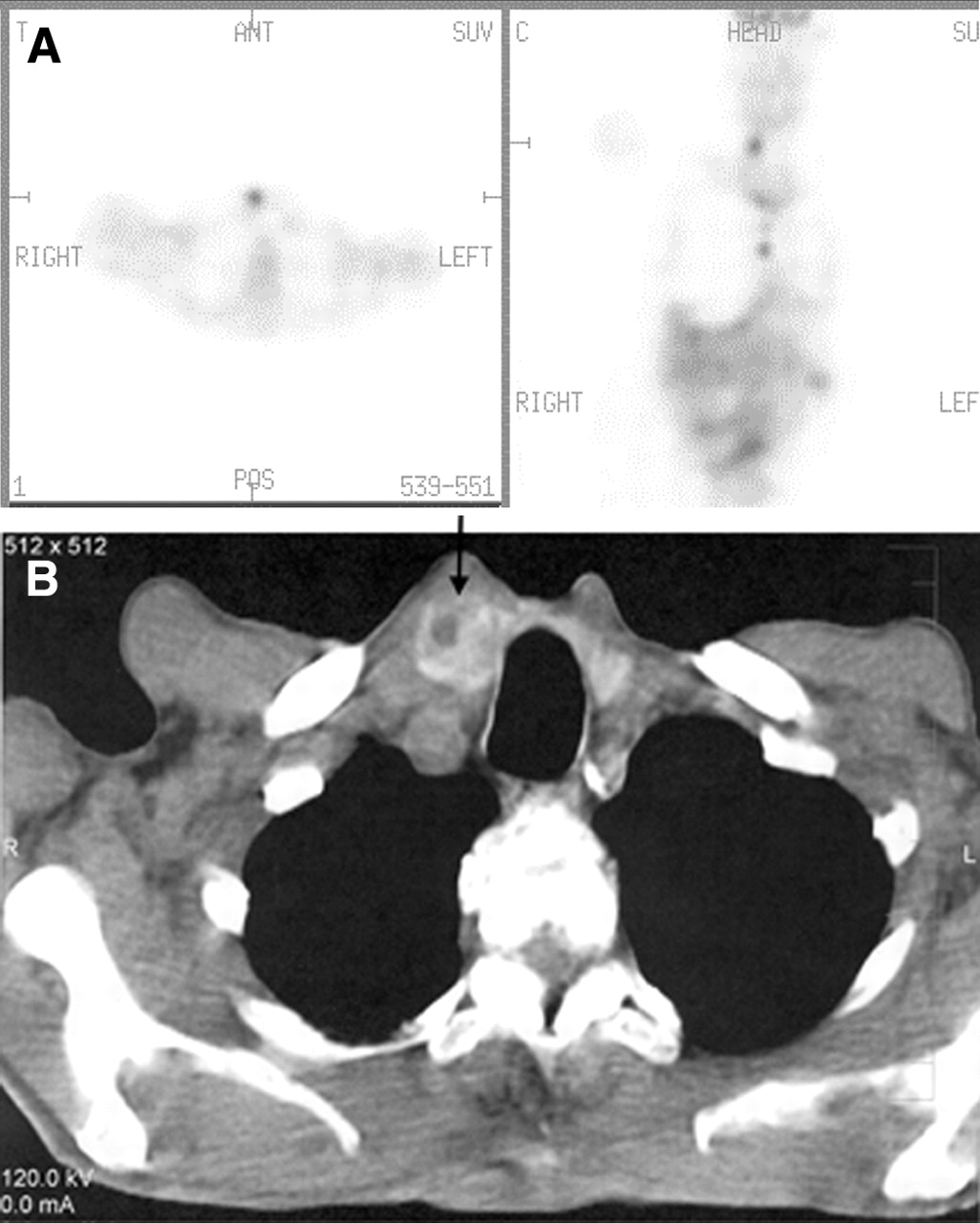
Focal thyroid uptake. (A) Focal thyroid uptake seen in right lobe of thyroid gland corresponding to focal density (arrow) seen on CT scan (B). ANT = anterior; POS = posterior; C = coronal.
MYOCARDIUM
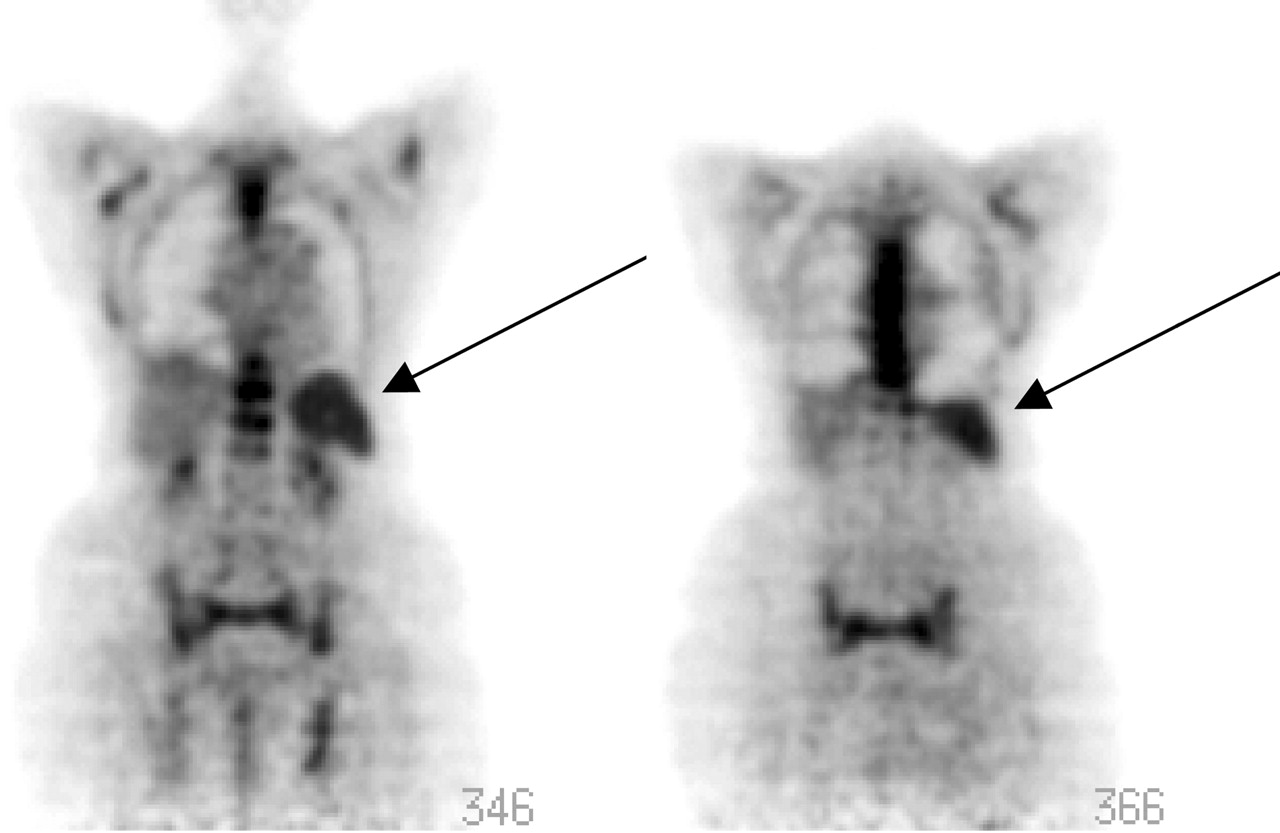
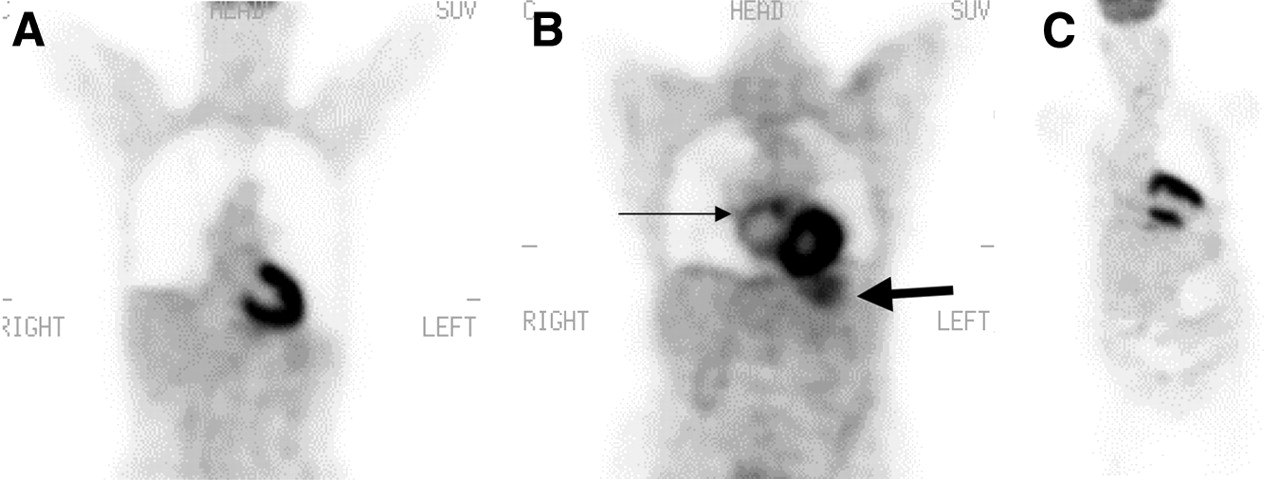
The myocardial uptake can vary significantly from one patient to another and in the same patient imaged on different occasions. During the fasting state, the myocardium depends on fatty acids to produce energy (21). For this reason we should not expect to see much myocardial uptake. On the other hand, in the postprandial state, the myocardial uptake could be enhanced significantly (Figs. 6A–6C). However, in spite of the patient’s fasting, we see many variations in the uptake, which range from absent to very intense uptake within the left ventricle, and occasionally we see intense uptake within the right ventricle as well. In some pathologic conditions we see even atrial uptake (Fig. 6B).

