


Abstract
Our aim was to comparatively assess dual-tracer PET/CT (68Ga-DOTATATE and 18F-FDG) and multimodality anatomic imaging in studying metastatic neuroendocrine tumors (NETs) of unknown primary (CUP-NETs) scheduled for peptide receptor radionuclide therapy for divergence of tracer uptake on dual-tracer PET/CT, detection of primary, and overall lesion detection vis-a-vis tumor proliferation index (MIB-1/Ki-67). Methods: Fifty-one patients with CUP-NETs (25 men, 26 women; age, 22–74 y), histopathologically proven and thoroughly investigated with conventional imaging modalities (ultrasonography, CT/contrast-enhanced CT, MRI, and endoscopic ultrasound, wherever applicable), were retrospectively analyzed. Patients were primarily referred for deciding on feasibility of peptide receptor radionuclide therapy (except 2 patients), and all had undergone 68Ga-DOTATATE and 18F-FDG PET/CT as part of pretreatment workup. The sites of metastases included liver, lung/mediastinum, skeleton, abdominal nodes, and other soft-tissue sites. Patients were divided into 5 groups on the basis of MIB-1/Ki-67 index on a 5-point scale: group I (1%–5%) (n = 35), group II (6%–10%) (n = 8), group III (11%–15%) (n = 4), group IV (16%–20%) (n = 2), and group V (>20%) (n = 2). Semiquantitative analysis of tracer uptake was undertaken by SUVmax of metastatic lesions and the primary (when detected). The SUVmax values were studied over increasing MIB-1/Ki-67 index. The detection sensitivity of 68Ga-DOTATATE for primary and metastatic lesions was assessed and compared with other imaging modalities including 18F-FDG PET/CT. Results: Unknown primary was detected on 68Ga-DOTATATE in 31 of 51 patients, resulting in sensitivity of 60.78% whereas overall lesion detection sensitivity was 96.87%. The overall lesion detection sensitivities (individual groupwise from group I to group V) were 97.75%, 87.5%, 100%, 100%, and 66.67%, respectively. As MIB-1/Ki-67 index increased, 68Ga-DOTATATE uptake decreased in metastatic and primary lesions (mean SUVmax, 43.5 and 22.68 g/dL in group I to 22.54 and 16.83 g/dL in group V, respectively), whereas 18F-FDG uptake showed a gradual rise (mean SUVmax, 3.66 and 2.86 g/dL in group I to 7.53 and 9.58 g/dL in group V, respectively). There was a corresponding decrease in the 68Ga-DOTATATE–to–18F-FDG uptake ratio with increasing MIB-1/Ki-67 index (from 11.89 in group I to 2.99 in group V). Conclusion: In CUP-NETs, the pattern of uptake on dual-tracer PET (68Ga-DOTATATE and 18F-FDG) correlates well with tumor proliferation index with a few outliers; combined dual-tracer PET/CT with MIB-1/Ki-67 index would aid in better whole-body assessment of tumor biology in CUP-NETs.
Neuroendocrine tumors (NETs) have been classified into 3 grades by the European Neuroendocrine Tumor Society system based on the proliferative index (MIB-1/Ki-67 index) (1,2). G1 and G2 are well-differentiated NETs whereas G3 NETs are poorly differentiated. A dual-tracer PET imaging approach (with somatostatin receptor [SSTR]–based 68Ga-DOTATATE and glucose metabolism–targeted 18F-FDG PET/CT) is emerging as an important parameter for treatment planning and response evaluation in patients with NETs (3–7). Most of the well-differentiated NETs express high SSTRs on their cell surface, which are used for receptor-specific imaging by 68Ga-DOTATATE PET/CT. 18F-FDG PET/CT avidity, on the other hand, images the high-grade tumors and indicates aggressiveness of the disease, and increased 18F-FDG uptake has been associated with a poor prognosis (3–8). In a typical case scenario, the lower grade NETs should show SSTR expression (on 68Ga-DOTATATE PET/CT) more than the glucose transporter expression (on 18F-FDG PET/CT) and vice versa with poorly differentiated cases. In the clinical setting, however, frequent outliers occur, and therefore the dual-tracer imaging aids in a great way individualization of peptide receptor radionuclide therapy (PRRT) and also in deciding the combination of PRRT with other treatment modalities (such as chemotherapy and tyrosine kinase inhibitors) based on scan findings (7).
Metastatic NET of unknown primary (CUP-NET) constitutes around 20%–25% of all the cases of NET. In these patients, detecting the site of primary is an important step that would help in planning a more definitive and appropriate treatment to the patient. Identification and knowledge of the primary site are also of immense importance because other aspects of management are highly dependent on them, ranging from disease prognosis, treatment outcome, and survival rates. The role of 68Ga-DOTATATE (and of other 68Ga-DOTA-peptides) is universally recognized for the study of NET localization, and the procedure is now included in international guidelines for the detection of the unknown primary (among other indications) (8). Furthermore, several papers have been or are being published on the role of somatostatin analog for the characterization of the unknown primary in NET (detailed in the “Discussion” section): however, the performance of dual-tracer PET in patients of CUP-NET is relatively less explored methodically. Hence, the main aim of the present work was to analyze the dual-tracer imaging characteristics of this particular group of patients and also look at the performance of individual tracers vis-a-vis the MIB-1 index on histopathology.
MATERIALS AND METHODS
A retrospective evaluation was undertaken analyzing the cases of CUP-NET. The study protocol was approved by the Institutional Ethics Committee. The institutional review board (Medical Ethics Committee) approved this retrospective study, and the requirement to obtain informed consent was waived.
Most of the patients were referred to our center for PRRT (except for 2 patients, who were referred to search for the primary by 68Ga-DOTATATE PET/CT). 68Ga-DOTATATE and 18F-FDG PET/CT scans were available in all patients and evaluated as a part of the pretreatment workup protocol for PRRT, during which special emphasis was given to review all cases in which the primary was unknown. The cases selected for the study analysis fulfilled the following criteria: the patients had been diagnosed with CUP-NET; the cases were histopathologically proven to be NET by biopsy evaluation of the metastatic site, with availability of MIB-1–labeling index in the biopsy report; and there was evidence of extensive workup data provided by the conventional imaging modalities (including ultrasonography, triple-phase contrast enhanced [ceCT], MRI, endoscopic ultrasound [EUS]) as part of initial workup by the referring gastrointestinal oncologist that could not detect the site of primary.
A total population of 51 patients (25 men and 26 women; age range, 22–74 y) was included for the analysis. The sites of metastasis included the liver, lung, mediastinum, skeleton, abdominal and retroperitoneal nodes, pericardium, and other soft-tissue sites (detailed in Table 1). The patients were divided into groups of 5 based on the proliferative index (MIB-1/Ki-67 index) (Table 2). Among these, 12 of 51 patients had a suspected site of primary with evidence of metastasis from the prior workup imaging, and 68Ga-DOTATATE PET/CT was used for definite characterization of the suspected primary site. The final confirmation was established either by histopathology or by further correlative imaging.
