


Abstract
Although bone scanning is a test primarily concerned with skeletal abnormalities, important nonosseous findings are occasionally present on the images. To gauge the significance of such nonosseous uptake and, in particular, to determine whether these findings contain useful diagnostic information, the technical and medical staff in nuclear medicine must recognize the various patterns of nonbony uptake and understand their causes. The objectives of this article are to demonstrate the appearances of nonosseous uptake on bone scans, to categorize the forms of soft-tissue uptake, to emphasize technical artifacts leading to soft-tissue uptake, and to highlight the clinical significance of pathologic soft-tissue uptake.
Bone scanning using the 99mTc-phosphate analogs is an established diagnostic modality for a variety of pathologies involving the skeleton, such as osteomyelitis, bony metastases, and occult fractures. Technically, scanning is performed using different imaging protocols depending on the indication for the scan. For instance, multiphase bone scanning is performed to image osteomyelitis; whole-body imaging, to image metastatic bone disease; and SPECT, to localize abnormalities in 3 dimensions for spine or hip lesions. The appearance of both skeletal and soft-tissue uptake depends heavily on imaging technique, and the practitioner should be aware of the impact of technical factors on image quality (1,2). The bone scan is interpreted by evaluating the pattern of radioactive localization in the bones and identifying areas of increased uptake (hot spots) or, less frequently, decreased or absent skeletal uptake. In addition, allowance is made for the normal uptake in the kidneys and urinary tract due to excretion of the radiopharmaceutical with subsequent drainage into the urine. Renal function and metabolic status of the patient also strongly affect the scan appearance of both skeletal and soft-tissue uptake (3).
In certain conditions, nonosseous structures other than the urinary tract are seen on the bone scan. For example, there may be localized muscle uptake, such as myositis ossificans, or localization in a pleural effusion. Such serendipitous findings may constitute welcome diagnostic information. On the other hand, soft-tissue uptake may at times hamper interpretation of the study by bringing in artifacts that degrade the quality of the images. Therefore, recognition of patterns of nonbony uptake is important for correct identification of artifacts and accurate interpretation of the scan.
In this article, an examination of nonosseous abnormalities on bone scans is presented. The review is based on the authors’ own experience and on a summary of the medical literature. Soft-tissue abnormalities are divided into 3 classifications: technical artifacts, urinary tract findings, and uptake in other soft tissues or viscera.
TECHNICAL ARTIFACTS
Artifacts related to poor technique are commonly observed on bone scans. Recognition of these “abnormalities” will lead in most cases to rectification of the error and, thereafter, acquisition of the appropriate study. Technical artifacts can be divided further into those related to the radiopharmaceutical, injection technique, or imaging process.
Radiopharmaceutical
A faulty radiopharmaceutical preparation can lead to altered biodistribution of 99mTc-methylene diphosphonate (MDP), markedly affecting the diagnostic image (4). Additional structures not usually seen on the scan will be identified, such as gastric uptake due to free 99mTc-pertechnetate (5). Faulty preparation such as occurs when aluminum ions are present (6), when dextrose solutions are added (7), when a preparation is left unused for a long time (8), or when an inappropriately high pH is present in the reaction mixture (9) will result in unintended soft-tissue uptake. The uptake of radioactivity in bone may be affected to such an extent that interpretation of the scan becomes impossible. Other situations leading to uninterpretable bone scans will be encountered in patients on medications that alter the distribution of the 99mTc-phosphate compound; for example, the diphosphonates used for treatment of osteoporosis saturate the sites of 99mTc-MDP uptake on bone (10). To avoid such drastic concerns, one should check the patient’s medications for possible interaction with the radiotracer. In addition, special therapies or interventions should be recorded in relationship to the scan to clarify some unexpected findings on the images, such as renal cortical uptake due to iron overload or after chemotherapy (11,12). In Table 1, the effects on the bone scan of various radiopharmaceutical contaminants or drug interactions are listed.
