


Abstract
Epilepsy is one of the most common yet diverse neurologic disorders, affecting almost 1%–2% of the population. Presently, radionuclide imaging such as PET and SPECT is not used in the primary diagnosis or evaluation of recent-onset epilepsy. However, it can play a unique and important role in certain specific situations, such as in noninvasive presurgical localization of epileptogenic brain regions in intractable-seizure patients being considered for epilepsy surgery. Radionuclide imaging can be particularly useful if MR imaging is either negative for lesions or shows several lesions of which only 1 or 2 are suspected to be epileptogenic and if electroencephalogram changes are equivocal or discordant with the structural imaging. Similarly, PET and SPECT can also be useful for evaluating the functional integrity of the rest of the brain and may provide useful information on the possible pathogenesis of the neurocognitive and behavioral abnormalities frequently observed in these patients.
Presently, nuclear medicine imaging such as PET and SPECT is not used in the primary diagnosis or evaluation of recent-onset epilepsy. However, it can play a unique and important role in certain specific situations. Almost a fourth of epileptic patients do not respond to medical treatment and develop intractable seizures. PET and SPECT can play a significant role in such patients by its ability to noninvasively localize epileptogenic brain regions before surgery. PET and SPECT do not play much of a role in localization when structural lesions visible on MR imaging are concordant with electrophysiologic and clinical data. However, many patients may have no visible brain lesion on CT or MR imaging, particularly children less than 2 y old, in whom some cortical malformations may be poorly visualized or missed completely because of immature myelination and poor gray matter–white matter differentiation. This limitation is significant, considering that these abnormalities constitute a major cause of epilepsy in children. Similarly, patients may have multiple structural lesions of which only 1 or 2 are epileptogenic, may have seizures arising far from the lesion, or may have discordant or inconclusive electroencephalogram findings. PET and SPECT can be useful in such cases by identifying the epileptogenic regions and guiding the subsequent subdural-electrode placement and surgical resection. Sometimes the epileptogenic lesion may be medial and associated with generalized epileptiform activity rather than focal discharges on the electroencephalogram due to secondary bilateral synchrony. In such cases, PET or SPECT may allow for a surgical option in a patient who might otherwise not even be considered for surgery. In this review, we will discuss some important roles played by PET and SPECT in the presurgical evaluation of intractable seizures: for localizing epileptogenic regions, particularly when structural imaging results are normal, when there is discordance between structural and electrophysiologic data, and when multiple lesions are shown by other modalities; for identifying dual pathology; for assessing the presence of potential secondary epileptic foci; and for evaluating the functional integrity of the rest of the brain.