Characteristics of Study Population
Division of Patients into Groups of 5 Based on MIB-1/Ki-67–Labeling Index and Depiction of Number in Each Category
Each patient was analyzed for the following parameters, both at the metastatic sites and at the primary site (if it could be located): measurement of the tracer uptake by semiquantitative SUVmax on 68Ga-DOTATATE and 18F-FDG PET/CT studies, correlation of the dual-tracer uptake with the biopsy-reported MIB-1/Ki-67–labeling index, number of cases in which 68Ga-DOTATATE or 18F-FDG PET/CT could detect the site of primary in which the conventional imaging modalities failed to conclusively diagnose, and total number of metastatic lesions in each patient detected by 68Ga-DOTATATE PET/CT in comparison with ultrasonography, CT/ceCT, MRI, and 18F-FDG PET/CT study.
RESULTS
The details of study population included and the patient subdivision according to MIB-1 index has been depicted in Tables 1 and 2, respectively. Separate patient-based and lesion-based analysis was undertaken.
Patient-Based Analysis: Performance of Dual-Tracer PET in Relation to MIB-1/Ki-67–Labeling Index
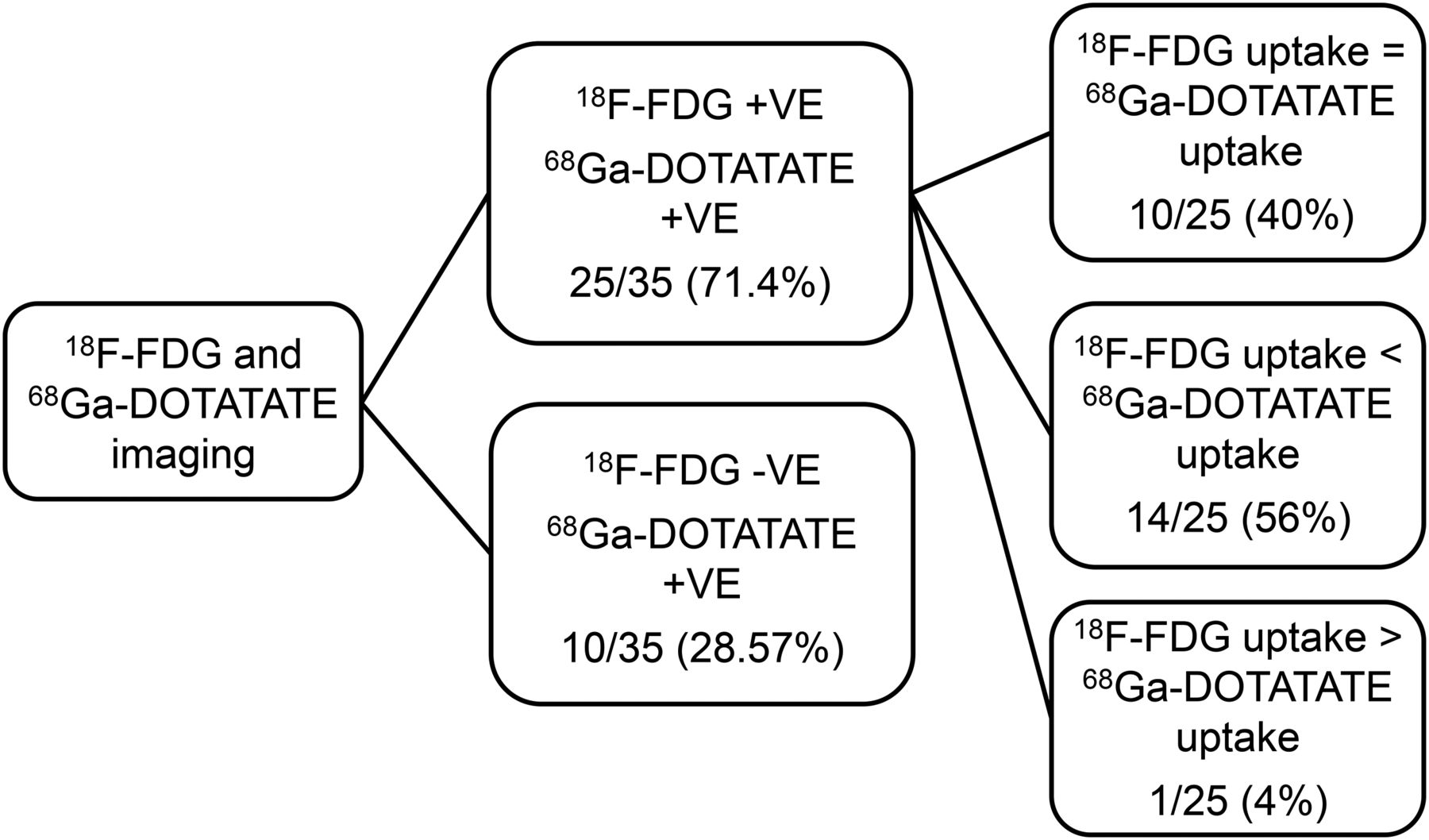
Group I (MIB-1/Ki-67 index of 1%–5%) consisted of 35 patients. Twenty-five of 35 (71.48%) patients showed scan positivity on both SSTR-targeted and glucose transporter–targeted imaging whereas 10 of 35 (28.57%) patients showed positivity only on SSTR-based imaging and had negative 18F-FDG PET/CT results (an expected finding in a low MIB-1 index case) (Figs. 1 and 2).

Flowchart demonstrating patient-specific analysis observed on 68Ga-DOTATATE and 18F-FDG PET/CT in group I patients (MIB-1 index, 1%–5%). +ve = positive; −ve = negative.