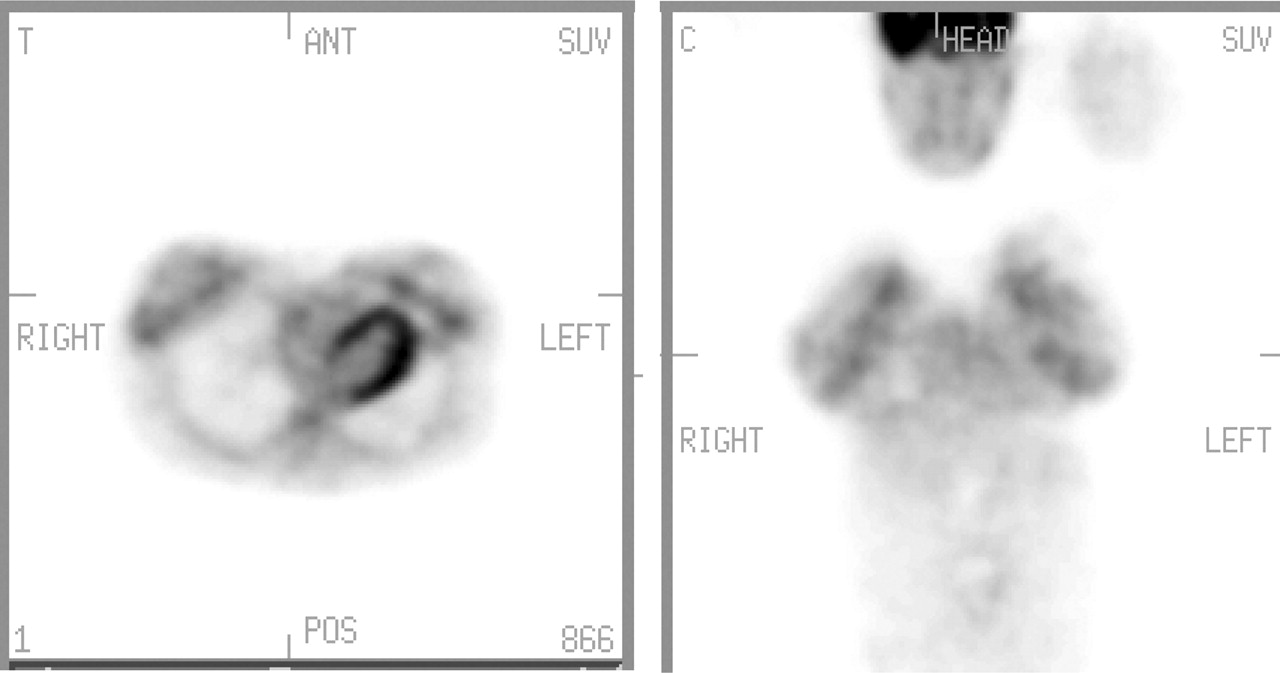
(A) Cardiac uptake: Normal physiologic intense 18F-FDG uptake throughout myocardium. (B) Atrial uptake: Note inhomogeneous mild 18F-FDG uptake in enlarged right atrium resembling abnormal mediastinal nodal tissue uptake. Thick arrow points out normal stomach uptake. (C) Cardiac uptake: Apical scar with aneurismal formation.
Sometimes the heart is not recognized for what it is. Inhomogeneous myocardial uptake and segmental absence of uptake attributed to previous myocardial infarction and scar formation (Fig. 6C) can cause confusion when interpreting the study.
GASTROINTESTINAL TRACT
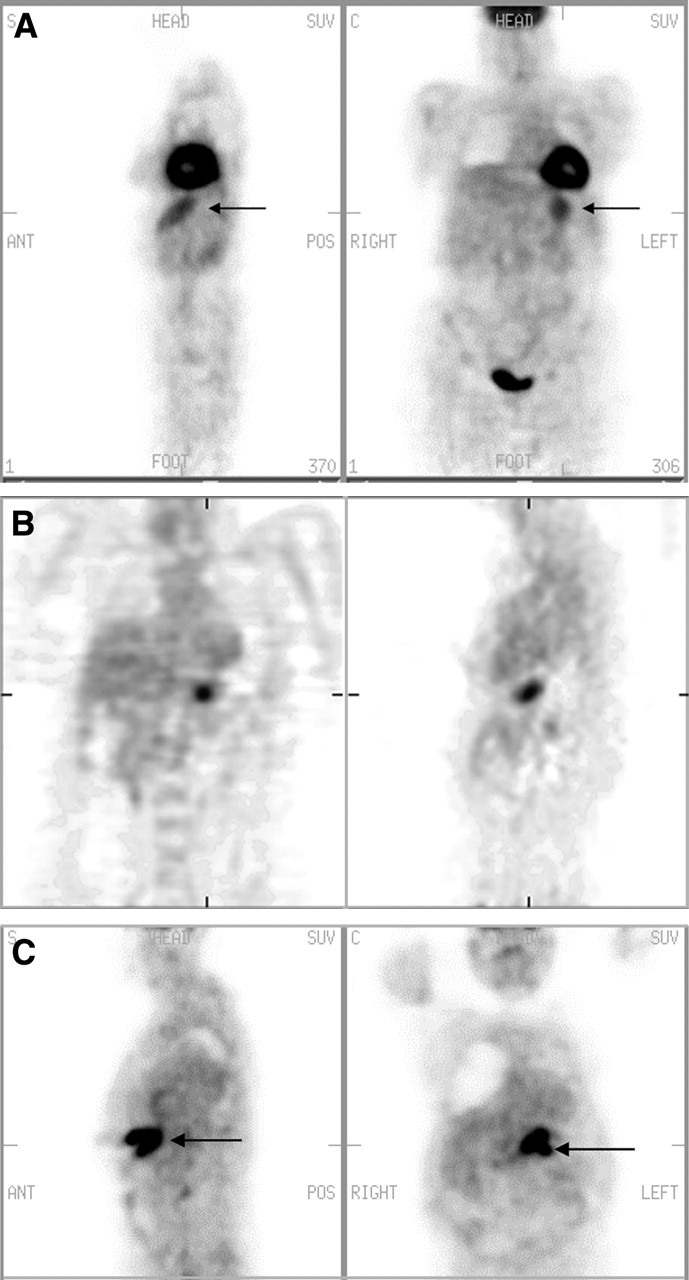
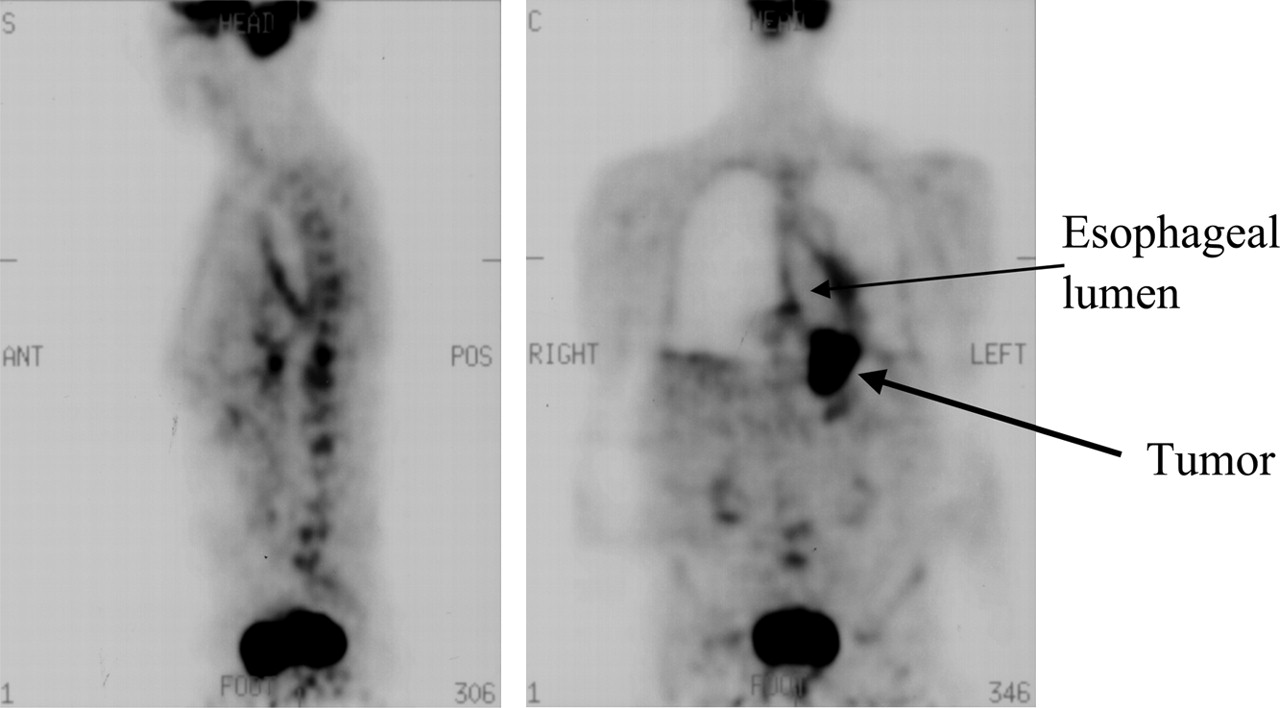
The origin of 18F-FDG uptake in the digestive tract is unknown; possible causes are active smooth muscle, metabolically active mucosa, swallowed secretions, or colonic microbial uptake (22). Gastric activity can be seen and has a characteristic J-shape within the left upper abdomen. The uptake can be faint or it can be intense (Fig. 7). Although less common, esophageal activity canbe seen as a mild linear uptake anterior to the spine, mostly due to swallowed saliva and partially due to smooth muscle metabolism. Prominent esophageal uptake is abnormal (Figs. 8 and 9). The colonic activity is also variable, ranging from faint heterogeneous activity, to mild focal, segmental, or diffuse activity (Fig. 10). Uptake in the cecum and right colon is usually higher than the rest of the colon because of the abundance of the lymphocyte cells, which are very glucose avid (Fig. 11). However, focal intense activity in the colon should be further evaluated with colonoscopy to exclude a neoplastic process. In some patients, the colonic uptake can cause a great clinical challenge, especially in the lower rectal region. By reviewing the sagittal and the rotating images, one can, in most cases, eliminate any pathologic uptake. The liver uptake is mostly faint and homogeneous. An overlapping loop of bowel can occasionally resemble a focal liver lesion; reviewing the corresponding CT slice can easily differentiate between the 2 conditions.