RADIOTRACERS AND TECHNICAL CONSIDERATIONS
Table 1 summarizes the PET and SPECT radiotracers used to evaluate epilepsy.
Targeted Pathways, Used Radiotracers, and Their Usual Uptake Pattern in Epileptogenic Region
PET Imaging
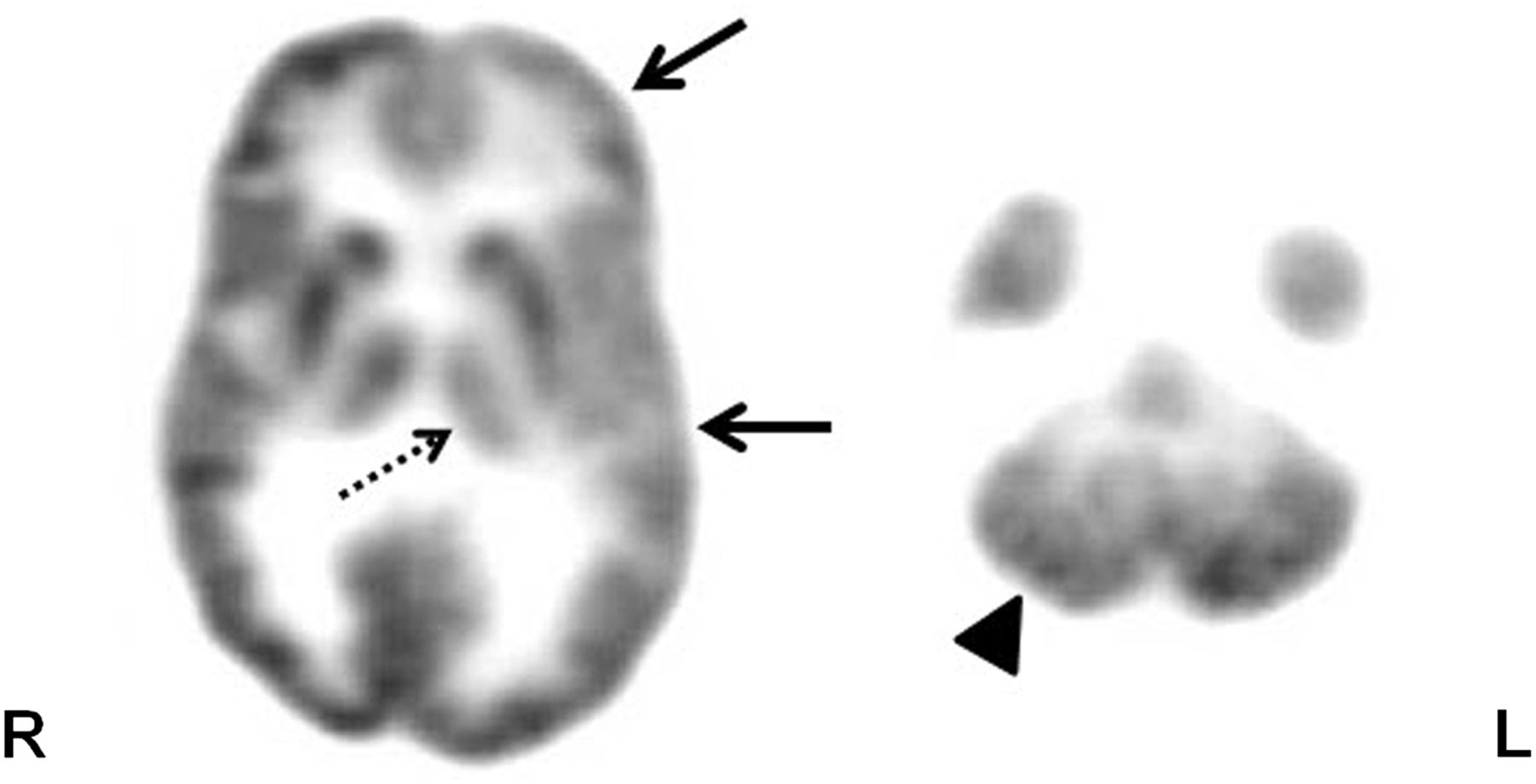
The most commonly used PET tracer in epilepsy is 18F-FDG, which measures glucose metabolism related to the synaptic and neuronal activity of the brain tissue (1). Interictal 18F-FDG PET typically shows reduced radiotracer uptake (hypometabolism) in the epileptogenic region (Fig. 1). This hypometabolism can result from a variety of mechanisms, including neuronal loss, diaschisis, or reduction in synaptic density. It appears that cortical hypometabolism may be associated with the duration, frequency, and severity of the seizures, as hypometabolism is usually found in only 25% of children with new-onset epilepsy, compared with 80%–85% of adults with intractable seizures (2). Persistent or increased seizure frequency may lead to enlargement of the hypometabolic area, whereas reduced seizure frequency may be associated with a decrease in the size of the hypometabolic cortex or even resolution of the hypometabolism (3). Hypometabolism of the ipsilateral thalamus can be seen in cases of focal epilepsy (mostly in the frontal and temporal cortex, medial temporal lobe epilepsy being particularly associated with dorsal thalamus hypometabolism; Fig. 1). Contralateral cerebellar hypometabolism (diaschisis) can be seen in cases of frontal (mainly) or parietal lobe seizures (Fig. 1). Occasionally, hypometabolism is seen in a contralateral mirror region and represents functional suppression of these regions through callosal fibers (transcallosal diaschisis) or through the fornix if the hippocampus is contralateral. Longstanding uncontrolled seizures may show extensive areas of hypometabolism, likely involving seizure propagation pathways or indicating the effect of the seizures on connected brain regions. Another factor that can affect the rate of glucose metabolism in the brain is the use of antiepileptic drugs. The absolute rates of glucose metabolism can be decreased by these drugs (such as barbiturates, valproate, phenytoin, or carbamazepine; the decrease is greatest with barbiturates and less with the 3 other drugs, in the order listed) (4).
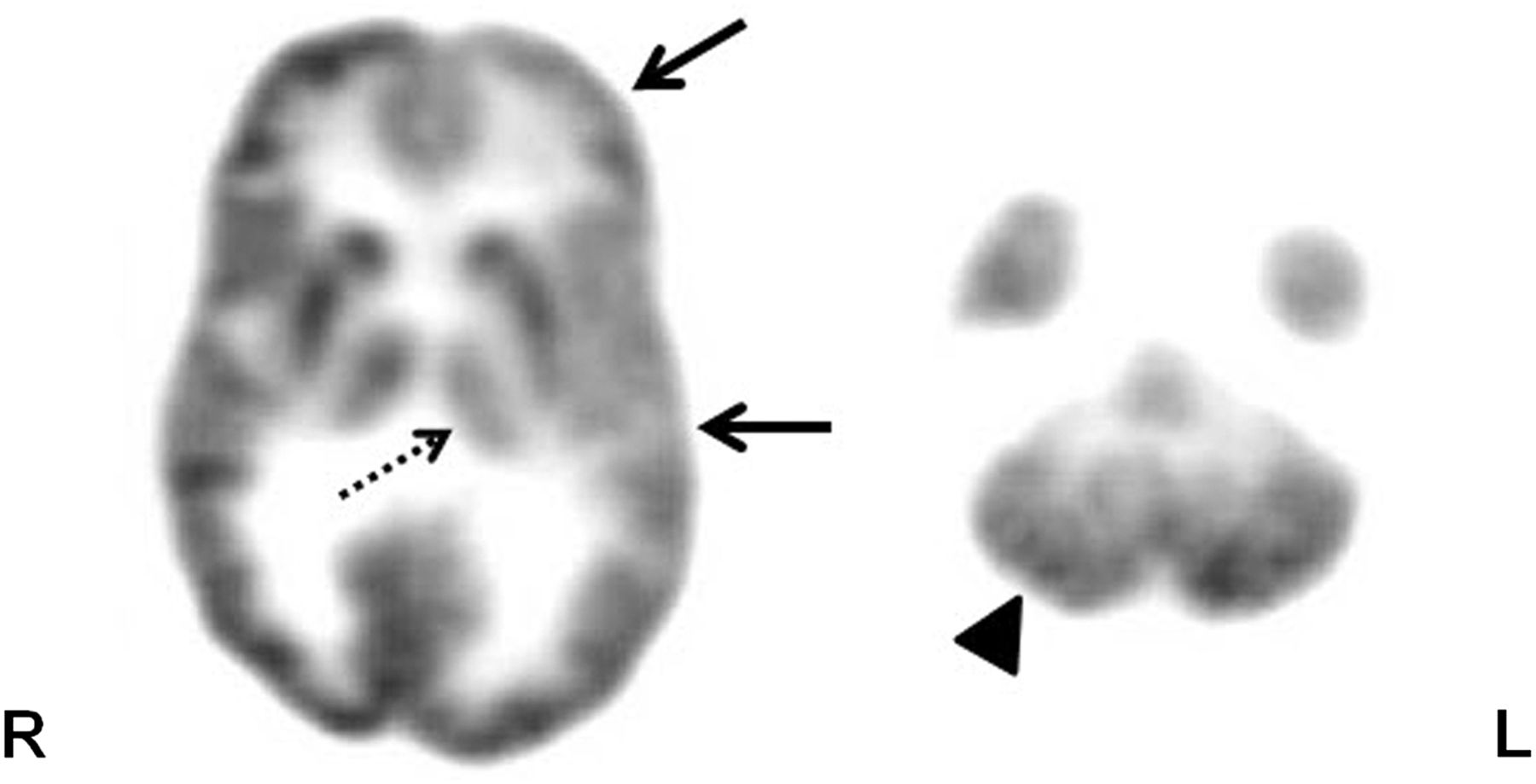
Axial 18F-FDG PET scan in patient with intractable epilepsy, showing hypometabolism in left frontotemporal cortex (solid arrows). Also seen is hypometabolism in ipsilateral thalamus (broken arrow) and contralateral cerebellum (arrowhead), likely representing thalamic and cerebellar diaschisis, respectively.