Effects of Faulty Radiopharmaceutical Preparation on Bone Scan
Injection Technique
Rarely, extravasation at the site of injection of 99mTc-MDP may be confused with an abnormality on the bone scan: Marking injection sites will prevent such confusion. The pressure and motion generated during bolus intravenous injection can easily dislodge the needle from the vein, causing extravasation of the radioactivity into the surrounding soft tissue. For this reason, faulty intravenous injection is the most frequent cause of abnormal soft-tissue uptake on bone scans (13). Another much less frequent blunder due to a faulty injection technique is arterial puncture and intraarterial injection of the radiotracer (14). After intraarterial injection, the distal arterial distribution shows pronounced soft-tissue uptake. For example, injection of 99mTc-MDP into the radial artery produces dramatic uptake over the lateral side of the hand and wrist (Fig. 1).
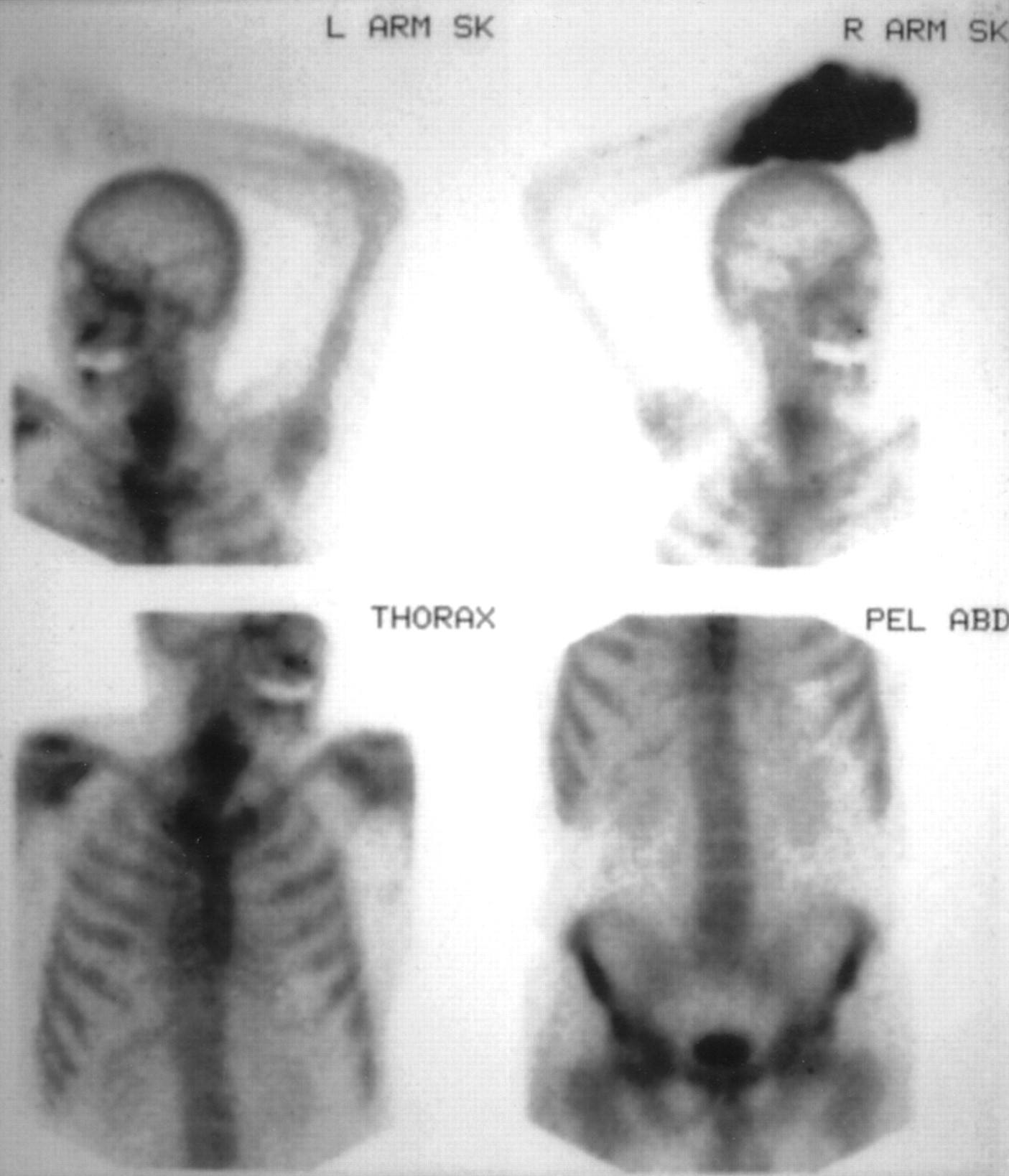
Injection of 99mTc-MDP into radial artery of right hand produces dramatic soft-tissue uptake in arterial distribution along lateral side of hand and wrist (anterior view). SK = skull; PEL ABD = pelvis and abdomen.
