


Abstract
The Society of Nuclear Medicine and Molecular Imaging and European Association of Nuclear Medicine procedure guide on gastrointestinal transit currently indicates that the mean of total abdominal counts of 7 time points (0–360 min) is used to define the total abdominal counts for bowel transit studies. The purpose of this study was to investigate the variability of total abdominal counts during the initial 6 h of bowel transit and to determine whether a simplified, single-time-point measurement can be used. Methods: Thirty consecutive bowel transit studies were retrospectively analyzed. Patients received an oral dose of 4.6 MBq (125 μCi) of 111In-DTPA in 300 cc of water together with a standard egg white solid-phase, gastric-emptying meal to measure small bowel and colon transit. 111In-DTPA geometric mean and decay-corrected total abdominal counts obtained at 0, 30, 60, 120, 180, 240, 300, and 360 min after meal ingestion were analyzed. The coefficient of variation was used to determine the variability of the mean total abdominal counts. Slope of the regression line, Student t test, and a Pearson product-moment correlation coefficient (PCC) were also calculated to determine the correlation of total abdominal counts at each time point compared with the mean of all time points. Results: The mean coefficient of variation of total abdominal counts of each patient was 3.3%, with a range of 1.1%–6.3%. The mean of the slope of the regression line of the total abdominal counts of the patients was −0.001 ± 0.003. There was no significant difference between the measured slope of the regression line compared with a line with a slope of 0 (P > 0.05). When the counts at each time were compared with the mean counts, there was no significant difference (P > 0.05). The PCC of each of the counts showed a significant and strong correlation between each interval and the mean total abdominal counts (P < 0.01). Conclusion: There is no significant variability in geometric mean 111In-DTPA total abdominal counts during the initial 6 h of bowel transit studies. This can permit a more simplified analysis using the total abdominal counts from only a single time point.
Gastric-emptying scintigraphy continues to evolve with more standardization of imaging protocols (1). Currently, solid-meal, gastric-emptying scintigraphy is most commonly ordered to assess patient symptoms of upper gastrointestinal dyspepsia when gastroparesis is suspected as a cause of a patient’s symptoms. Scintigraphic gastrointestinal transit studies have been expanded to involve the ingestion of a radiolabeled solid, liquid, or combined solid and liquid meal. The liquid phase is used to measure both liquid gastric empting and small bowel and colon transit. A recent practice guideline has been adopted by the Society of Nuclear Medicine and Molecular Imaging (SNMMI) together with the European Association of Nuclear Medicine (EANM), which expands gastric-emptying scintigraphy to include measurement of both small bowel and colon transit (2,3).
Effective, January 1, 2016, 2 new current procedural terminology codes, 78265 and 78266, became available to report gastric-emptying scintigraphy with small bowel and colon transit studies. Therefore, studies of the motility of the entire gastrointestinal tract (stomach, small bowel, and colon) in which the small bowel alone or small bowel and colon transit are continuations of the gastric-emptying scintigraphy study can now be performed.
The current SNMMI EANM Practice Guideline on gastrointestinal transit indicates that the mean of total abdominal counts from 7 individual time points from 0 up to 360 min should be used to define the total abdominal counts available to fill the terminal ileum and colon when quantifying small bowel and colon transit studies (3). This recommendation was based on early studies using older γ-cameras in which there was concern for potential nonuniform counting rates from the photomultiplier tubes and that there could be significant variability in the measurement of total abdominal counts due to variable bowel geometry and depth-related attenuation of counts over the multiple imaging time points.
We have observed in many small bowel and colon transit studies, however, that there is little variation in the measurement of the total abdominal counts that is used to calculate the percentage of activity in the terminal small bowel at 6 h after meal ingestion and the geometric centers of colon activity at 24, 48, and 72 h. The purpose of this study, therefore, was to investigate the variability of geometric mean total abdominal counts during the initial 6 h of small bowel transit imaging and to determine whether a single-time-point measurement could be used to simplify the analysis.
MATERIALS AND METHODS
This was a retrospective review of prior patient imaging studies and data. Our institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived. Thirty consecutive patient studies from a 3-mo period that were performed to measure combined small bowel and colon transit as part of a dual-isotope mixed solid and liquid meal were retrospectively analyzed. The study population included 35 women and 5 men. Patients were aged 20–69 y. The mean body surface area of the patients was 1.76 m2 (Du Bois method), with a range of 1.37–2.33 m2 (Table 1).
Patient Demographics
All acquisition parameters followed the SNNMI and EANM Practice Guideline using a combined liquid water and egg white, solid-phase meal to record gastric emptying as well as small bowel and colon transit (3). Patients received an oral dose of 4.6 MBq (125 μCi) of 111In-DTPA in 300 cc of water combined with 37 MBq (1.0 mCi) of 99mTc-sulfur colloid in 120-g cooked liquid egg white in a meal including 2 slices of white bread and 30 g of strawberry jam.