Because 18F-FDG PET usually shows a large area of hypometabolism extending beyond the epileptogenic region, this modality cannot reliably be used to precisely determine the surgical margin. However, it can be used for lateralization and general localization of the seizure focus. This information can help in making an a priori hypothesis about subsequent subdural electrode placement—information that may be useful, particularly when the results of MR imaging are normal. At the same time, 18F-FDG PET can be useful for evaluating the functional status of the rest of the brain when an epileptogenic lesion is considered for surgical resection, as postsurgical neurocognitive outcome will also depend on the integrity of the remaining (unresected) cortex. Such an evaluation is particularly important in children, because brain plasticity after resection is likely to involve functionally intact regions.
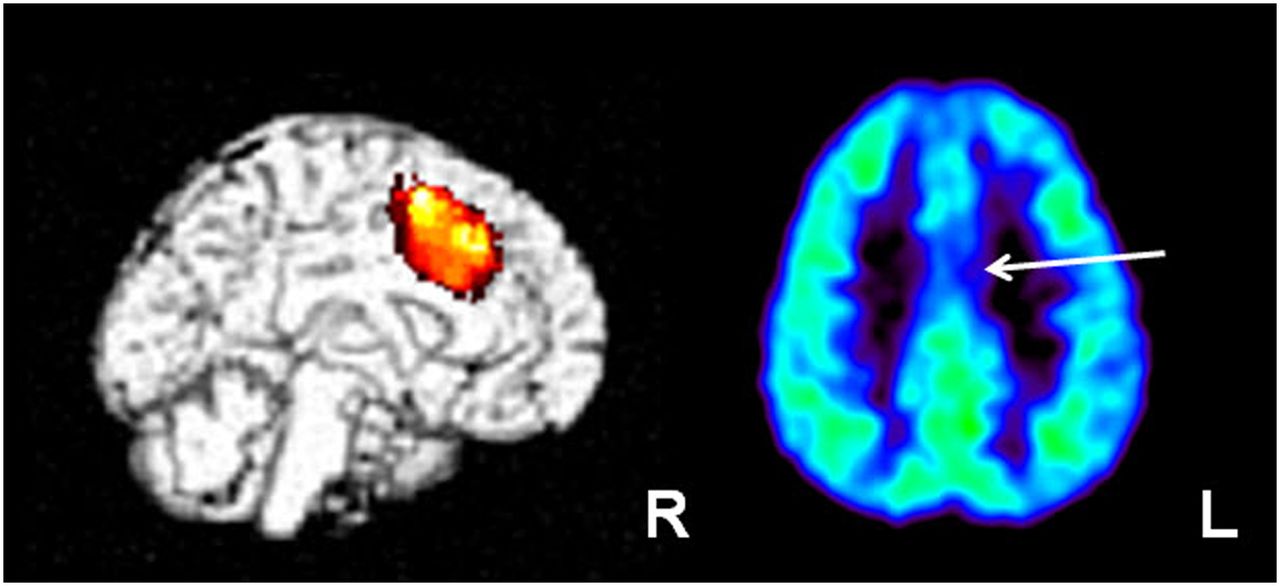
For clinical 18F-FDG images, visual inspection is the standard method of interpretation, with the interpreter comparing any hemispheric asymmetry with a normal 18F-FDG brain pattern. The analysis can be further refined by calculating the asymmetry index and comparing it with a preselected threshold value of asymmetry (usually ∼10%) to aid surgical resection of epileptic foci (5). Various other methods of PET data analysis, such as statistical parametric mapping (SPM, a voxel-based whole-brain analysis) or SPM extent analysis with asymmetry index, can also be used and can either increase the diagnostic yield of the PET scan or be helpful in equivocal cases (Fig. 2) (6–8).

SPM analysis of 18F-FDG PET scan in child with intractable epilepsy, normal findings on MR imaging, and generalized electroencephalogram changes. Initial reading showed normal findings on 18F-FDG PET; however, SPM analysis revealed area of hypometabolism in left medial frontal/cingulate cortex (left image), which appeared to be suggestive/hypometabolic in rereview of 18F-FDG PET scan (arrow; right image). Child underwent 2-stage epilepsy surgery with intracranial subdural interhemispheric electrode placement, which showed ictal discharges from this region. These medial discharges perhaps resulted in generalized (nonlateralized) electroencephalogram changes. Area was resected and child is seizure-free after surgery.