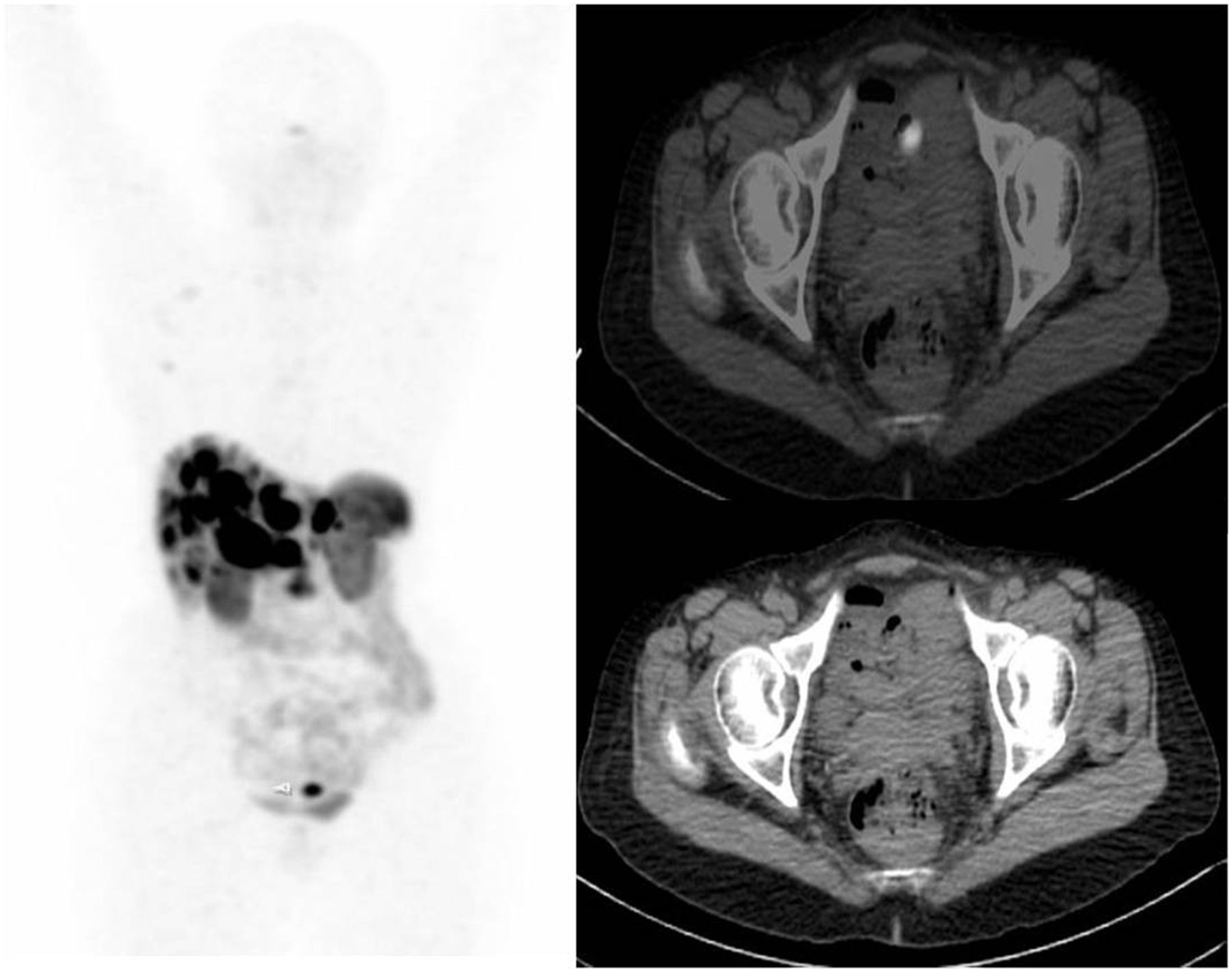
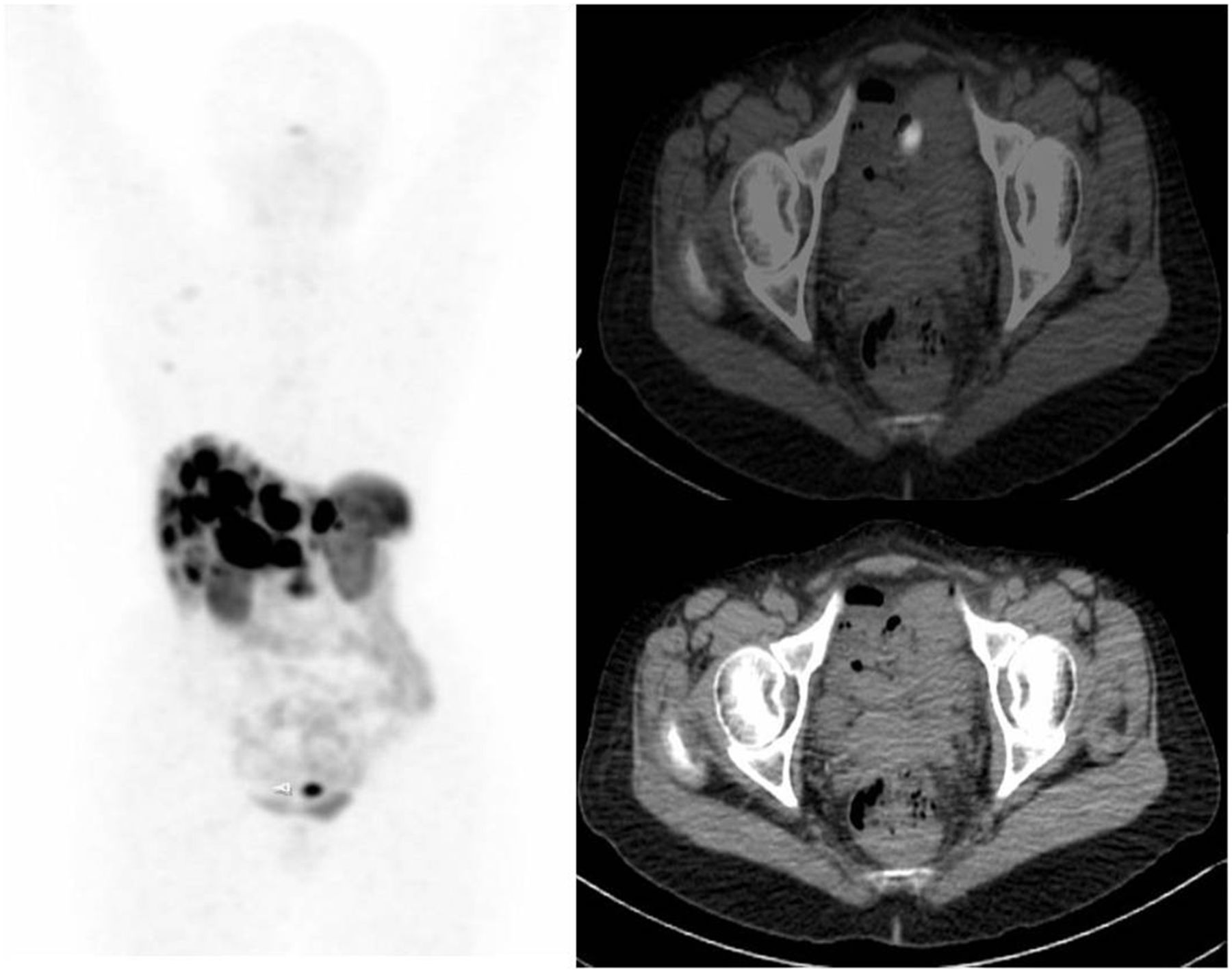
A 56-y-old woman with liver biopsy suggestive of metastatic NET of liver (MIB-1 index, <1%). Primary was undetected by conventional imaging. 68Ga-DOTATATE PET/CT scan showed multiple metastatic liver lesions and focal tracer concentration in the pelvic ileum. Final diagnosis was ileal NET with bilobar hepatic metastases. A color version of this figure is available as a supplemental file at http://tech.snmjournals.org.
Among the 25 patients positive on both 18F-FDG and 68Ga-DOTATATE PET/CT imaging, on visual assessment, uptake on SSTR-based PET was higher in 14 of 25, equal in 10 of 25, and less in 1 of 25 patients compared with the 18F-FDG PET uptake in the lesions.
On further subanalysis, in 10 of 14 cases showing predominant 68Ga-DOTATATE uptake, the MIB-1 index was found to be 2% or less (i.e., grade I NET), and in 4 of 14 cases it ranged from 3% to 5% (grade II NET). Both the aforementioned findings are commensurate with what can be expected of the performance 18F-FDG and 68Ga-DOTATATE in patients with low MIB-1–labeling index.