A large-field-of-view γ-camera, Millenium MPR (GE Healthcare), was used for imaging. All images were obtained in a 128 × 128 pixel matrix using a medium-energy collimator. The photopeak setting for 99mTc is 15% at 140 keV. Both the 172- and the 247-keV peaks for 111In with 15% windows were used.
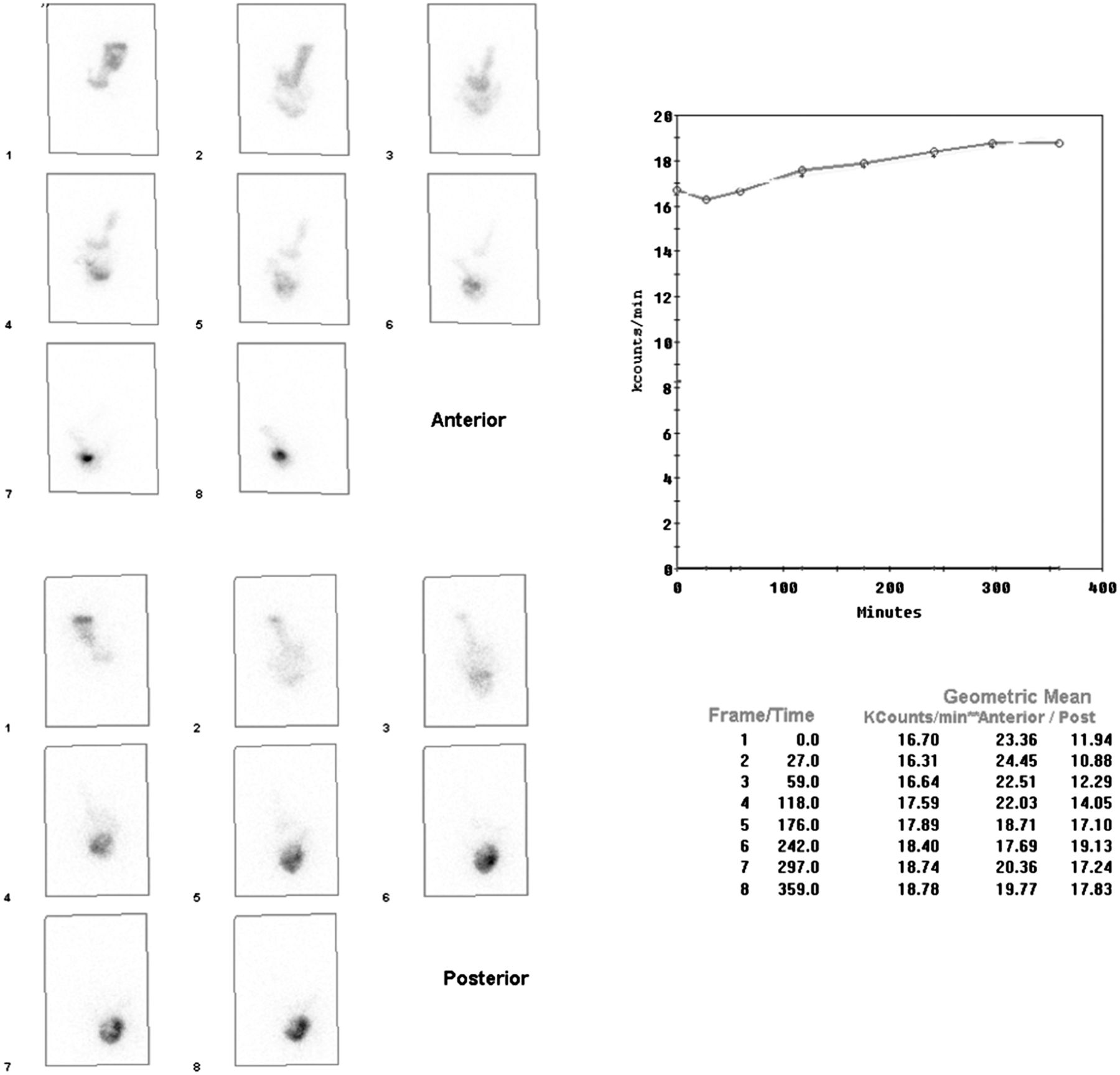
To obtain the 111In-DTPA total abdominal counts, large rectangular manual regions of interest were drawn to encompass the entire abdomen and to determine the 111In-DTPA geometric mean and decay-corrected counts at times 0, 30, 60, 120, 180, 240, 300, and 360 min after meal ingestion (Figs. 1–3; Table 2). We obtained an additional set of images at 30 min. Although this is not required by the SNNMI and EANM Practice Guideline on gastrointestinal transit, this is added at our institution to help in evaluation of gastric accommodation and potential rapid gastric emptying.