Another PET tracer with the potential for detecting epileptic brain regions is 11C-flumazenil, which binds to α subunits of the γ-aminobutyric acid A benzodiazepine receptor. 11C-flumazenil binding in the medial temporal lobe is robust enough for its good visualization (compared with 18F-FDG PET, with which the medial temporal region, particularly the hippocampus, is often not well visualized). This characteristic of 11C-flumazenil PET is a main reason that it is preferred over 18F-FDG PET for use in medial temporal lobe epilepsy, with the former showing focally decreased tracer binding in the hippocampus, compared with the larger area of hypometabolism also involving the temporal neocortex shown by the latter (Fig. 3). Also evaluated in epilepsy have been various other radioligands that bind to translocator protein (previously known as peripheral benzodiazepine receptors and expressed on activated microglia in cases of neuroinflammation), opioid receptors, histamine receptors, N-methyl-d-aspartate (NMDA) receptors, serotonin receptors, and acetylcholine receptors. Among these radioligands, 11C-α-methyl-l-tryptophan, which does not bind to a receptor but measures tryptophan metabolism, appears to be a promising candidate. Interestingly, PET performed with this radioligand can show increased uptake in the epileptogenic cortex interictally, making visual detection easier than with those tracers whose uptake or binding is usually reduced in the interictal phase (9).
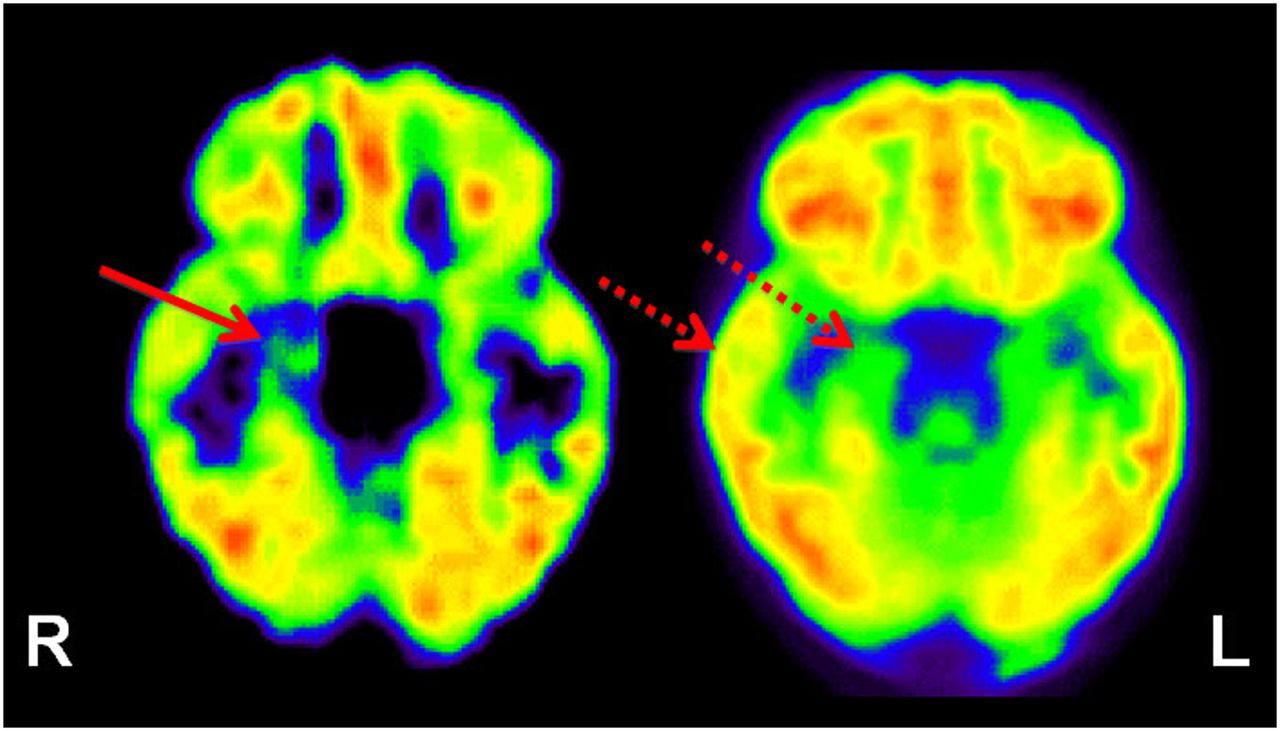
11C-flumazenil PET (left image) showing focal abnormality (decreased tracer binding) involving right hippocampus (solid arrow) in patient with medial temporal lobe epilepsy. In comparison, 18F-FDG PET (right image) shows widespread 18F-FDG hypometabolism in right temporal lobe, including neocortex (broken arrows).
SPECT Imaging
In epilepsy, SPECT imaging is used mostly to provide information about cerebral perfusion, alteration of which is considered to depend on the electrical status of the brain. The most common radiotracers used for this purpose are hexamethylpropyleneamine oxime and ethyl cysteinate dimer labeled with 99mTc. During a seizure, the cerebral blood flow changes rapidly over time, depending on the type of seizure and its mode of propagation. Therefore, early injection of the radiotracer during the seizure is imperative to capture blood flow changes in the epileptic zone. Similarly, knowledge of the exact time of injection and duration of the seizure is important for correct interpretation of the SPECT images. Delayed injection of radiotracer may show a variable pattern of blood flow changes in the epileptic zone as the seizure evolves, as well as a variation in the mode and pattern of seizure propagation.