Group II (MIB-1/Ki-67 Index of 6%–10%)
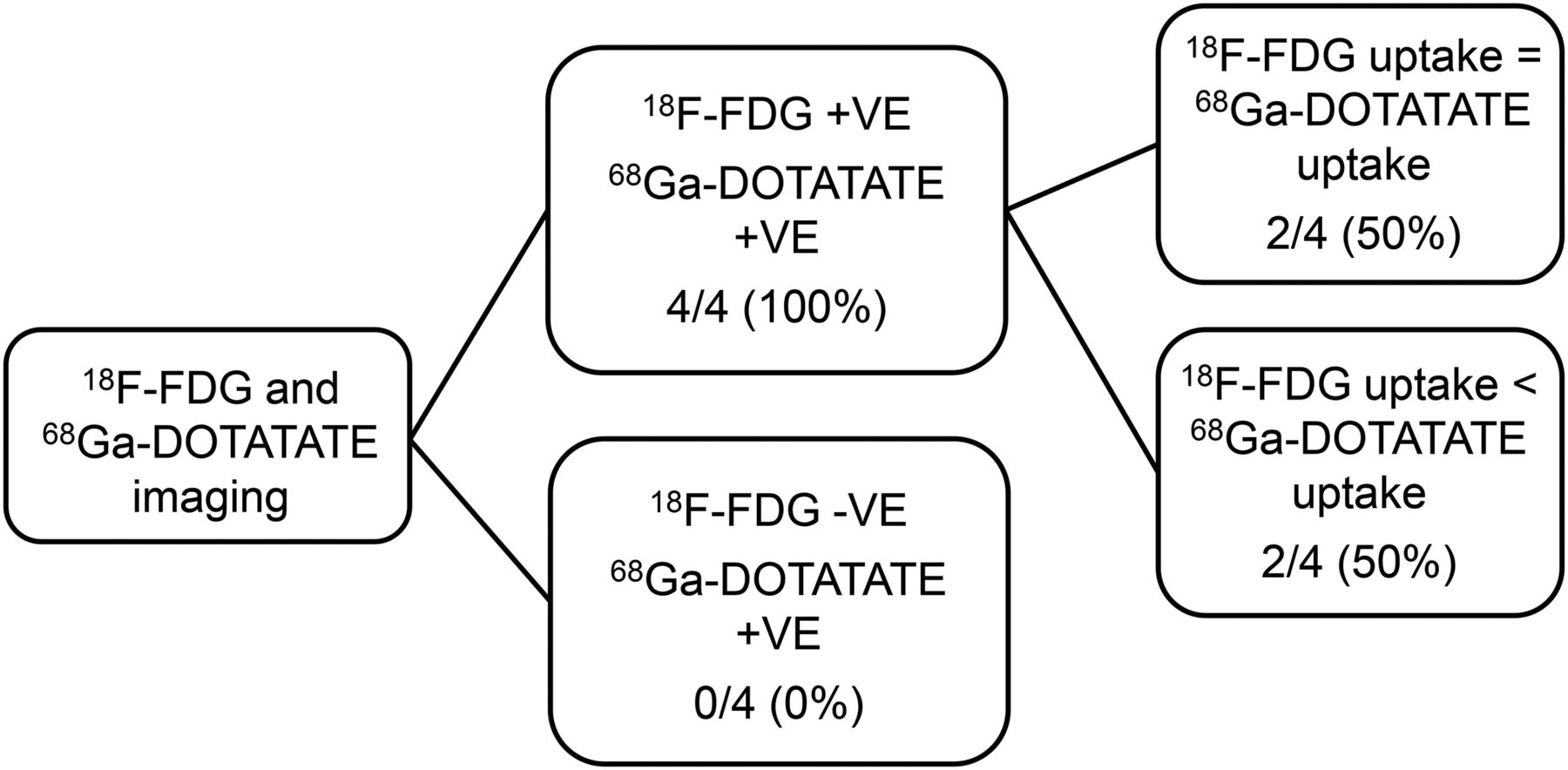
A total of 8 patients belonged to group II, among which 4 of 8 (50%) cases had negative 18F-FDG PET/CT findings, and 4 of 8 (50%) showed increased uptake by both tracers. All cases demonstrated high uptake on 68Ga-DOTATATE PET/CT scanning.
In 4 patients who had positive 18F-FDG PET/CT results, 2 of 4 showed 18F-FDG uptake equal to 68Ga-DOTATATE uptake, 1 of 4 showed predominant 18F-FDG uptake, and the remaining 1 patient showed 68Ga-DOTATATE uptake predominantly (Fig. 3).

Decision tree type ramification analysis to assess relative performance and uptake intensity in metastatic lesions by 68Ga-DOTATATE and 18F-FDG PET/CT in group II (MIB-1/Ki-67 index, 6%–10%). +ve = positive; −ve = negative.
Group III (MIB-1/Ki-67 index of 11%–15%) consisted of 4 patients, all of whom showed increased 18F-FDG as well as 68Ga-DOTATATE uptake (Fig. 4) on the dual-tracer PET (i.e., 100% concordance with regard to scan positivity). In 2 of these 4 patients, the 18F-FDG uptake was equal to SSTR-based imaging, and in the other 2 patients the uptake on 68Ga-DOTATATE was more than that with 18F-FDG PET.
Decision tree type ramification analysis to assess relative performance and uptake intensity in metastatic lesions by 68Ga-DOTATATE and 18F-FDG PET/CT in group III. +ve = positive; −ve = negative.