Imaging Process
Despite routine quality control testing, artifacts due to equipment failure or faulty technique remain unfortunately common (15). Equipment malfunction such as a camera badly out of tune or the use of the wrong flood correction map will produce a nonuniform appearance that simulates soft-tissue uptake. However, the most frequently encountered problem is patient motion, which at times can produce blurred structures on the image similar to soft-tissue uptake. Motion artifacts are particularly serious in SPECT reconstruction; therefore, routinely checking the raw projection data before discharge of the patient is important. Furthermore, when not adequately supervised, the patient may place an upper limb over the site that is being imaged, leading to mysterious structures superimposed on the abdomen or pelvis. Such artifactual nonosseous findings can be minimized by close monitoring of the progress of the scan. Finally, even when appropriately performed, the SPECT imaging process may at times lead to patterns of projected activity that cross the soft tissues. Streaks of increased activity and photopenia extending outward from a full bladder on bone SPECT of the pelvis are a good example of this pitfall (16).
NONOSSEOUS FINDINGS RELATED TO URINARY SYSTEM
The most frequent nonskeletal incidental findings on bone scans are related to the genitourinary system (17). Abnormalities of renal size, position, and structural integrity are identifiable on whole-body bone scans, and comments on the status of the kidneys and bladder have become a constant feature in bone scan reports. Examples of such findings range from the clinically insignificant (such as a ptotic kidney) to the photopenic kidney defect that proves to be cancer (Fig. 2) (18). In addition, findings related to the urinary collecting tracts, such as a dilated pelvicaliceal system, can be observed (19). For example, a patient with newly diagnosed prostate cancer who is undergoing bone scanning to exclude metastases may have the unexpected finding of a dilated, obstructed ureter (Fig. 3)—which the urologist may or may not have identified on prior studies such as contrast-enhanced CT. Whether incidental urinary findings bear any significance to the patient’s condition remains, however, controversial. In our own series (unpublished), the incidence of urinary tract findings was 15%. However, most of these findings were already known to be present before bone scanning. The evaluation of the genitourinary system on routine bone scans is crude and limited when compared with the renogram or CT scan. However, occasionally the patient’s diagnostic problem will be solved by carefully inspecting the genitourinary findings on a bone scan. For example, the bone scan may reveal an unknown renal problem, such as hydronephrosis, that could explain a patient’s low-back pain and lead the clinician to appropriate diagnostic testing and therapy (20).