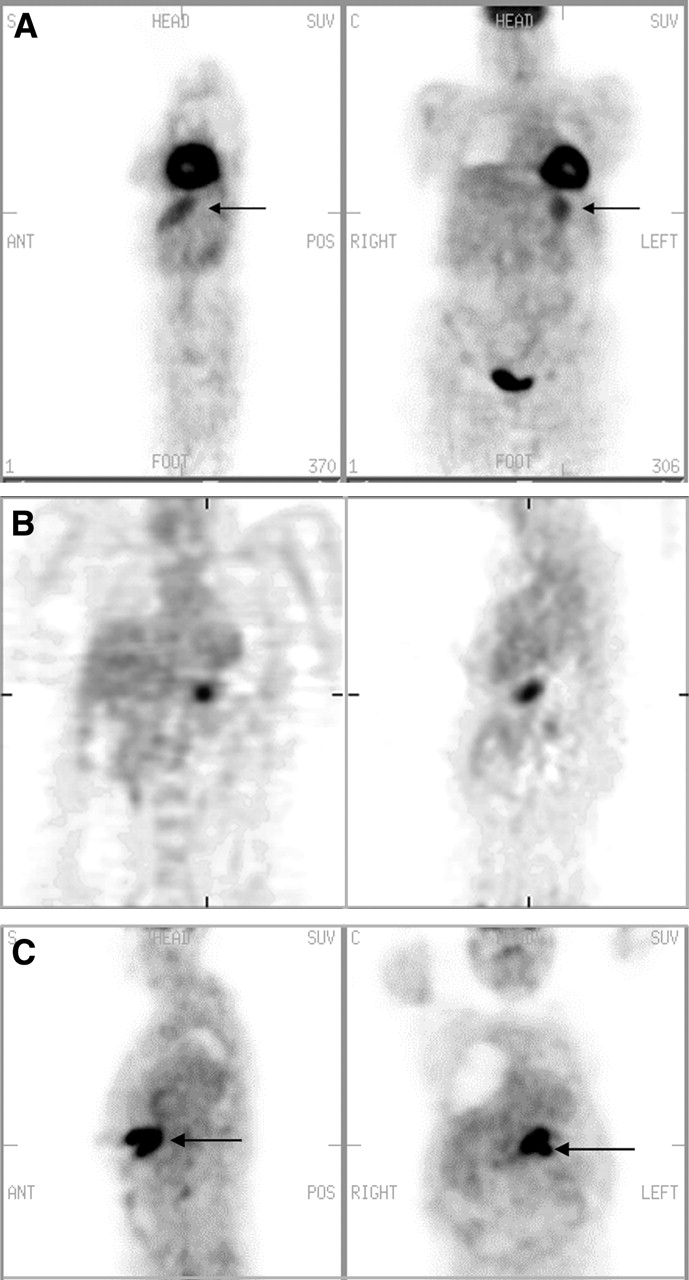
Stomach uptake. (A) Normal uptake: mild diffuse uptake (arrows) conforming to stomach configuration. (B) Adenocarcinoma of stomach: focal uptake in region of stomach. Coronal view on left; sagittal view on right. (C) Stomach lymphoma: intense focal uptake (arrows). S = sagittal; C = coronal; ANT = anterior; POS = posterior.
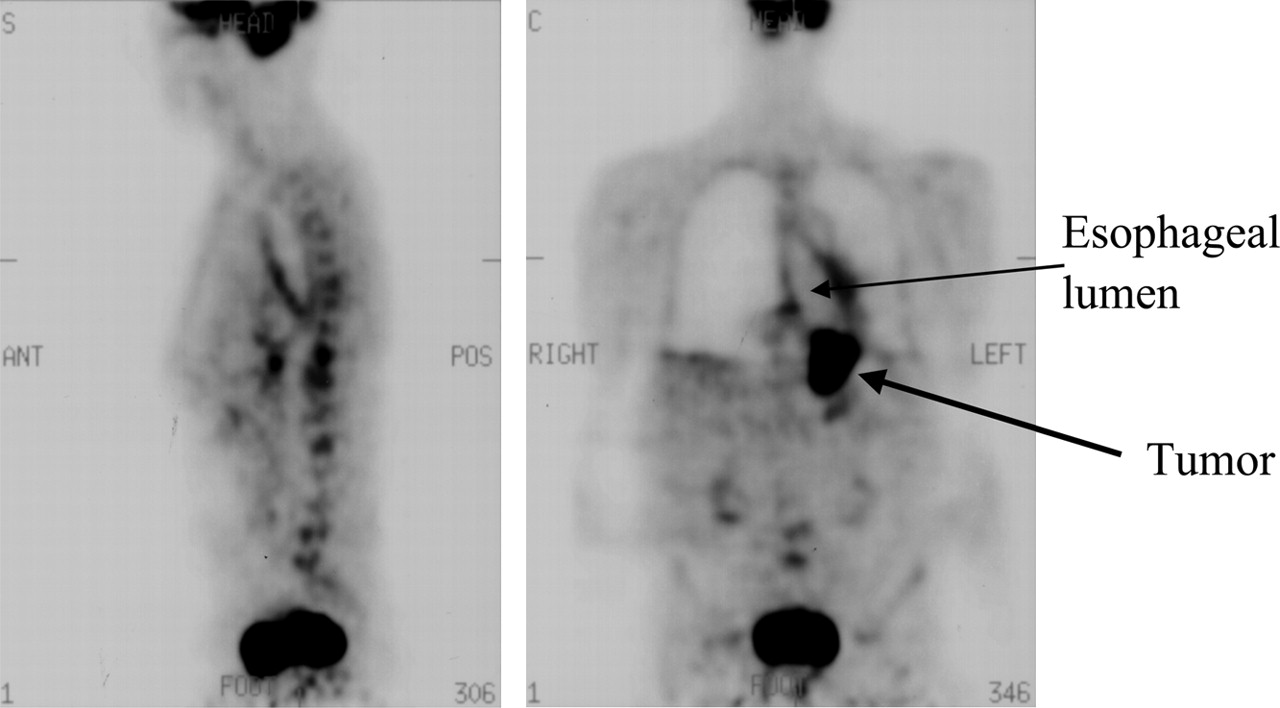
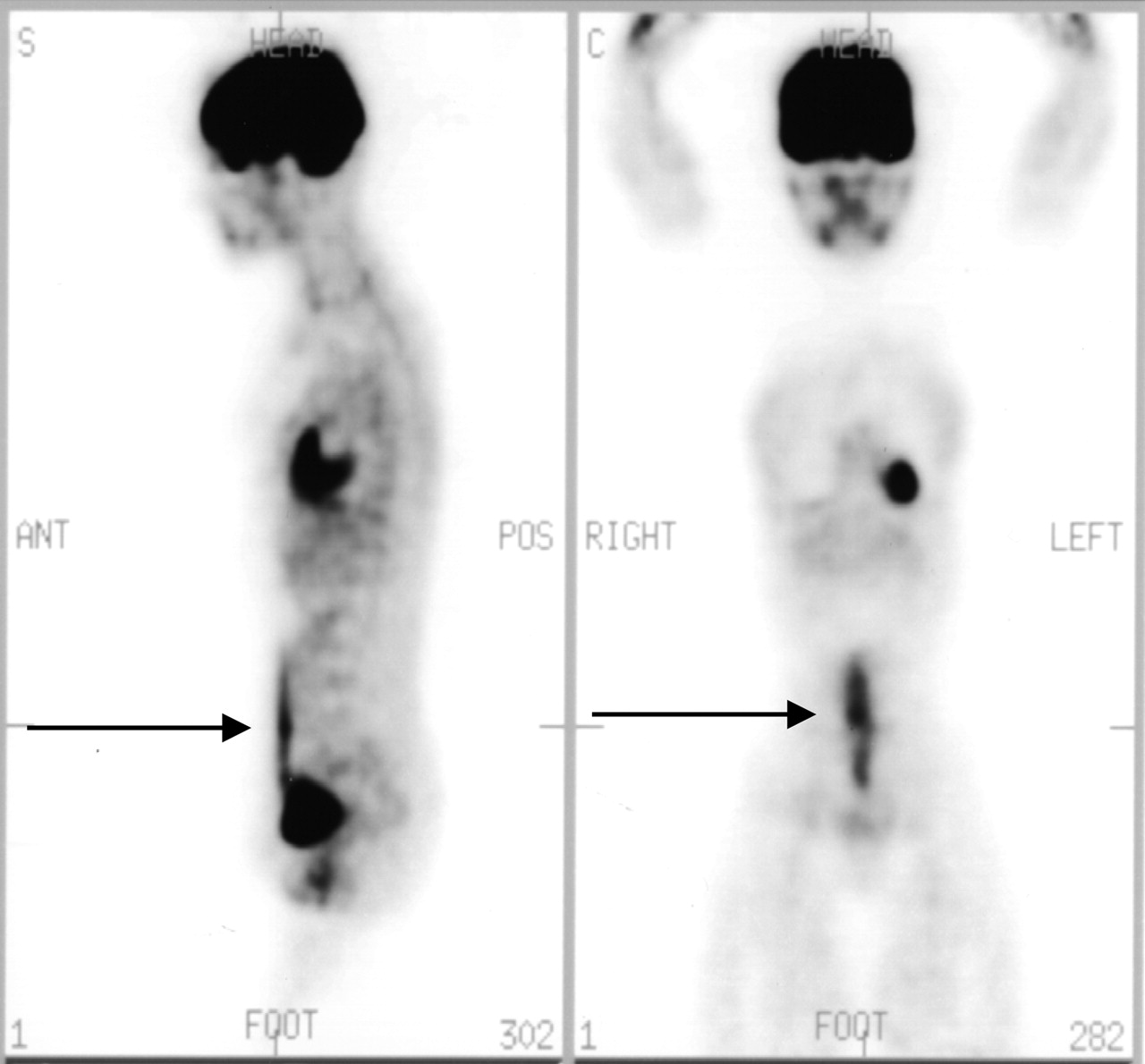
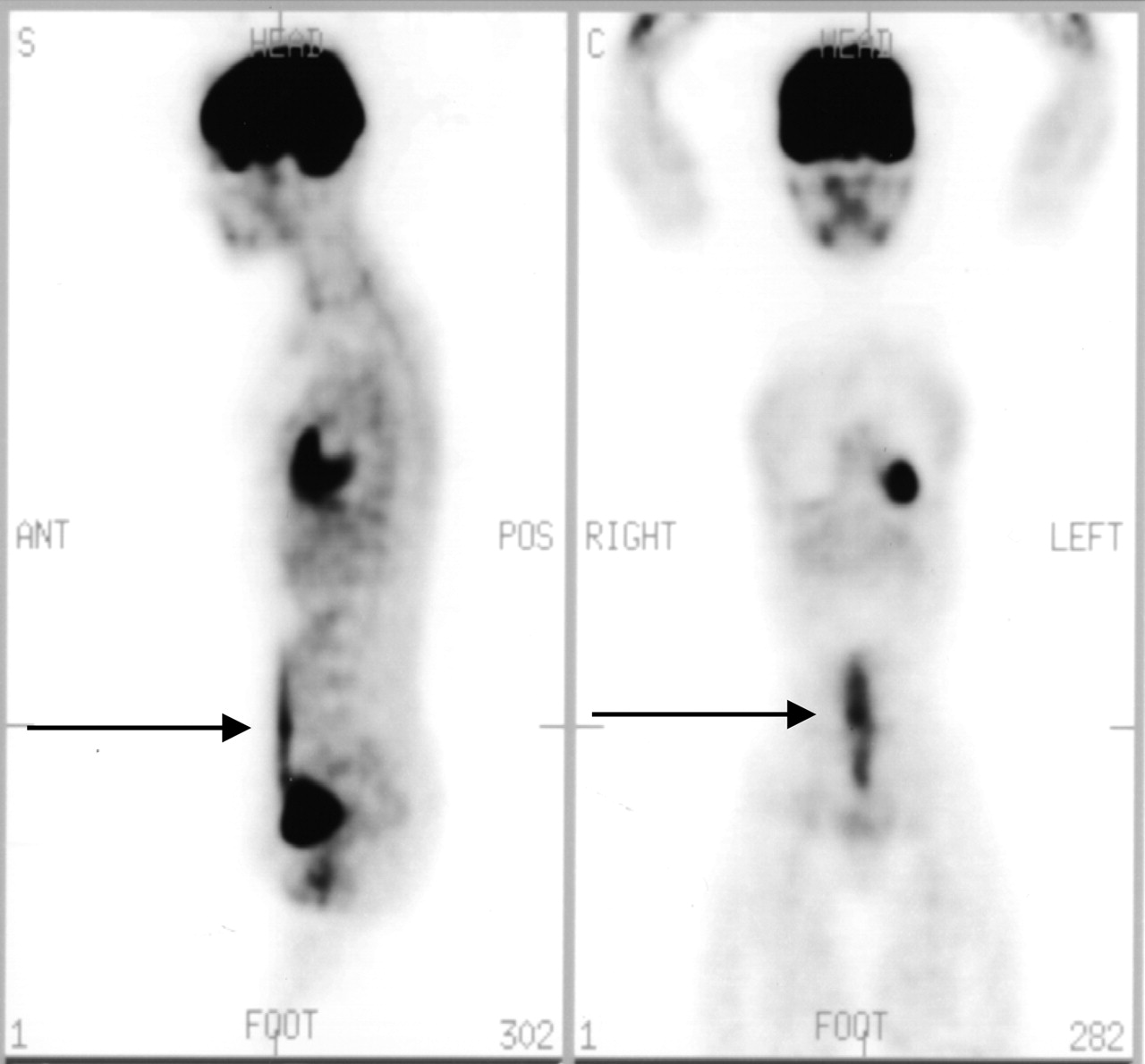