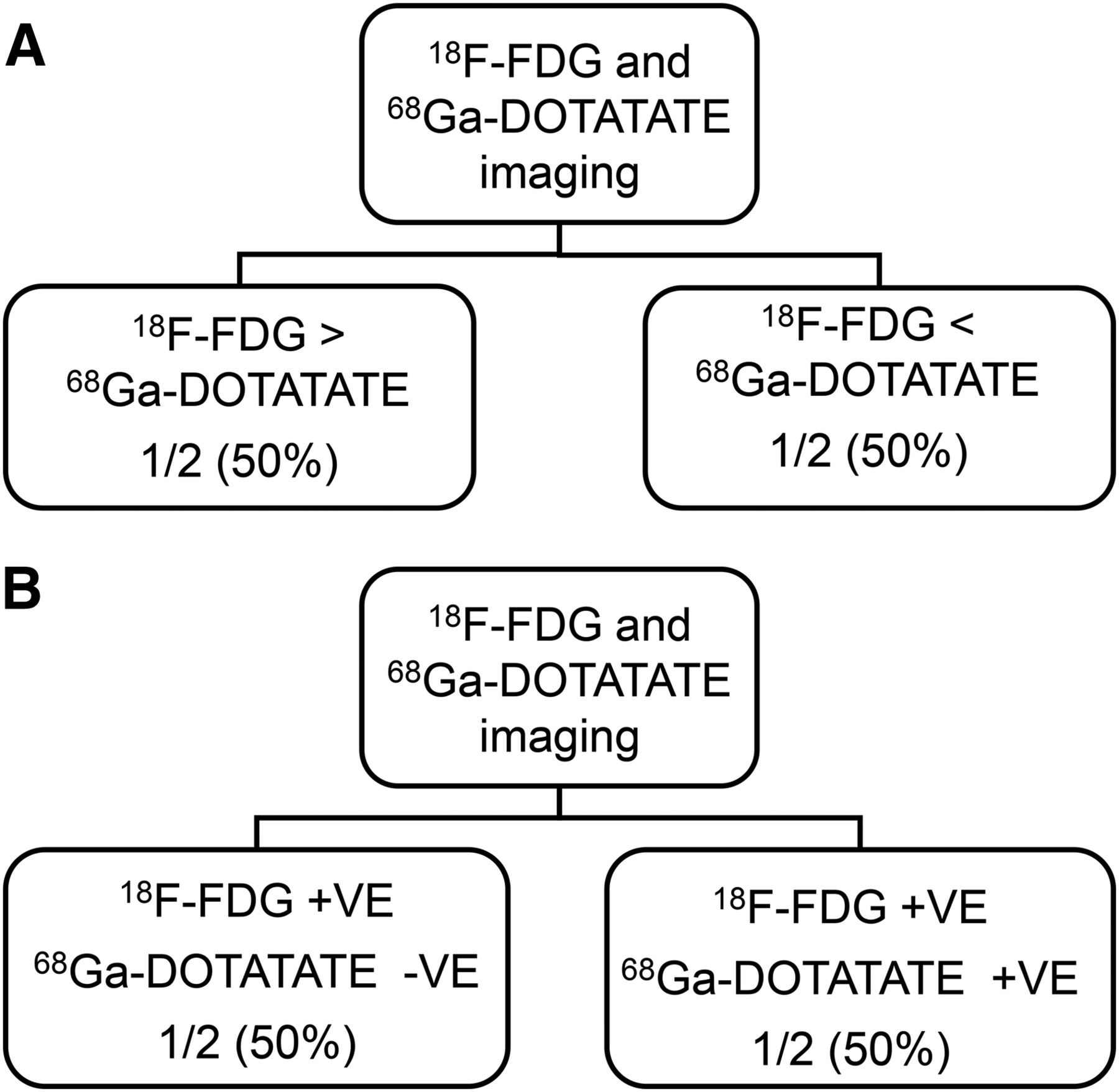
Group IV (MIB-1/Ki-67 index of 15%–20%) consisted of 2 patients. Both the patients showed 18F-FDG and 68Ga-DOTATATE uptake; one of the patients (50%) exhibited predominant 18F-FDG uptake whereas the other (50%) displayed predominant 68Ga-DOTATATE uptake (Fig. 5A).
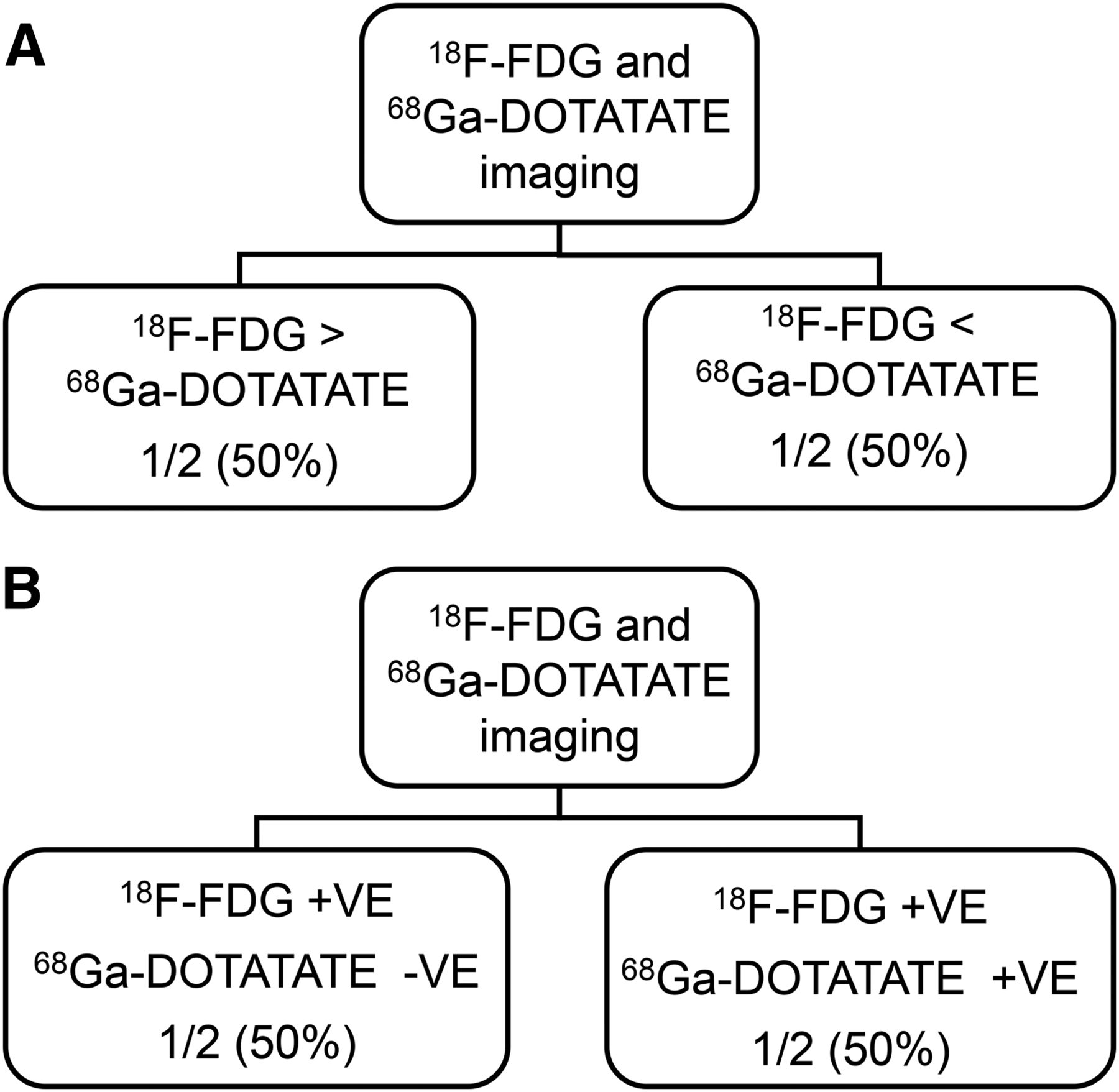
(A) Flowchart of assessment of relative positivity and uptake intensity in metastatic lesions by 68Ga-DOTATATE and 18F-FDG PET/CT in group IV. (B) Flowchart of assessment of relative positivity and uptake intensity in metastatic lesions by 68Ga-DOTATATE and 18F-FDG PET/CT in group V. +ve = positive; −ve = negative.