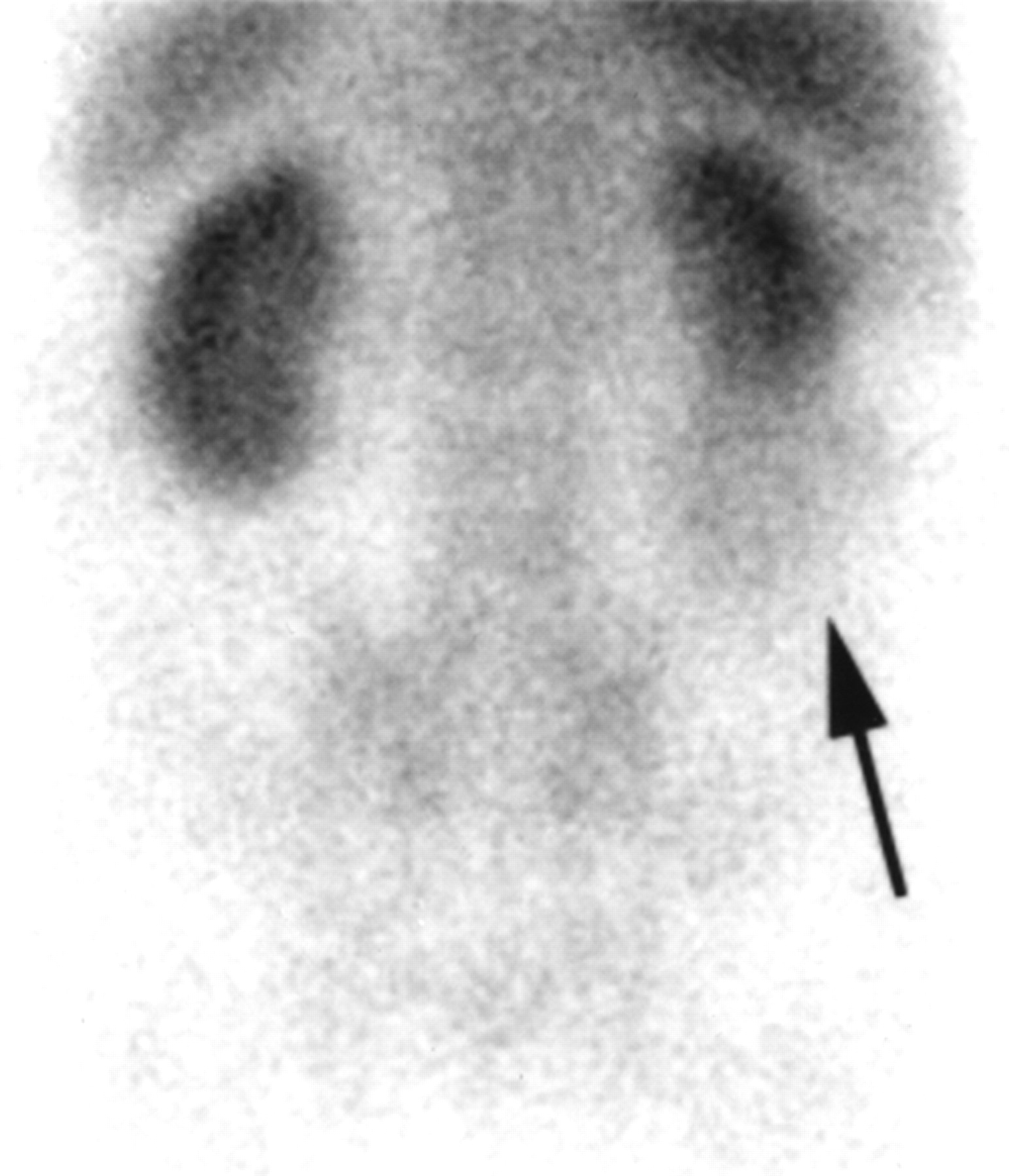
Blood-pool image of posterior lower back shows blunting of lower pole of right kidney and uptake in soft-tissue mass (arrow), which proved to be renal cell carcinoma.

Grossly dilated left ureter and renal collecting system seen on anterior whole-body 99mTc-MDP bone scan of patient with prostate cancer. Indwelling Foley catheter was in place at time of scanning.