Dilated esophagus. A 72-y-old man with known esophageal carcinoma. Note dilated esophagus with linear increased uptake on both sides. Chronic dilation is due to distal obstruction by tumor mass. Linear uptake is due to reactive inflammation. ANT = anterior; POS = posterior; S = sagittal; C = coronal.
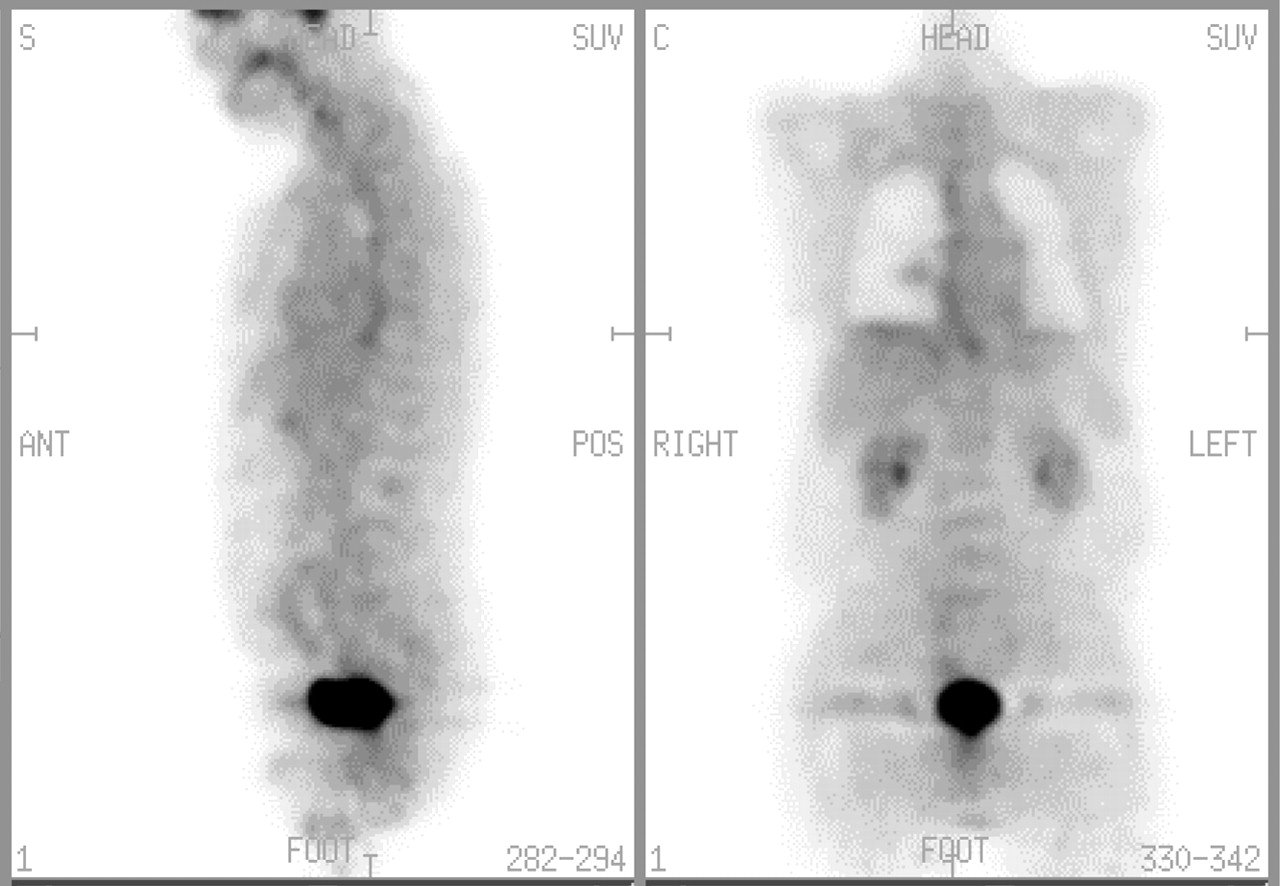
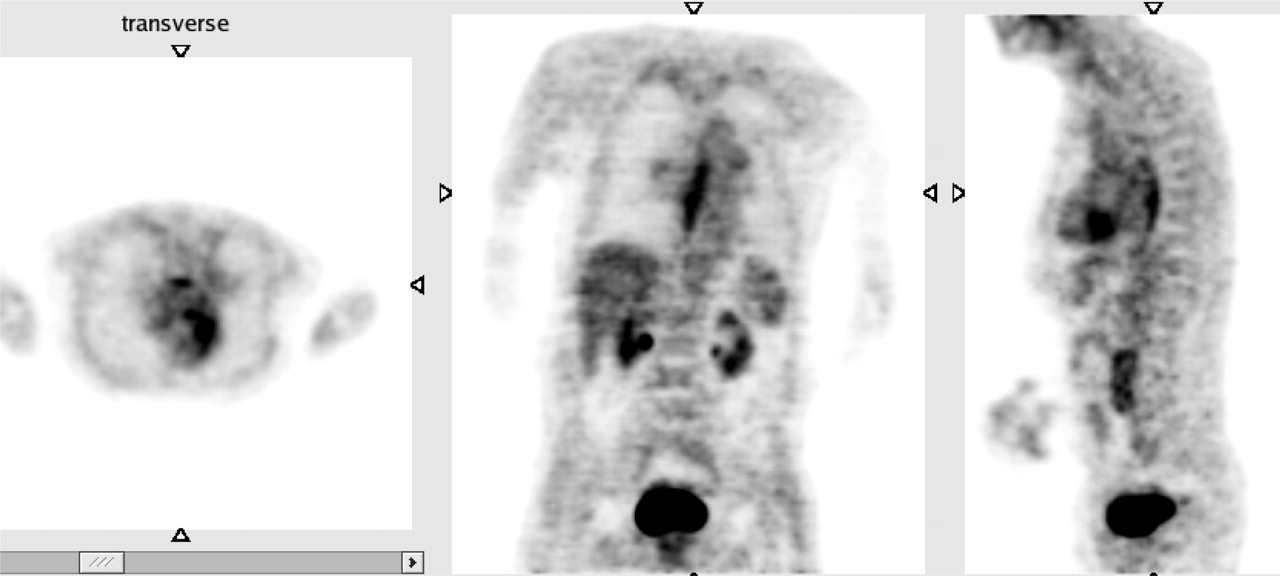
Esophageal uptake. Esophageal uptake in patient with gastroesophageal reflux disease. S = sagittal; C = coronal; ANT = anterior; POS = posterior.