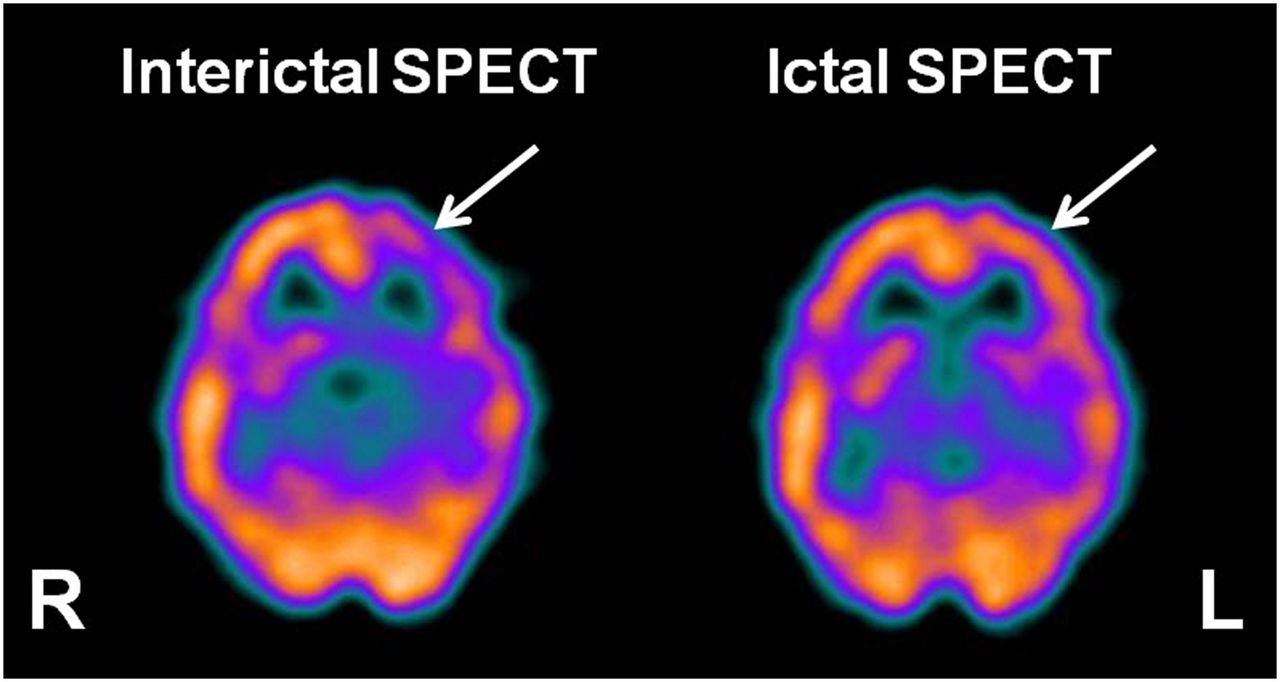
During the ictal phase, blood flow in the epileptic region can increase by up to 300% and can be seen as an area of hyperperfusion on ictal SPECT (Fig. 4) (10). True ictal SPECT (tracer injected immediately after the onset of the seizure and SPECT images showing perfusion at that time) shows an area of hyperperfusion in the epileptogenic region, surrounded by an area of hypoperfusion that becomes more prominent at the end of the ictal phase. This surrounding area of hypoperfusion may be caused by the steal syndrome (shifting of blood flow to the seizure focus) or may reflect an inhibitory zone trying to limit the seizure spread (11). Interictal SPECT (tracer injected when the patient is not having any clinical or subclinical seizure and SPECT images showing the baseline perfusion pattern) shows hypoperfusion or normal perfusion in the epileptogenic region (Fig. 4). Even when present, hypoperfusion may be mild and sometimes difficult to distinguish from the surrounding normal brain on visual examination. The main role of interictal SPECT at present is to assist in the evaluation of ictal SPECT, visually or quantitatively, using SPM or SISCOM (subtraction ictal SPECT coregistered to MR imaging; that is, the interictal SPECT images are subtracted from the ictal images and the results are displayed on coregistered MR images), by providing a baseline blood flow. Use of these registration techniques can increase the sensitivity and specificity of ictal SPECT (12,13). The probability of localizing an ictal onset zone has been found to be higher with SISCOM than with ictal electroencephalography and MR imaging (14). Use of SISCOM can help in revisiting and detecting subtle changes on MR images that were initially reported as showing normal findings (15). Studies have shown that the area of the resected SISCOM abnormality is associated with surgical outcome; the larger the area of the resected SISCOM abnormality, the better the outcome (14,16). However, the use of SPECT or SISCOM in children can sometimes be limited by the difficulty of acquiring good interictal or ictal brain SPECT images, as seizures in children may be frequent and brief (such as infantile spasms or myoclonic epilepsy).

Interictal 99mTc-ethyl cysteinate dimer SPECT (left image) showing the usual hypoperfusion in presumed epileptogenic focus (arrow) in left frontal cortex region, which becomes hyperperfused during ictal SPECT (right image).
TEMPORAL AND EXTRATEMPORAL LOBE EPILEPSY
PET Imaging
18F-FDG PET has a reported sensitivity of 85%–90% in detection of the epileptic brain region in cases of temporal lobe epilepsy (17–19). 18F-FDG PET can help to identify the epileptic temporal lobe in almost half of patients with noncontributory electroencephalography (20). However, temporal lobe interictal hypometabolic regions often extend beyond the presumed epileptogenic zone. The temporal neocortex is probably involved in most patients with medial temporal lobe epilepsy, and it is difficult to distinguish medial from lateral temporal lobe epilepsy on the basis of 18F-FDG PET patterns (21,22). Patients may show hypometabolism in the ipsilateral parietal and frontal cortex, in the thalamus, and even occasionally in the contralateral temporal lobe (23). This pattern may represent the epileptic network involved in seizure propagation (24) and be related to the behavioral and neuropsychologic changes of chronic epilepsy. 18F-FDG PET can be particularly helpful in dual-pathology cases (coexistence of medial temporal and neocortical seizure foci) or when a secondary noncontiguous epileptic focus due to kindling or similar effects is suspected. In cases of extratemporal epilepsy, 18F-FDG PET does not perform as well, with a reported sensitivity of 45%–92% (generally ∼55%) in localizing the epileptogenic zone in frontal lobe epilepsy (25–27). Poor localization for 18F-FDG PET has also been reported in cases of occipital lobe epilepsy (28). However, considering that the incidence of extratemporal epilepsy is higher in children and that most have normal MR imaging findings, 18F-FDG PET can be useful for clinical management in the pediatric population. 18F-FDG PET can be particularly useful in cortical dysplasia, which appears to be a major etiology for pediatric epilepsy, unlike adult epilepsy, for which hippocampal sclerosis is a major etiology. 18F-FDG PET can also sometimes detect, and thus provide an opportunity for surgical treatment of, heterotopias, which often lead to intractable epilepsy and may be subtle enough to escape detection by MR imaging (Fig. 5).