SOFT-TISSUE FINDINGS ON BONE SCANS
A plethora of bone scan cases featuring soft-tissue or visceral uptake can be found in the medical literature. Such findings also occur frequently in one’s own clinical practice. Excluding the technical artifacts and the genitourinary causes already mentioned, various pathophysiologic mechanisms have been postulated for soft-tissue uptake. For example, deposition of the bone radiotracer in heterotopic new bone formation (e.g., myositis ossificans) follows a pathway similar to bone localization (21). Although bone scanning is frequently ordered for evaluation and follow-up of known heterotopic ossification (22), the incidental finding of uptake around the joints and in certain muscles can be a prelude to clinical presentation of heterotopic ossification in these cases (23).
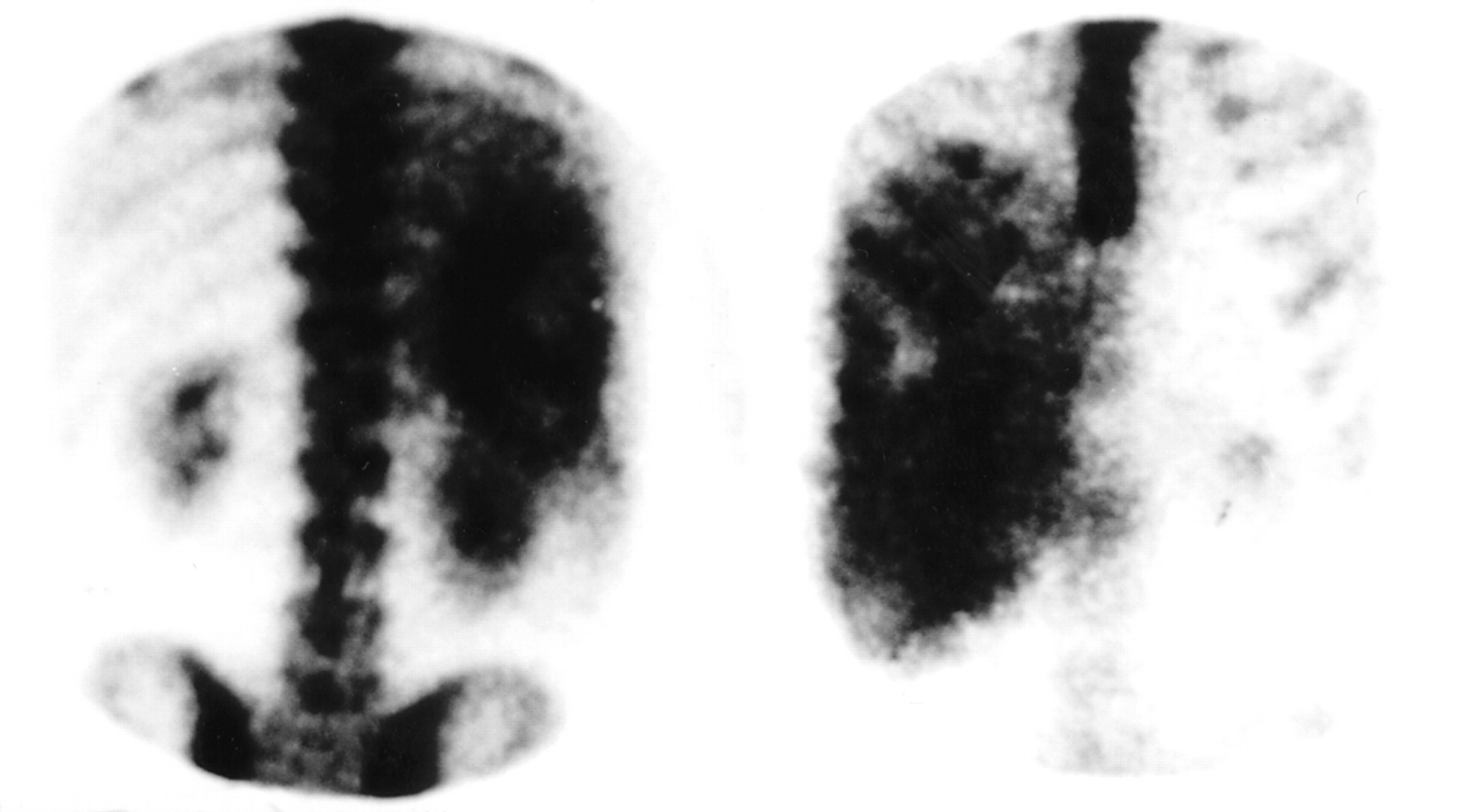
In other situations of soft-tissue visualization, the mechanism of uptake is less well defined although soft-tissue calcification is thought to play an important role (24). Because calcium deposition in the soft-tissue can be found in a variety of disease processes (such as ischemia, necrosis, metastatic calcification in renal failure, or hypercalcemia of any cause), it is conceivable to find uptake of the bone radiotracer in any organ in the body. However, this is an oversimplification; the