Colonic activity (projection view). Patient had bladder cancer, status post cystostomy, and ileal conduit. PET was done to rule out pelvic recurrence. Note nonspecific diffuse colonic activity (a), ileal conduit (b), urinary bag (c), and area of recurrence (d).

Cecal uptake. (A and B) Normal diffuse physiologic uptake (arrow) in cecum. C = coronal.
GENITOURINARY
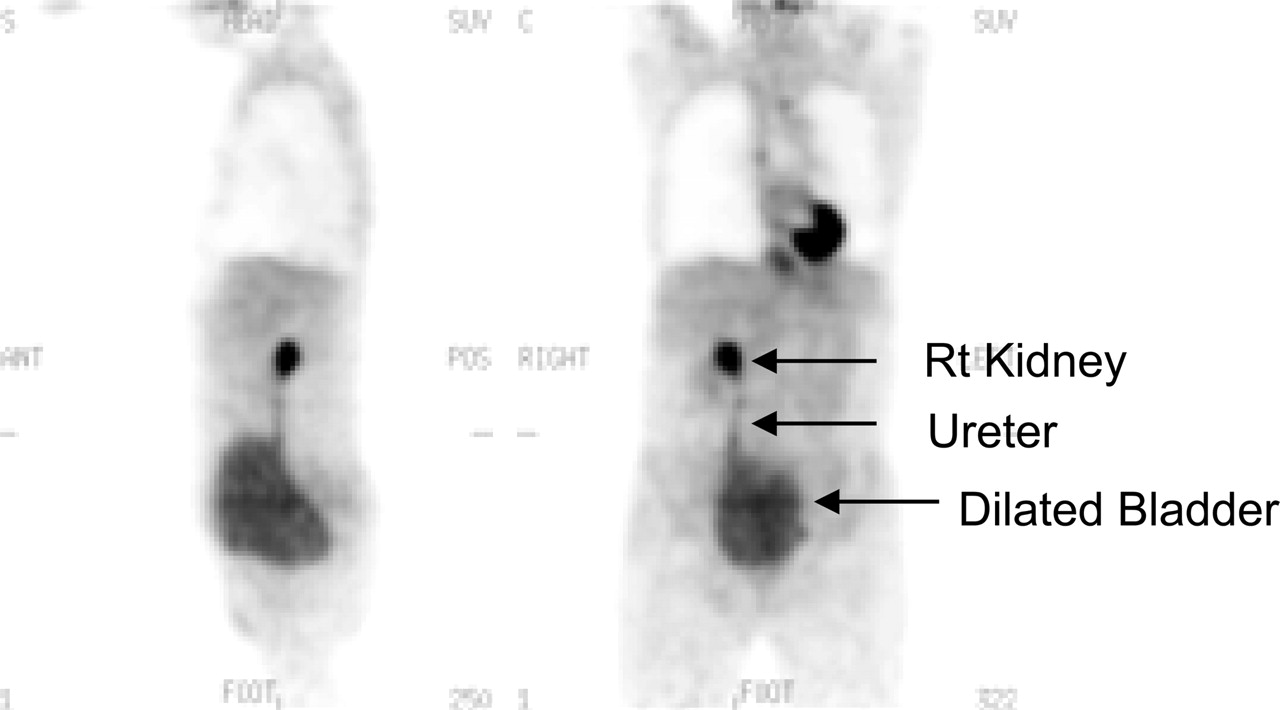
Because FDG is filtered through the glomeruli, without reabsorption unlike glucose, one should see the activity within the collecting system, ureters, and urinary bladder. Hydration and frequent voiding promote diuresis and help to decrease the radiation dose to the genitourinary tract. Congenital urinary malformation and acquired structural deformity as in postsurgical intervention can create artifacts (Figs. 12, 13, 14, and 15).
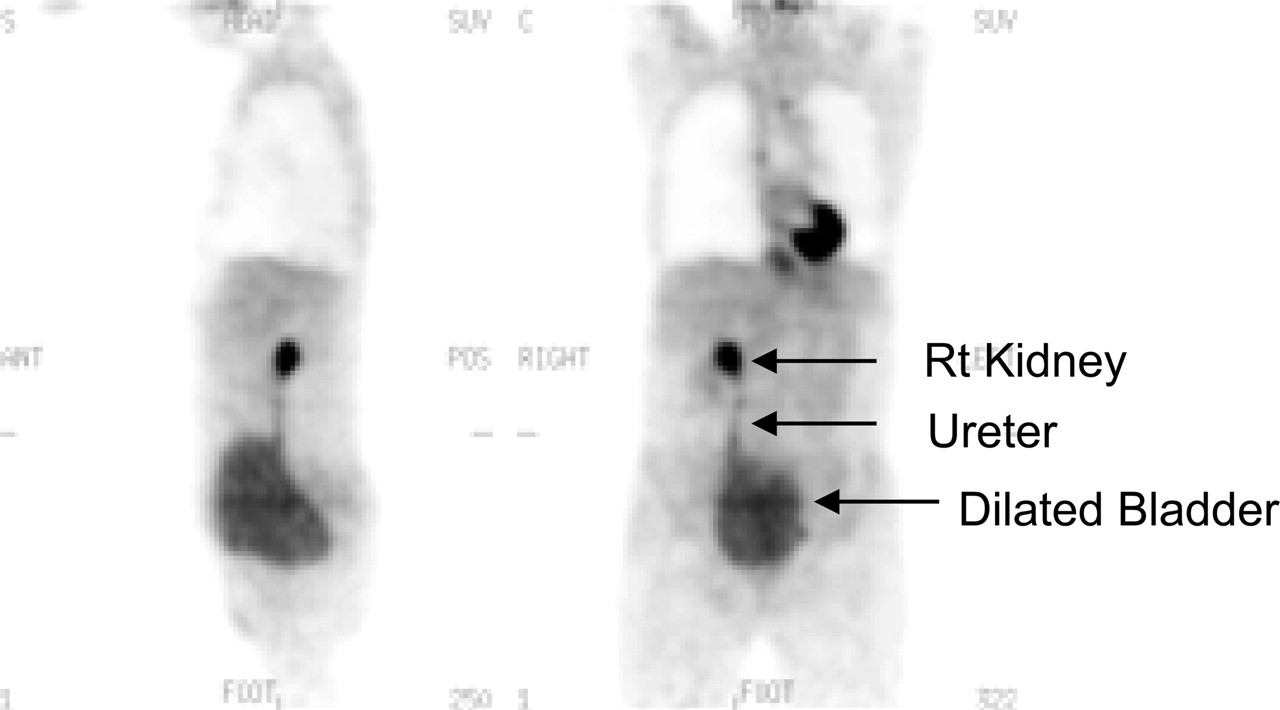
Dilated urinary bladder. Note prominent right (Rt) kidney collecting system, right ureter, and dilated urinary bladder.
Horseshoe kidney. (A) Horseshoe kidney (arrow) seen on 18F-FDG PET scan (projection view on left). Patient with Hodgkin’s lymphoma. (B) 99mTc-Glucoheptonate scan confirms presence of horseshoe kidney.