Anterior and posterior 111In-DTPA images of abdomen are shown with examples of large rectangular regions of interest used to obtain total abdominal counts for calculation of geometric mean and decay-corrected total abdominal counts for all time points. There is small time point–to–time point variation in total abdominal counts; however, variation from mean is always less than 10% (Table 2).
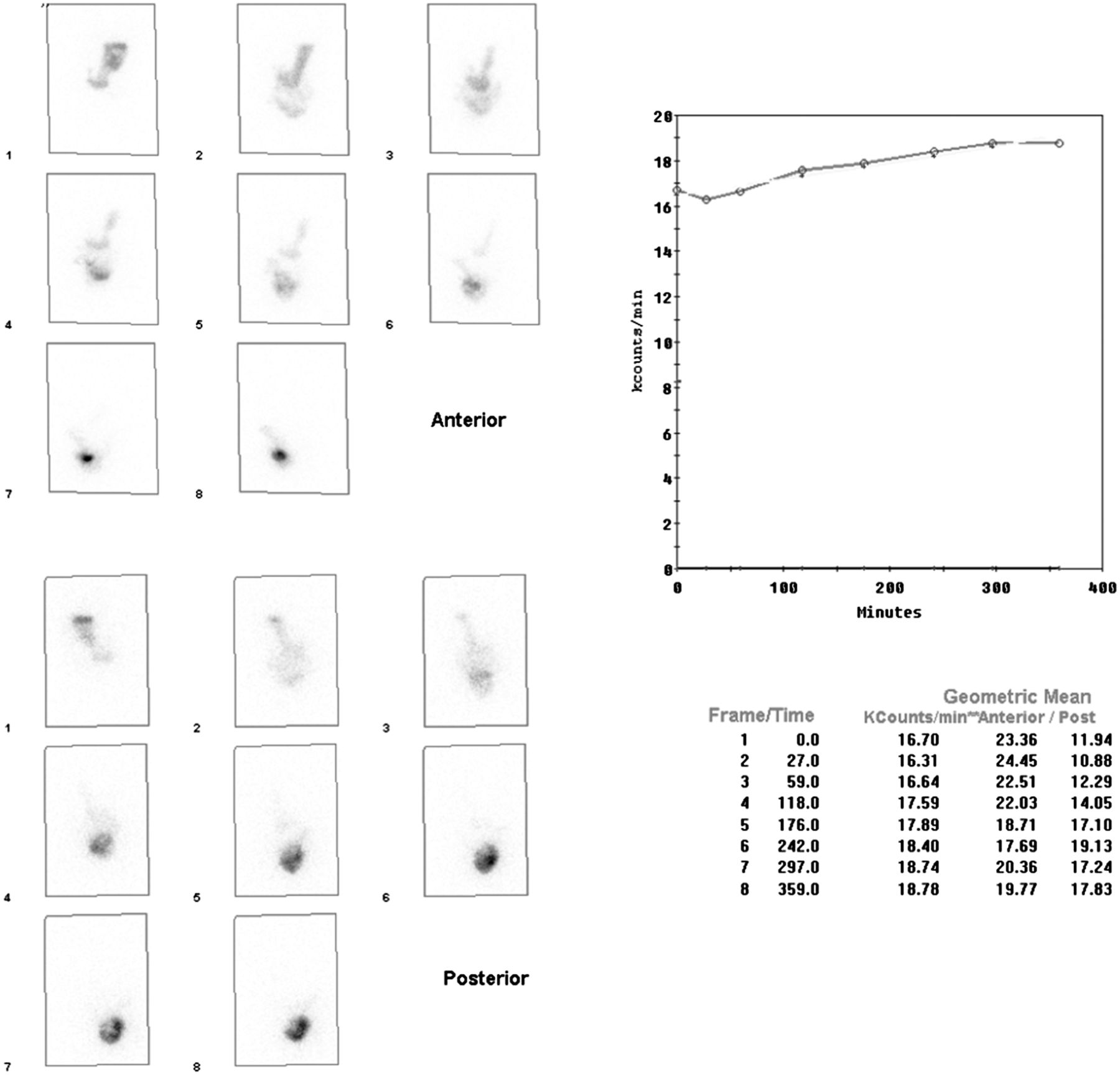
Orientation and regions shown are same as in Figure 1, however, this figure shows example of patient in whom there is mild increase in total abdominal counts over course of 6 h of imaging.