Group V (MIB-1/Ki-67 index of >20%) included 2 patients, one of whom (50%) showed no significant 68Ga-DOTATATE uptake but significant 18F-FDG uptake whereas the other (50%) showed both 18F-FDG and 68Ga-DOTATATE uptake, though the 68Ga-DOTATATE uptake was much more than 18F-FDG uptake (Fig. 5B).
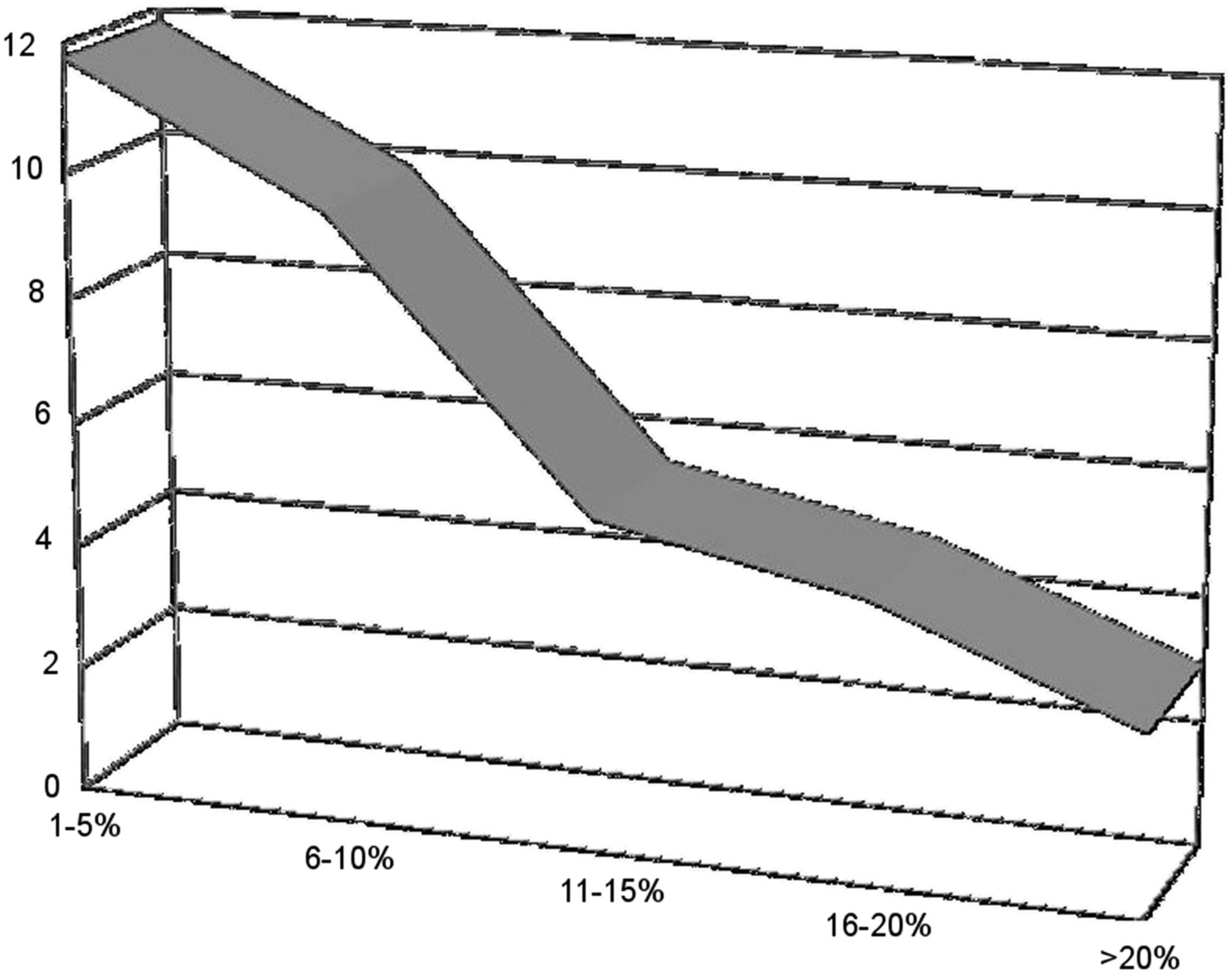
Thus, from the aforementioned data, we observed that 68Ga-DOTATATE uptake was typically predominant in the low–MIB-1/Ki-67 index tumors/well-differentiated NETs and 18F-FDG uptake predominated in the high–MIB-1/Ki-67 index tumors/poorly differentiated NETs. However, it was also noted that a low-grade 18F-FDG uptake can be observed in a fraction of low-grade NETs, and high-grade tumors (MIB-1 index > 20%) can also demonstrate significant 68Ga-DOTATATE uptake. When the SUVmax was calculated for either PET study, a decrease was noted in the uptake of 68Ga-DOTATATE as the MIB-1/Ki-67 index increased whereas 18F-FDG uptake demonstrated a gradual rise, resulting in a decrease in the 68Ga-DOTATATE–to–18F-FDG uptake ratio (Table 3). The decrease in uptake ratio with increasing proliferative index is an expected finding, signifying that lesional uptake of 68Ga-DOTATATE decreases and 18F-FDG increases with increasing proliferative activity of the tumor (Fig. 6).