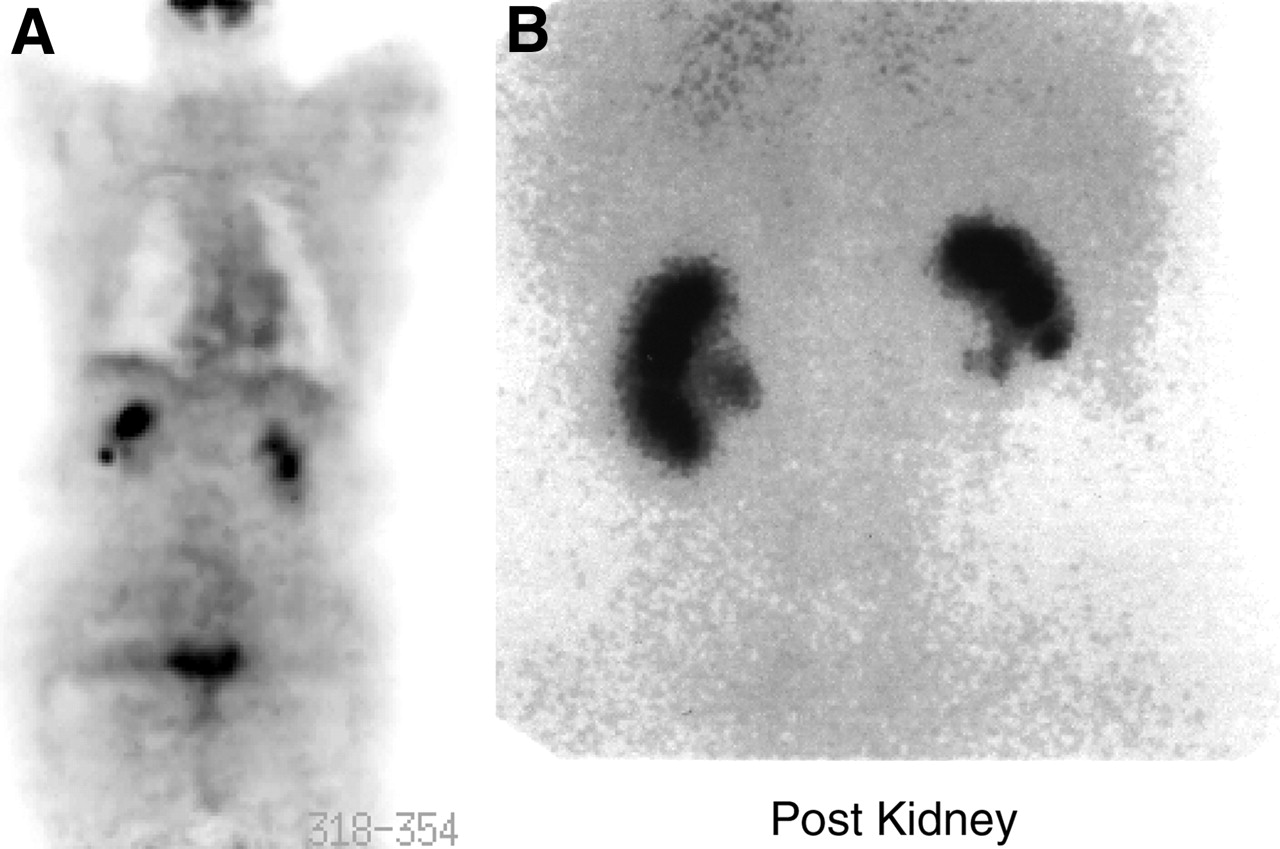
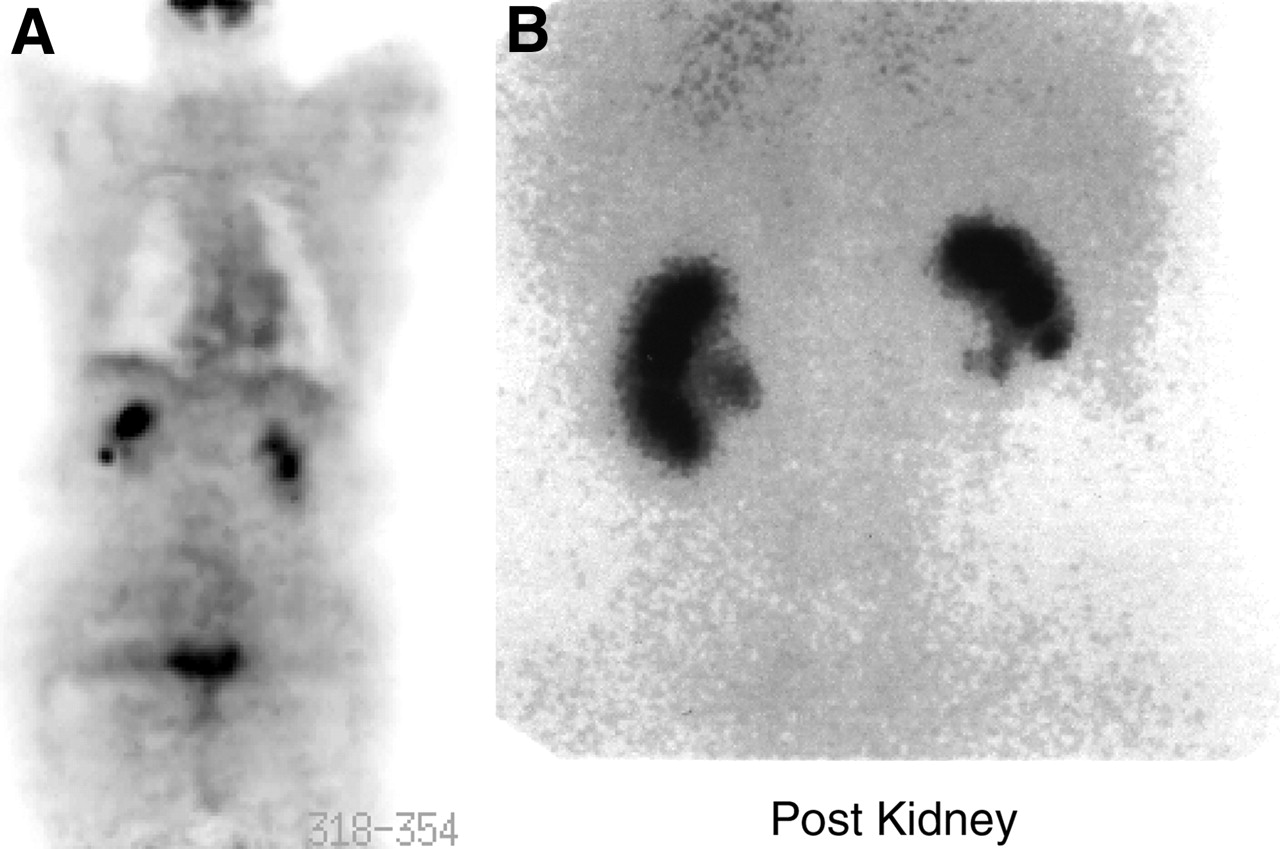
Renal activity. (A) Intense activity in right kidney collecting system overlapping right lobe of liver, simulating a liver lesion. (B) 99mTc-Dimercaptosuccinic acid image of same patient confirms that right kidney is slightly higher than left. Post = posterior.
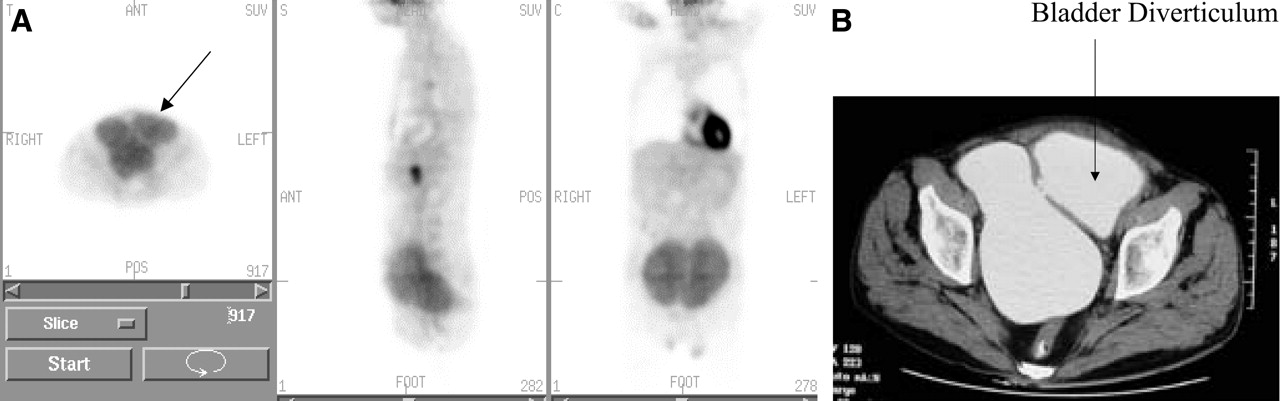
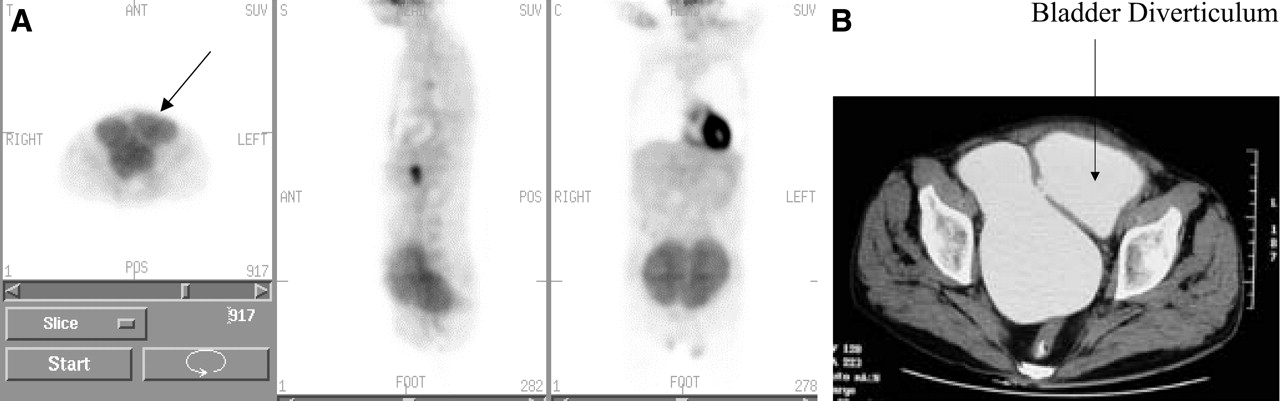
Bladder diverticulum. (A) Bladder diverticulum caused by chronic bladder outlet obstruction by hypertrophied prostate. (B) Corresponding CT scan. ANT = anterior; POST = posterior; S = sagittal; C = coronal.