Axial 18F-FDG PET scan showing subcortical band heterotopia (arrows) in right temporal–occipital white matter in child with intractable epilepsy and normal MR imaging findings. Heterotopic band has higher glucose uptake than adjacent white matter but lower uptake than cortex.
18F-FDG PET can provide additional information about the epileptic focus in up to two thirds of cases, affecting surgical decision making in up to 50%–70% of cases and sometimes changing initial decisions based on MR imaging or electroencephalography (29,30). Further, 18F-FDG PET alone may be the basis for surgical decisions in almost 17% of patients (30). 18F-FDG PET has been found to be most useful when MR imaging findings are negative or when ictal electroencephalography is discordant with MR imaging or seizure semiology (30). 18F-FDG PET findings can also predict surgical outcome, as ipsilateral PET hypometabolism appears to be associated with a good outcome (86%) even in patients with negative MR imaging findings (80%) or with noncontributory ictal scalp electroencephalography (72%) (31). An odds ratio of 7 has been reported for 18F-FDG PET in predicting a seizure-free outcome after epilepsy surgery (32), though it is difficult to predict who will not become seizure-free after surgery (33). In one study, patients with more severe temporal lobe hypometabolism appeared to have better postsurgical seizure control (34). However, in another study, no association was found between surgical outcome and the results of 18F-FDG PET along with MR imaging, electroencephalography, or ictal SPECT (35). The basis for these differences is not entirely clear, but they may be related to confounders such as differences in the patient populations, in the resolutions of the scanners, and in the approaches to image analysis. Medial temporal compared with lateral temporal hypometabolism (36), restricted temporal hypometabolism (37), and greater inferior lateral temporal hypometabolism (20) appear to be independent predictors for seizure control in temporal lobe epilepsy. Contralateral hypometabolism is a negative prognostic factor (38).
Additionally, 18F-FDG PET can provide some other important prognostic information. For example, in patients with unilateral temporal lobe epilepsy, the presence of bitemporal glucose hypometabolism is associated with poor memory performance (39) and prefrontal hypometabolism is associated with impaired executive function (40). Similarly, associated hypometabolism of the ipsilateral insular cortex may correlate with emotional or somesthetic symptoms (41). Bilateral lateral temporal and bilateral medial prefrontal hypometabolism may be associated with interictal aggressive behavior, probably because of removal of the inhibitory effects of the temporal neocortex (and perhaps the medial prefrontal cortex) on the medial temporal lobe (42). Thalamic glucose metabolism can be an independent predictor of surgical outcome in patients with temporal lobe epilepsy, with thalamic hypometabolism contralateral to the epileptic foci relating to poor surgical outcome, compared with ipsilateral or no thalamic hypometabolism (43).
Under specific circumstances, some other radiotracers can be more useful than 18F-FDG for evaluating epilepsy. For example, 11C-flumazenil may sometimes show a smaller area of abnormality than does 18F-FDG PET (19,44). 11C-flumazenil PET is sensitive in temporal lobe epilepsy (19), particularly in cases of a sclerotic hippocampus (45). 11C-flumazenil PET has been reported to have a sensitivity of up to 100% in the detection of unilateral hippocampal sclerosis, with contralateral abnormalities detected in a third of patients with apparently unilateral hippocampal sclerosis (45,46). In MR imaging–negative temporal lobe epilepsy, 11C-flumazenil PET results have been found to be abnormal in up to 85% of patients (47). In cases of extratemporal lobe epilepsy, 11C-flumazenil PET has been shown to have a sensitivity of 60%–100% for detecting the epileptogenic cortex using intracranial ictal electroencephalography as the gold standard (19,48,49), and complete resection of the 11C-flumazenil abnormality has been found to be associated with good seizure outcome, even in children with normal MR imaging results (48,50). Contrary to 18F-FDG PET, which usually shows extratemporal hypometabolism in the parietal and frontal cortex in cases of temporal lobe epilepsy (probably associated with cognitive dysfunction or reflecting diaschisis), decreased 11C-flumazenil binding usually represents neuronal loss or receptor changes related to epileptogenicity and therefore should be more closely scrutinized (46). Use of SPM can further increase the accuracy of 11C-flumazenil PET, allowing detection of subtle changes in 11C-flumazenil binding that are difficult to appreciate visually (41,45). These SPM studies sometimes have also found increased 11C-flumazenil binding, which in some cases has indicated cortical developmental malformations (51). Also, in normal-appearing temporal lobe white matter, the use of SPM has revealed increased 11C-flumazenil binding that was found, on histopathologic examination, to be caused by microdysgenesis (52). This is an interesting finding, as these ectopic neuronal clusters may lead to epileptogenesis by providing an aberrant circuitry.