Semiquantitative Analysis of Uptake Intensity (SUVmax) in Cases Demonstrating Uptake of Both Tracers in Metastases
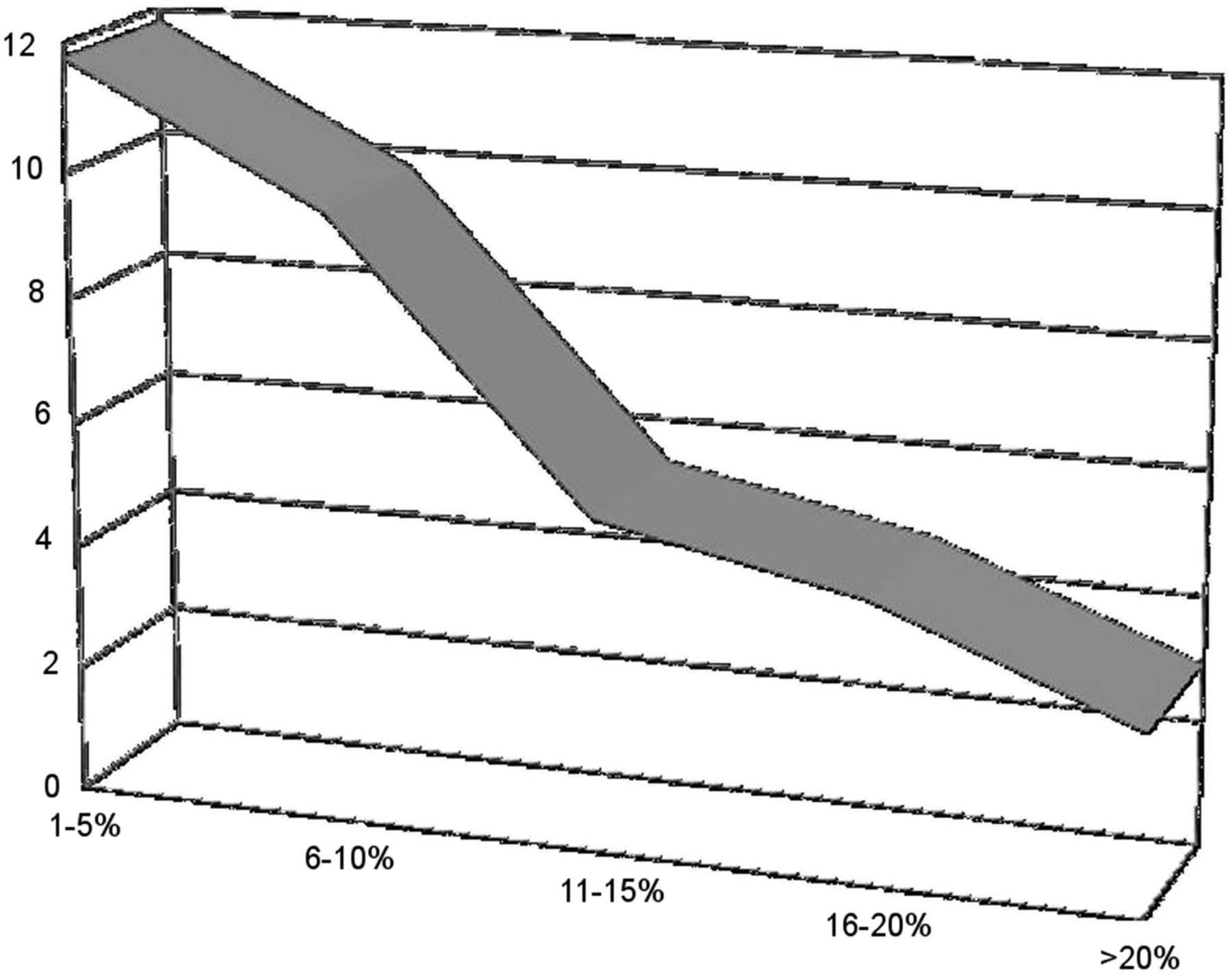
Graphical representation of variation in 68Ga-DOTATATE–to–18F-FDG uptake ratio in relation to increasing tumor proliferation (MIB-1) index.
Lesion-Based Analysis
Performance of 68Ga-DOTATATE in Detecting Site of Primary
Of a total of 51 patients who underwent thorough workup with conventional imaging modalities (ultrasonography, CT/ceCT, MRI, EUS) previously and yet the site of primary was not detected, 68Ga-DOTATATE could detect primary in 31 patients, resulting in an overall sensitivity of 60.78% in this group of patients. The most common site identified was gastroenteropancreatic NETs; others included lung and mesentery (Table 4).
Performance of 68Ga-DOTATATE in Detecting Primary in Patients of CUP-NET by Conventional Imaging Modalities
Comparative Performance of 68Ga-DOTATATE and 18F-FDG PET/CT in Detecting Primary in Relation to MIB-1–Labeling Index
The comparative sensitivity of dual-tracer PET imaging in detecting the primary was also studied in connection with MIB-1/Ki-67 index.
In group I, the primary could be detected in 23 of 35 cases (65.7%), of which only 4 primaries showed increased 18F-FDG uptake and all the primaries showed clearly enhanced 68Ga-DOTATATE uptake. In group II, among 8 patients, 3 (37.5%) sites of primary could be identified, of which none showed increased 18F-FDG uptake. However, all 3 patients displayed high uptake on SSTR-targeted imaging. In group III, 2 sites of primary could be detected among a total of 4 patients (detection sensitivity, 2/4 that is, 50%), of which both demonstrated increased 18F-FDG and 68Ga-DOTATATE uptake. In both group IV and group V, the site of primary could be found in only 1 of 2 patients (50%), who showed positivity on both PET/CT scans (Table 5).
Scan Positivity and Semiquantitative Analysis of Uptake intensity (SUVmax) in Cases Demonstrating Uptake of Both Tracers in Detected Sites of Primary: Comparison with MIB-1–Labeling Index Stratified Group
Groupwise Comparison of Overall Disease Staging: 68Ga-DOTATATE and 18F-FDG PET/CT Versus Conventional Anatomic Modalities
In all the groups, the sensitivity of the 68Ga-DOTATATE PET/CT scan was clearly superior to the standard imaging modalities such as ultrasonography, ceCT/CT, and even 18F-FDG PET/CT (96.87% vs. 42.96%, 57.81%, and 51.56%, respectively) (Table 6). 68Ga-DOTATATE is a potential investigation to be selected as the prime imaging modality for initial investigation and staging of the disease. It has been noted that 68Ga-DOTATATE and 18F-FDG PET/CT scans together complementarily can become a superlative staging modality, particularly in patients with relatively higher MIB-1–labeling index. Another noteworthy finding in this analysis was the increasing sensitivity of 18F-FDG PET/CT scanning with increasing proliferative index (MIB-1/Ki-67 index).
Comparison of All Imaging Modalities in Detecting Number of Lesions and Calculation of Their Sensitivity
The following are imaging characteristics of dual-tracer PET/CT imaging in correlation with MIB-1/Ki-67 index. In low MIB-1/Ki-67 index (especially ≤ 2%), 68Ga-DOTATATE uptake predominated even though low-grade 18F-FDG uptake can be seen in several cases; this is consistent with features of well-differentiated NET. As the MIB-1/Ki-67 index rises (>3%–15%), the 18F-FDG uptake shows a progressive rise both in primary and in metastatic lesions. Significant 68Ga-DOTATATE uptake in the tumor persists despite the intermediate proliferative index. In high MIB-1/Ki-67 index (>15%), 18F-FDG uptake progressively increases and predominates in an increasing percentage of patients. However, a low-grade 68Ga-DOTATATE uptake can be seen given the type of tumor. The 68Ga-DOTATATE–to–18F-FDG uptake ratio showed a decreasing trend with increasing tumor proliferation (MIB-1) index (Fig. 6). 68Ga-DOTATATE PET/CT has a potential role to become the sole investigation for staging of the disease in a patient with NET (particularly up to an MIB-1 index of 20%, with superior overall lesion detection sensitivity [96.87%]). Moreover, it should become the first investigation in a workup of a patient with CUP-NET because it can detect a substantial fraction of patients who were designated CUP-NET after extensive investigation with conventional anatomic imaging modalities. The sensitivity of 18F-FDG PET/CT for staging the disease rises with the increasing proliferative activity in the tumor signified by MIB-1/Ki-67 index. 18F-FDG uptake progressively increases with increasing tumor grade and should be used for disease prognostication. The overall detection sensitivity of 68Ga-DOTATATE PET/CT in detecting the site of primary in cases of CUP-NET, in which the conventional imaging modalities could not identify the primary, was 60.78%. One area where it can have a potential role is confirming through characterizing a suspected site and clearly depicting the primary when it was missed by conventional ceCT (Fig. 7).