uptake patterns occurring in individual organs usually point to a specific pathology. For example, cardiac uptake might be due to a recent myocardial infarction or to the presence of amyloid deposits (25). Pleural effusions may be delineated on the bone scan by diffuse increased uptake in a hemithorax. Such pleural uptake indicates a malignant effusion and is an ominous sign in patients scanned for skeletal metastases (26). The spleen may be seen on the bone scan of sickle cell patients (27), whereas uptake in the liver may indicate metastases from colon cancer (Fig. 4) (28). The renal parenchyma may show uptake on the bone scan because of hypercalcemia (29), posttransfusion changes (30), or irradiation (31).

Anterior (right) and posterior (left) abdominal views of 99mTc-MDP bone scan of patient with hepatic metastasis from colon carcinoma show intense uptake of radioactivity in liver, which is heavily involved with tumor.
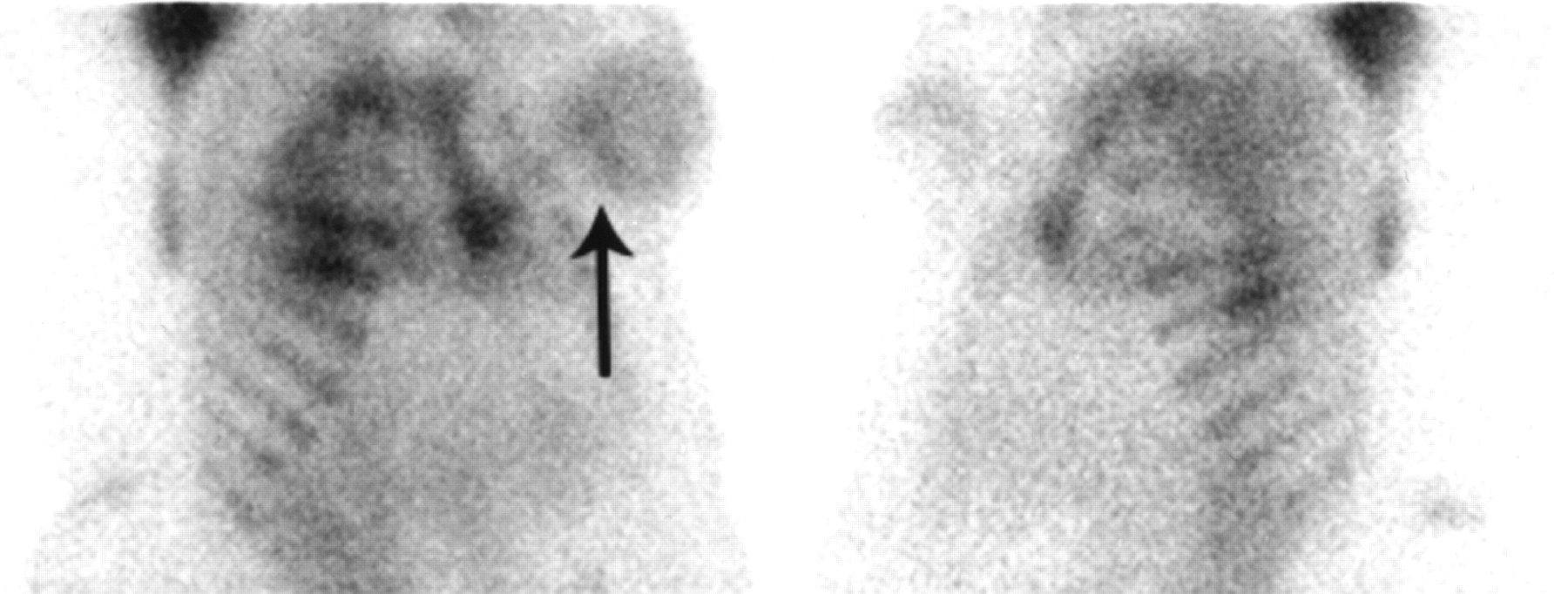
Finally, bone scanning has been advocated for evaluation of some soft-tissue tumors. For example, neuroblastoma and breast carcinoma are known to concentrate 99mTc-MDP (Fig. 5) (32). However, the clinical usefulness of 99mTc-MDP in this situation has not been established. A summary of clinically significant soft-tissue findings on bone scans is presented in Table 2. However, new