Several other PET tracers, such as those evaluating tryptophan metabolism or receptors for opiate, histamine, NMDA, acetylcholine, dopamine, and other neurotransmitters, have been developed and used in epilepsy (Table 1). One study found 11C-α-methyl-l-tryptophan PET to be useful in patients with temporal lobe epilepsy and a normal hippocampal volume (53). This tracer appears to be especially useful in cases of cortical dysplasia with normal MR imaging findings and mild 18F-FDG changes. In such cases, the tracer sometimes shows increased uptake, particularly in patients with cortical dysplasia type IIB, who usually have a good surgical outcome (Fig. 6) (54). This is an important development, as it indicates that there appears to be an in vivo imaging technique that can predict pathologic subtype and thus may provide presurgical prognostic information. Studies of opiate receptor PET imaging have reported both increased (55) and normal (56) receptor density in patients with temporal lobe epilepsy, whereas lower receptor availability was reported in the left parietotemporooccipital cortex in patients with reading epilepsy (57). Available data suggest that there is endogenous opioid release during the ictal phase, resulting in reduced receptor availability and reduced tracer binding, followed by low levels of endogenous opioids, resulting in increased receptor availability and therefore increased tracer binding. Similarly, the level of monoamine oxidase B has been found to be both high (58) and low (59) in temporal lobe epilepsy. Although significantly reduced dopamine receptor binding has been reported in the epileptogenic temporal lobe in temporal lobe epilepsy (60), no binding alterations were found with PET using 11C-verapamil, a p-glycoprotein substrate (61). Patients with temporal lobe epilepsy have also been found to have reduced NMDA receptor binding (62) but increased 11C-doxepine uptake (63) in the ipsilateral temporal cortex. Although one group found reduced dopamine-1 receptor binding in the right putamen in autosomal dominant nocturnal frontal lobe epilepsy (64), another group found increased tracer binding to nicotinic acetylcholine receptors in the midbrain, pons, and cerebellum and reduced binding in the dorsolateral prefrontal cortex in this condition (65). Recently, evidence of inflammatory changes was shown using 11C-PBR28 (N-acetyl-N-(2-11C-methoxybenzyl)-2-phenoxy-5-pyridinamine), a marker of activated microglia-mediated neuroinflammation, in the hippocampus, parahippocampal gyrus, amygdala, and fusiform gyrus ipsilateral to the epileptic focus in patients with temporal lobe epilepsy (66). Although this is a preliminary finding and it is not clear whether observed neuroinflammatory changes are the cause or the effect of seizures, these observations are quite interesting and encouraging. However, there have not been many studies involving these tracers, and there has been no class I evidence; furthermore, the findings have been mixed and variable. In addition, most of these studies come from only a handful of centers. Therefore, more data are required before a valid conclusion can be reached about the usefulness of the findings in epilepsy evaluation.
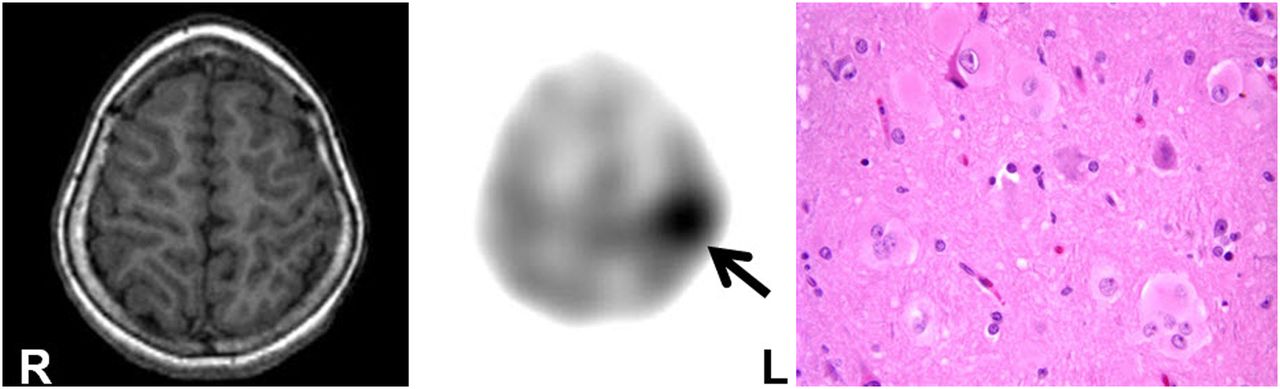
11C-α-methyl-l-tryptophan PET scan (middle image) showing increased tracer uptake in left parietal lobe (arrow) in child with intractable epilepsy and normal findings on MR imaging (left image). Postsurgical histopathology (right image) revealed type IIB cortical dysplasia with balloon cells (×40, hematoxylin and eosin). Child remains seizure-free after epilepsy surgery.
SPECT Imaging
SPECT can reveal focal perfusion abnormalities concordant with other noninvasive presurgical examinations in up to 95% of patients (14,15,67–69). However, the overall sensitivity for interictal SPECT is low (<50%) for the detection of epileptogenic regions in temporal lobe epilepsy, with false-positive or false-negative findings in 20%–75% of cases. In contrast, ictal SPECT can correctly localize the epileptogenic focus in 70%–90% of cases with unilateral temporal lobe epilepsy (68,70–72). False localization is usually due to rapid seizure propagation or subclinical seizure onset. In addition, resection of the SPECT focus has been found to be associated with a favorable surgical outcome (67). The use of SISCOM can increase the focus detection rate by up to 93%, compared with 74% without it (Fig. 7) (73). The sensitivity of postictal SPECT (70%–90%) has also been reported to be greater than that of interictal SPECT and can further improve with use of SISCOM (74). However, in extra–temporal lobe epilepsy, SPECT may not be as useful, as seizures are brief and propagate rapidly, thus making it difficult to acquire an ictal SPECT study, and a much lower sensitivity (66%) has been reported for ictal SPECT (75). Interestingly, in 2 studies, ictal SPECT or SISCOM was found to be more sensitive than 18F-FDG PET in the detection of epileptic foci (76,77). However, in another study of occipital lobe epilepsy, ictal hexamethylpropyleneamine oxime SPECT was found to be less sensitive than 18F-FDG PET (78). SISCOM appears to increase the diagnostic yield in extra–temporal lobe epilepsy patients also and correlates better with postsurgical outcome (16,32).