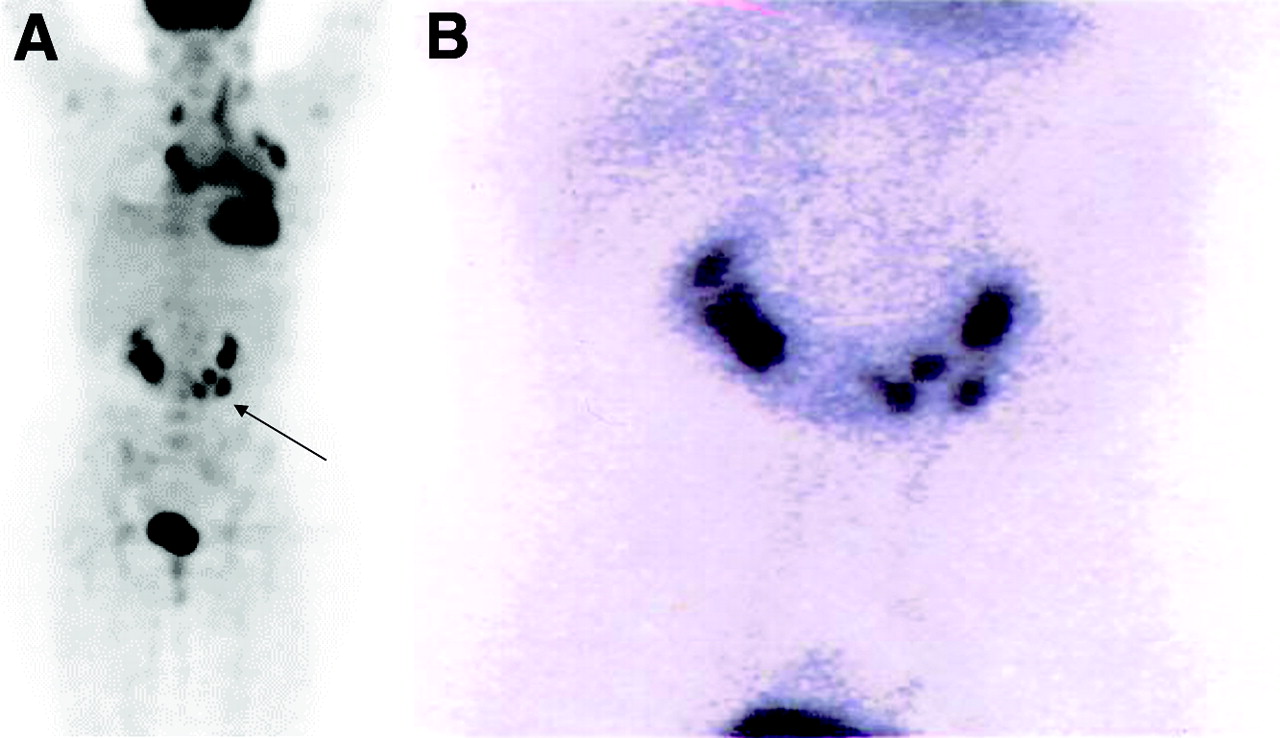
For example, a horseshoe kidney, congenital pelvic kidney, and transplanted kidney can simulate neoplastic lesions. Furthermore, focal urinary activity within the ureter can also simulate focal nodal neoplasia. One must also be aware of urine contamination and surgical tubes draining the kidney (Fig. 16).
(A) Nephrostomy tube (arrow). (B) Diaper artifact. POS = posterior.
Increased 18F-FDG uptake has been reported in the normal uterus during menstruation (23,24), in a follicular ovarian cyst (25), and in the ovary with an inflammatory reaction during ovulation (26). In a recent study by Nishizawa et al. (27), the authors observed distinct ovarian 18F-FDG uptake with an SUV of 3.9 ± 0.7 in 26 of 32 premenopausal women examined during the late follicular to early luteal phase of the menstrual cycle. Eighteen of the 32 women also showed focal 18F-FDG uptake in the endometrium, with an SUV of 3.3 ± 0.3. On the other hand, all 9 women in the first 3 d of the menstrual cycle demonstrated intense 18F-FDG uptake in the endometrium, with an SUV of 4.6 ± 1.0. The authors concluded that in women of reproductive age, 18F-FDG imaging should preferably be done within a week before or a few days after the menstrual flow phase to avoid any misinterpretation of pelvic 18F-FDG PET images (27).
MUSCULAR ACTIVITY
Vigorous exercise in the days just before a scan can cause intense uptake in the associated skeletal muscles. Skeletal muscle uptake could be enhanced not only because of exercise activity but also because of stress-induced muscle tension as is often seen in the trapezius and paraspinal muscles. Hyperventilation may induce uptake in the diaphragm as well.
Muscle uptake is typically symmetric, mild-to-moderate linear activity (Figs. 17 and 18). However, occasionally the uptake can be focal and unilateral, which could create a diagnostic challenge, especially in head and neck cancer and lymphoma. Similarly, the use of insulin to adjust the serum glucose level immediately before injection of 18F-FDG can result in 18F-FDG accumulation in skeletal muscle. Benzodiazepines may be used to decrease paraspinal and posterior cervical muscle uptake in tense patients.
Muscle uptake. Symmetric muscle uptake in neck (arrows). C= coronal.

Intercostal muscle uptake due to persistent coughing (projection view).
In addition to the muscles, increased 18F-FDG uptake can be seen in the adipose tissue of the neck, supraclavicular regions, around the large vessels in the mediastinum, the axillae, the perinephric regions, and in the intercostal spaces along the thoracic spine in 3.7% of patients undergoing 18F-FDG PET, constituting a potential source of false-positive PET (28). Uptake in the neck adipose tissue is typically bilateral and symmetric, intense, and more often multifocal than linear (29) (Fig. 19).

Brown fat uptake. (A) Asymmetric neck uptake (arrows). (B) Intense symmetric uptake in adipose tissue (arrows). Brown fat can cause difficulty in scan interpretation. C = coronal.
THYMUS UPTAKE
Thymus uptake is a normal finding in children and young adults, appearing as an upside down letter V. Also, thymus hyperplasia after chemotherapy is a normal variant in the adult population as well (25,30) (Fig. 20).

Thymus uptake (coronal views). (A) Diffuse thymus uptake (arrow). (B) Focal thymus uptake (arrow).
BONE MARROW
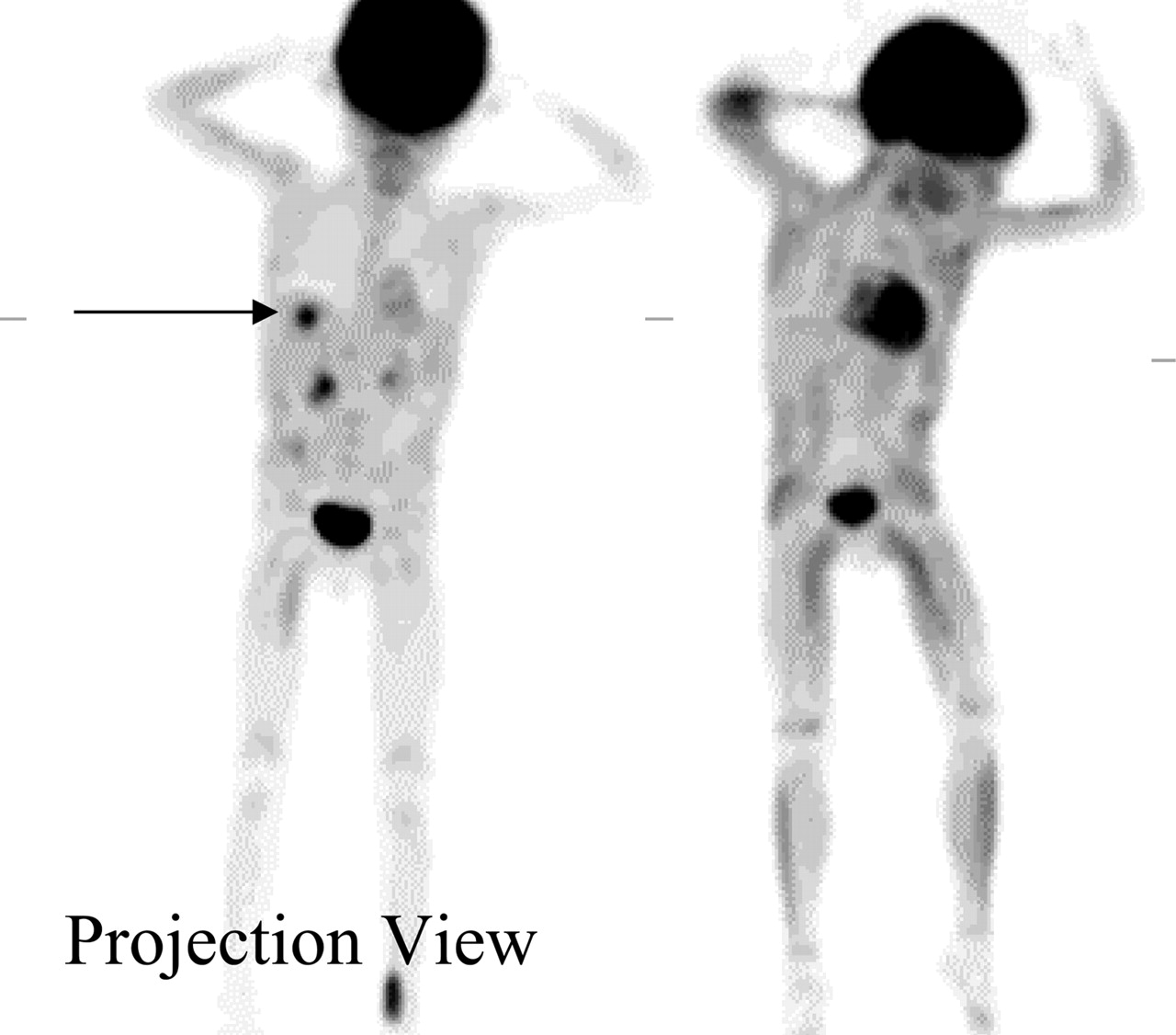
Bone marrow accumulation of 18F-FDG is generally faint diffuse low-grade activity, less than liver activity and mostly seen in vertebral bodies. Focal activity within bone marrow is always suspicious for an abnormality. Uniform diffuse increased bone marrow activity can be seen also with bone marrow recovery after chemotherapy, which usually resolves by 1 mo after therapy (31).