artifacts and pitfalls in the form of unexpected soft-tissue uptake continue to occur in our clinical practice. Shown in Figure 6 is a recently encountered example of incidental soft-tissue uptake at a lower-back medication injection site that masqueraded as pathology on the bone scan.

Left anterior oblique (right) and right anterior oblique (left) views of chest from 99mTc-MDP bone scan of patient with left-breast cancer show soft-tissue uptake in both breasts. Uptake in left breast is more extensive (arrow) and corresponds to tumor mass on that side.

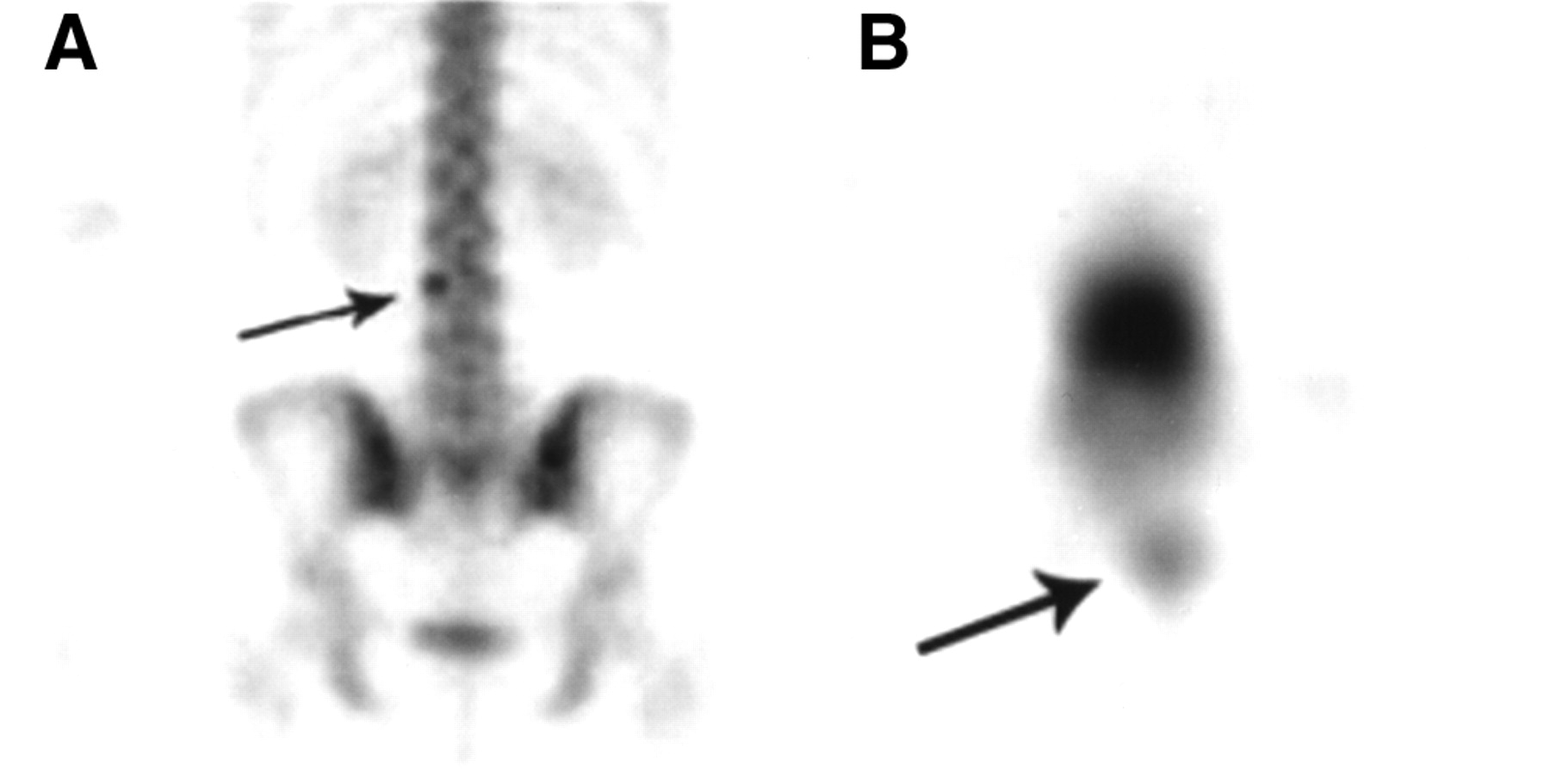
(A) Planar posterior image of lower back from 99mTc-MDP bone scan of patient with chronic back pain. Focus of increased uptake is seen in region of left pedicle of 3rd lumbar vertebra (arrow). (B) SPECT image shows this uptake to be more superficial in overlying soft tissue (arrow). Patient had received injections of antiinflammatory drugs at this site a few weeks before scan.
Soft-Tissue Uptake That Often Is Clinically Significant
CONCLUSION
Incidental nonosseous uptake on bone scans is occasionally seen. The uptake could be artifactual and due to a flaw in the procedure. Recognition of such occurrences helps to rectify the error and obtain the proper study. True nonosseous findings are related mainly to the urinary system. Most of the genitourinary abnormalities seen on the scan would be known from the clinical history or prior imaging investigations. Nevertheless, mention of such findings has become an integral part of the nuclear medicine report. Visualization of other organs can be expected and readily explained in certain conditions, such as splenic uptake in patients with sickle cell disease. However, in a few cases, incidental findings such as a previously unrecognized malignant pleural effusion in a patient with cancer can have an impact on patient management. The main purpose of the bone scan in most cases, however, remains to address abnormalities of the skeleton. This can be achieved only by using meticulous technique and appropriate assessment of the patient’s condition. In this context, obtaining a relevant medical history including a review of medications and other imaging studies will put the clinical problem in perspective and clarify incidental soft-tissue findings on the bone scan.
Footnotes
For correspondence or reprints contact: Issa Loutfi, MD, PhD, Department of Nuclear Medicine, Faculty of Medicine, Kuwait University, P.O. Box 24923, Safat 13110 Kuwait.
E-mail: loutfi{at}hsc.kuniv.edu.kw
*NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/education/ce_online.html) THROUGH SEPTEMBER 2004.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}