(A) A 56-y-old woman, diagnosed as having metastatic NET. ceCT showed multiple hypodense liver lesions, abdominal nodes, multiple skeletal lesions, pararectal node, and right adnexal mass. Irregular wall thickening was seen in rectum, but was missed due to relative nonenhancement of lesion. In view of histopathology, patient was referred to us for 68Ga-DOTATATE scanning. (B) 68Ga-DOTATATE showed increased uptake in rectal wall, left adnexal mass, pararectal node, and multiple liver and skeletal lesions, thus confirming that this was a case of metastatic NET with rectal primary. A color version of this figure is available as a supplemental file at http://tech.snmjournals.org. (C) Corresponding images of MRI pelvis: confirming right adnexal mass and rectal primary.
DISCUSSION
There is a rapid expansion and increasing application of functional SSTR-targeted imaging with 68Ga-DOTA labeled somatostatin analogs and therapy (PRRT) with 177Lu-DOTATATE in the clinical management of metastatic and inoperable NETs (9–14). 68Ga-DOTATATE PET/CT has proven to be a pertinent tool in management of NETs, its utility extending right from diagnosis until prognostication of the disease (9–12). Another important role that 68Ga-DOTATATE PET/CT can play is the detection of the primary tumor site in patients of CUP-NETs, an essential step toward patient management (15–20).
One of the salient decision-making factors for choosing the appropriate therapy in metastatic NETs has been the tumor grade, which is based on the proliferation index (also known as MIB-1/Ki-67–labeling index) (21–24). The European Neuroendocrine Tumor Society system grades the NETs based on the proliferative index (MIB-1/Ki-67–labeling index) into G1 (well differentiated), G2 (moderately differentiated), and G3 (poorly differentiated) NETs (1). A flip-flop phenomenon is usually seen in which 68Ga-DOTATATE PET/CT and 18F-FDG PET/CT findings are inversely related at either end of the European Neuroendocrine Tumor Society system spectrum (3–8). G2 tumors, representing the middle of the spectrum, can demonstrate uptake of both 68Ga-DOTATATE and 18F-FDG (3–8,18). 68Ga-DOTATATE PET/CT as a relatively superior disease-characterizing and -localizing modality that plays an important role during planning of treatment for NET and furthermore, combined with 18F-FDG PET/CT, constitutes a major prognostication tool in management. Functional imaging with both 68Ga-DOTATATE and 18F-FDG has potential for a more comprehensive tumor assessment in both intermediate– and high–MIB-1 index tumors (3–8).
68Ga-DOTATATE PET/CT has proven to be superior to conventional imaging modalities in detecting the primary in patients with CUP-NET (15–20). All the cases of CUP-NET are usually initially worked up with conventional imaging modalities such as ultrasonography, CT/ceCT, MRI, and EUS where applicable, which are unsuccessful in identifying the site of origin. In this study, we have strictly included those cases of histopathologically proven metastatic CUP-NETs, which have been thoroughly worked up with conventional imaging modalities, by which the site of primary could not be detected. As a tertiary care center with a busy clinical PRRT service, we primarily got cases that were referred for PRRT. This might have introduced some bias in the cases that were retrospectively included because all of them had high uptake on 68Ga-DOTATATE (which could also explain why our study had high grade 1 tumors); however, to our advantage was the availability of complete imaging and histopathologic (MIB-1 index) workup data in each patient included in the analysis. This availability of data made it possible to create a unique study design to examine the performance of dual-tracer PET in patients of CUP-NET vis-a-vis the MIB-1/Ki-67–labeling index for detection of not only the primary but also the other characteristics such as the dual-tracer uptake intensity and pattern and overall lesion detection sensitivity across the varying MIB-1–labeling indices. Dual-tracer PET/CT with quantification was undertaken along with the conventional anatomic imaging modalities.
The sensitivity of 68Ga-DOTATATE PET/CT in detecting primary was highest in G1, well-differentiated NETs (65.7%), and decreased as the proliferative index increased (37%–50% in G2 and G3 NETs). We had extended the objectives of this study to scrutinize how the overall lesion detection sensitivity of each of the functional imaging (68Ga-DOTATATE PET/CT and 18F-FDG PET/CT) modalities can differ from that of the proliferative activity and whether they have a complementary role. 68Ga-DOTATATE PET/CT demonstrated higher sensitivity than conventional modalities and 18F-FDG PET/CT scans. As could be theoretically expected, we observed that the sensitivity of 18F-FDG PET/CT increased with intermediate- and high-grade NETs. Also the number of lesions detected was greater when 68Ga-DOTATATE and 18F-FDG PET/CT scan findings were combined, arguing for the adoption of this approach in clinical routine while evaluating NETs.
The concept of dual-tracer imaging with SSTR scanning with 68Ga-DOTATATE and 18F-FDG PET/CT (signifying glycolytic metabolism) is forthcoming in the management of NETs and is being continued to be explored. The number of patients has been divided into 5 groups based on MIB-1/Ki-67–labeling index within a range of 5% between each successive group so that the variability in the tumor behavior can be studied with dual-tracer PET imaging within a narrow width of proliferation. Most of the cases were concordant with the typical flip-flop pattern of dual-tracer uptake with highest 68Ga-DOTATATE uptake in low-grade tumors and highest 18F-FDG uptake in the high-grade tumors. Atypical partial concordance was also observed with regard to uptake of both 68Ga-DOTATATE and 18F-FDG in a few cases; this signified different tumor biology in metastatic and primary lesions as well as different sites of metastasis. The finding of an atypical uptake pattern suggests that in such cases histopathologic diagnosis alone would not suffice. Interestingly, the recent literature on NETs have reported behavioral and treatment response heterogeneity among the same-grade tumors (21–24), which, at least in part, could be explained by our finding of an atypical uptake pattern in dual-tracer PET imaging. Our finding would warrant an amalgamation of histopathology and dual-tracer PET imaging for improving diagnosis, therapy selection, and prognostication, which in turn has the potential to better the overall outcome of disease.
The sensitivity of 68Ga-DOTATATE PET/CT in detecting the site of primary in cases of CUP-NET as observed in our study (60.78%) conforms well not only with the current facts, but also with the high sensitivity of overall lesion detection ability in low- and intermediate-grade tumors (in our study up to group IV), making it a preferred modality compared with the others.
Although the limitation of this study has been a small population in each subgroup (especially groups III, IV, and V), on a broader perspective, this was a unique group of patients with CUP-NETs that were specifically examined in a PRRT workup setting; even in this specific population group there was an overall trend noted between MIB-1 index and PET index (68Ga-DOTATATE–to–18F-FDG uptake ratio) as demonstrated by the results.
CONCLUSION
68Ga-DOTATATE PET/CT is an important imaging modality for the detection of site of unknown primary in CUP-NETs and also for overall lesion detection of the disease. It scores over the conventional imaging modalities and also 18F-FDG PET/CT in staging of the disease. However, a better assessment and sensitivity for staging can be acquired by combining 68Ga-DOTATATE and 18F-FDG PET/CT scans. An amalgamation of dual-tracer uptake imaging with 68Ga-DOTATATE and 18F-FDG PET/CT should be done with histopathologic diagnosis of disease to study the divergent tumor biology for better management and outcome in patients with NETs.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Feb. 2, 2017.
REFERENCES
- Received for publication October 20, 2016.
- Accepted for publication November 30, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}