Increased diffuse intense 18F-FDG uptake in the bone marrow (Fig. 21) has been reported in patients taking hematopoietic growth factors (HGF), granulocyte-macrophage colony-stimulating factor (GM-CSF), granulocyte colony-stimulating factor (G-CSF), and erythropoietin (31,32). In a study by Yao et al. (33), administration of G-CSF caused 18F-FDG uptake to increase to 97% above baseline on day 3 of therapy and to 170% above baseline on day 10 of therapy. Sugawara et al. showed that 18F-FDG uptake of bone marrow declined after G-CSF was completed but remained higher than baseline for almost 4 wk after completion of G-CSF (31). The identification of bone metastases could be a challenging task in this group of patients. Therefore, depending on the clinical situation, waiting for 2–4 wk before performing the 18F-FDG study is advised.

Bone marrow. Intense 18F-FDG uptake in bone marrow is attributed to hematopoietic growth factor.
SPLENIC UPTAKE
Normally, there is faint uptake of 18F FDG in the spleen. Because the spleen is an active site for the extramedullary hematopoiesis, one would expect to see a diffuse enhanced 18F-FDG uptake in conjunction with diffuse bone marrow uptake after administration of HGF, such as G-CSF and erythropoietin (Fig. 22) (32,34). Similarly; other hematologic diseases such as thalassemia, which can cause extramedullary hematopoiesis, can also lead to enhanced 18F-FDG uptake in the spleen (35). Furthermore, other nonneoplastic conditions such as infection can cause diffuse enhancement of glucose uptake within the spleen.
Spleen uptake (arrows) due to hematopoietic growth factor.
BENIGN PATHOLOGIC CAUSES OF 18F-FDG UPTAKE
18F-FDG is not a tumor-specific probe. In addition to its physiologic accumulation in different organs, it can accumulate in nonneoplastic pathologic conditions, including infection (36–40), whether acute or chronic infection such as tuberculosis, granulomatous diseases such as sarcoidosis (38,41,42), and autoimmune disease such as Grave’s disease (43,44) (Figs. 23 and 24). In addition, the 18F-FDG uptake can be enhanced by inflammatory induced changes, which include postoperative healing scars and postradiation therapy (Figs. 25, 26, 27, and 28). A unique example of an inflammatory condition is the one caused by the atherosclerotic plaque formation that is associated with an abundance of macrophages known by its avidity to 18F-FDG (45–47) (Fig. 29). The degree of uptake is usually less than the uptake within the neoplastic tissues. However, there is clearly an overlap between the 2 conditions and, in some cases, the uptake could even exceed the neoplastic uptake. Furthermore; the image interpreter should be aware of a high accumulation of 18F-FDG in some benign tumors, such as giant cell tumor, fibrous dysplasia of the bone, and adenomatous polyps in the colon (48,49).

18F-FDG uptake in lymph nodes attributed to tuberculosis (projection view).
Fungal infection in liver of pediatric patient. (A) Before therapy (arrow). (B) Infection resolved on image after specific antifungal therapy.
Scar tissue from recent surgery. Patient underwent recent abdominal surgery for hernia repair. Note linear superficial increased 18F-FDG uptake along anterior abdominal wall conforming to abdominal scar tissue (arrow). S = sagittal; C = coronal; ANT = anterior; POS = posterior.

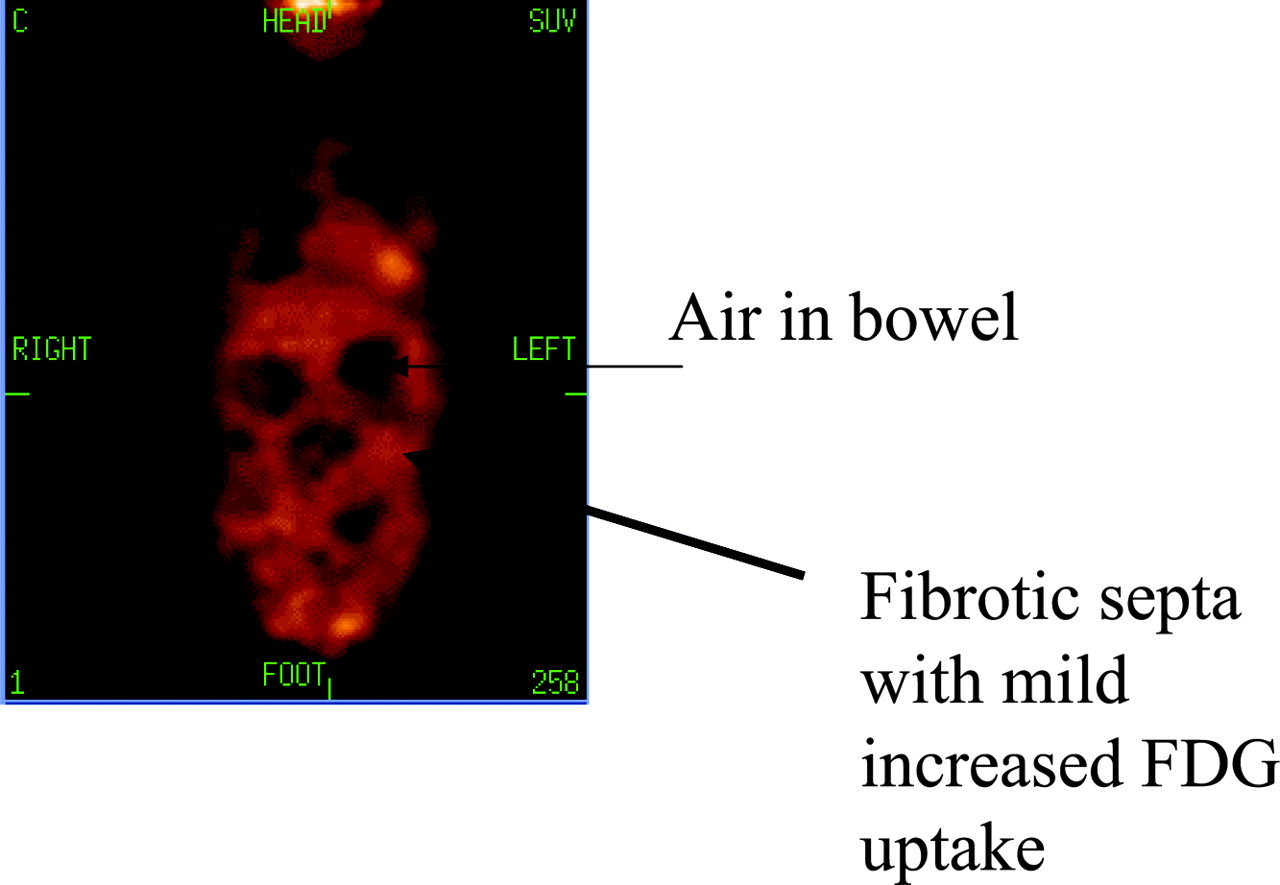
Abdominal fibrosis, honeycomb appearance. Patient had history of multiple abdominal surgeries leading to scattered segmental fibrosis. Image shows mild 18F-FDG uptake between dilated loops of bowel forming the honeycomb appearance. C = coronal.

Uptake in sternum after coronary artery bypass grafting. Patient had open-heart surgery 1 wk before 18F-FDG study. S = sagittal; C = coronal.
Postsurgical hematoma (arrows). Patient had excisional breast biopsy 10 d before 18F-FDG scan. ANT = anterior; POS = posterior; S = sagittal; C = coronal.
Intense aortic uptake due to inflammation (unstable plaque formation).
Occasionally one will also see breast-related activity. Breast activity will be more obvious in lactating females (Fig. 30).
Breast uptake, lactating female. ANT = anterior; POS = posterior; C = coronal.
CONCLUSION
In recent years 18F-FDG PET has become an essential tool in the management of cancer patients. To optimize its appropriate interpretation, one must understand the normal physiologic distribution and different confounding artifacts. Proper patient preparation and a complete patient history are needed to accurately interpret the scan and also to avoid the artifacts.
Acknowledgments
The authors acknowledge the following technologists: Paul Galantowicz, Scott Wisniewski, Debbie Erb, and Kimberly Dix. Also, images in Figures 3B, 18, and 23 are courtesy of Drs. Jayakumari Gona and Dr. Syed Husain at the Western New York Veterans Healthcare Hospital System.
Footnotes
For correspondence or reprints contact: Elpida S. Crawford, MS, Nuclear Medicine Department, University at Buffalo, 105 Parker Hall, 3435 Main St., Buffalo, NY 14214-3007.
E-mail: esc{at}buffalo.edu
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH SEPTEMBER 2006.
REFERENCES





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Noninvasive brain cancer imaging with a bispecific antibody fragment, generated via click chemistry
- Stratification of 18F-Labeled PET Imaging Agents for the Assessment of Antiangiogenic Therapy Responses in Tumors
- Multimodal Assessment of In Vivo Metabolism with Hyperpolarized [1-13C]MR Spectroscopy and 18F-FDG PET Imaging in Hepatocellular Carcinoma Tumor-Bearing Rats
- Could Different Hydration Protocols Affect the Quality of 18F-FDG PET/CT Images?
- Assessment of a New 18F-FDG PET/CT Protocol in the Staging of Oral Cavity Carcinomas
- Uncommon Reason for High Fluorodeoxyglucose Positron Emission Tomography Uptake
- A "fat chance" it's malignant: lipoid pneumonia simulating lung cancer on PET scan
- Pediatric PET/CT Imaging: Tips and Techniques
- A "fat chance" it's malignant: lipoid pneumonia simulating lung cancer on PET scan
- Forced Diuresis Improves the Diagnostic Accuracy of 18F-FDG PET in Abdominopelvic Malignancies