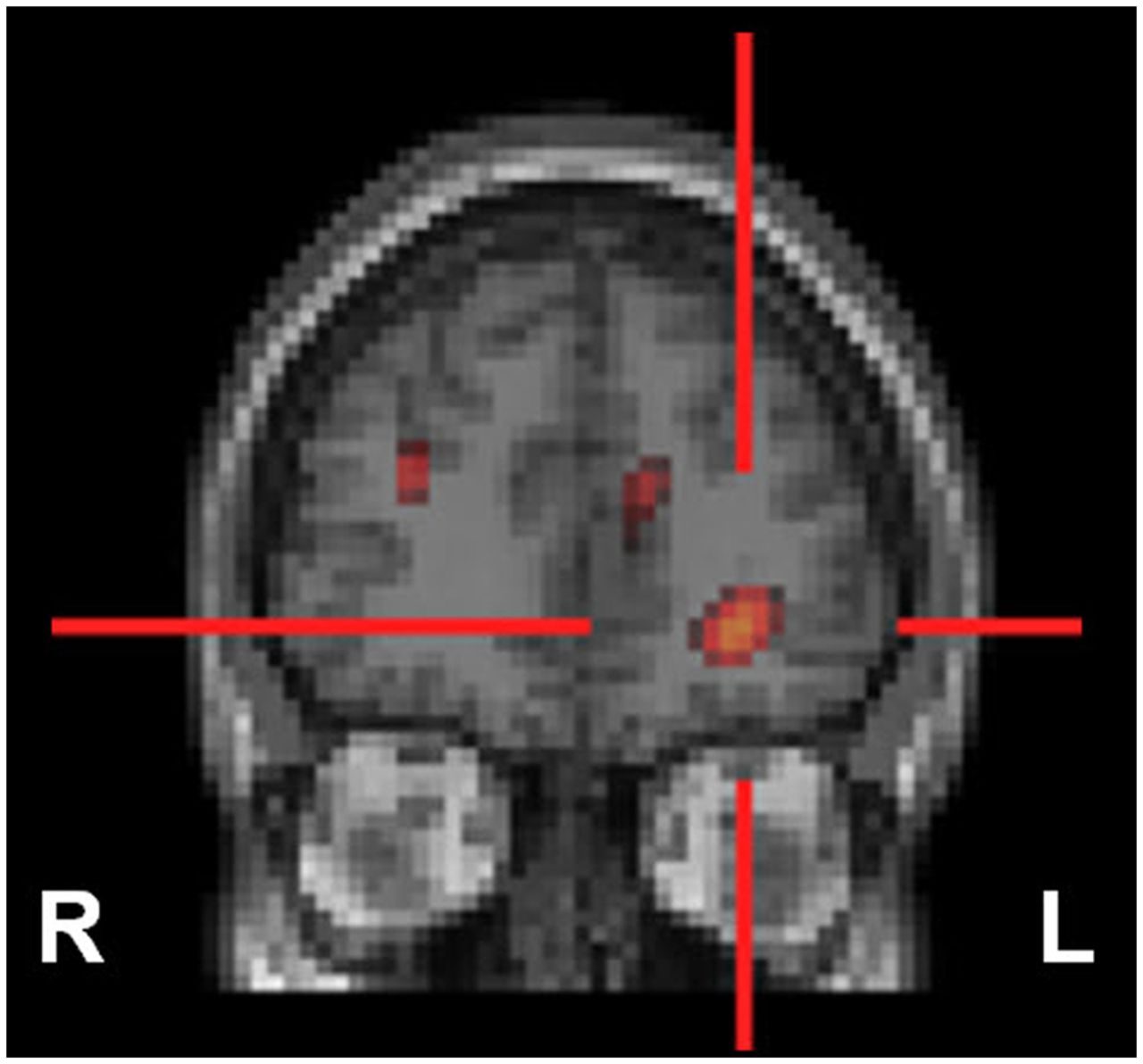
SISCOM may result in better delineation of epileptogenic focus, which may sometimes be missed even on ictal SPECT. In child with intractable complex partial epilepsy with normal findings on MR imaging and nonlocalizing scalp electroencephalography, SISCOM revealed focus of hyperperfusion in left inferior frontal cortex (red cross), likely representing seizure focus.
CONCLUSION
Radionuclide imaging such as PET and SPECT can play an important role in noninvasive presurgical localization of epileptogenic brain regions in patients with intractable seizures who are being considered for epilepsy surgery. Radionuclide imaging may be particularly useful if MR imaging findings are negative or show multifocal lesions of which only 1 or 2 are suspected to be epileptogenic and if electroencephalogram changes are equivocal or discordant with the structural imaging. PET and SPECT can be helpful in evaluating the functional integrity of the rest of the brain and may provide useful information on the possible pathogenesis of the observed neurocognitive and behavioral abnormalities.
Footnotes
CE credit: For CE credit, you can access the test for this article, as well as additional JNMT CE tests, online at https://www.snmmilearningcenter.org. Complete the test online no later than March 2020. Your online test will be scored immediately. You may make 3 attempts to pass the test and must answer 80% of the questions correctly to receive 1.0 CEH (Continuing Education Hour) credit. SNMMI members will have their CEH credit added to their VOICE transcript automatically; nonmembers will be able to print out a CE certificate upon successfully completing the test. The online test is free to SNMMI members; nonmembers must pay $15.00 by credit card when logging onto the website to take the test.
REFERENCES
- Received for publication April 22, 2013.
- Accepted for publication August 6, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}