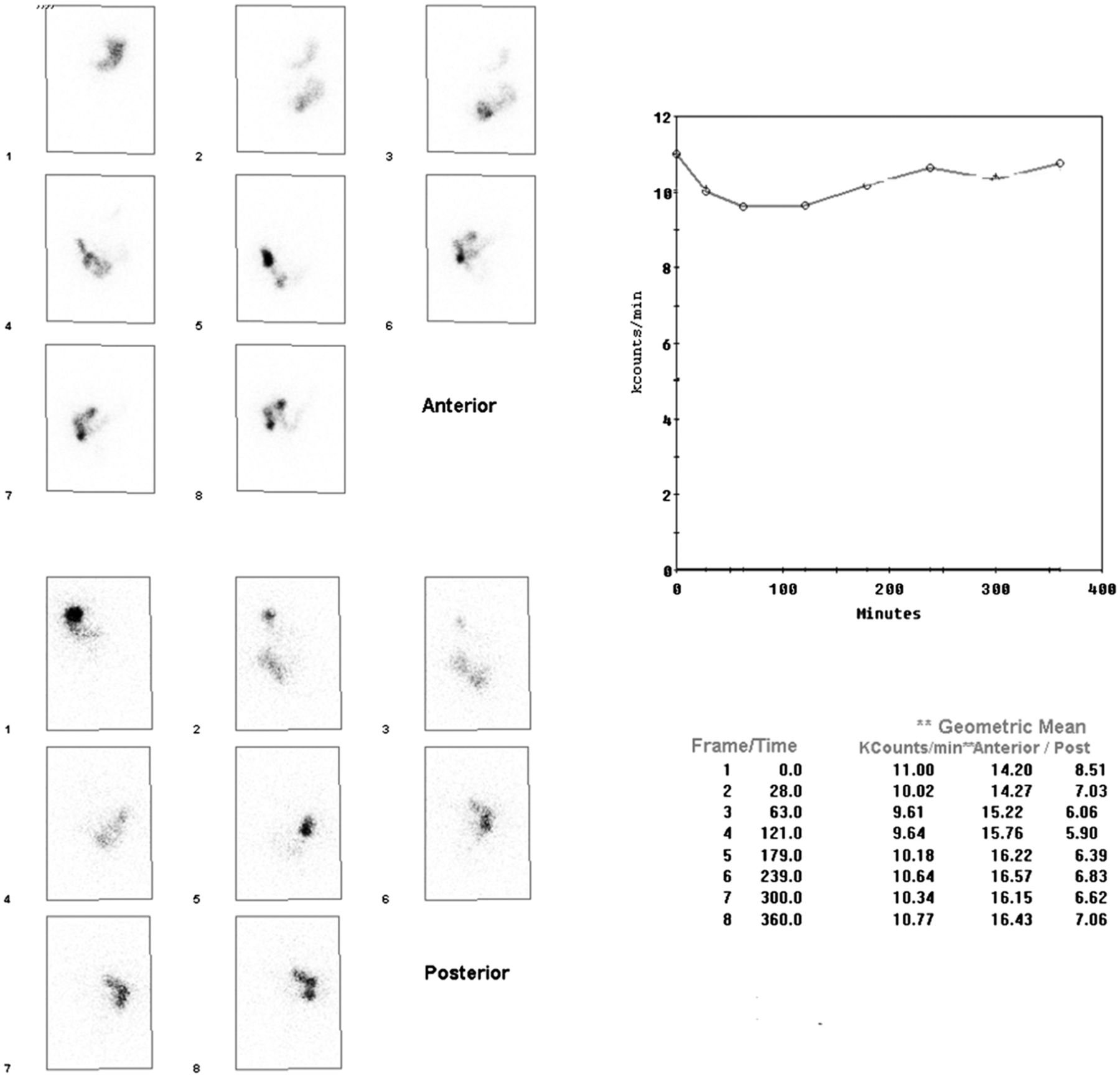
Orientation and regions shown are same as in Figure 1, but in this case there is mild decrease in total abdominal counts over course of 6 h of imaging.
Summary of Measured Total Abdominal Counts (Kcounts/min) for All Patients and All Time Points
The coefficient of variation was used to determine the variability of the mean of the total abdominal counts for each patient. The slope of the regression line, Student t test, and a Pearson product-moment correlation coefficient (PCC) were also calculated to determine the correlation of the time–activity curve at each time point compared with the mean of all time points.
RESULTS
The mean coefficient of variation of time–activity curve of each patient was 3.3%, with a range of 1.1%–6.3%. The mean of the slope of the regression line of the measured counts of the patients was 0.001 ± 0.003. There was no significant difference between the measured slope of the regression line compared with a line with a slope of 0 (P > 0.05). When the counts at each time were compared with the mean counts, there was no significant difference (P > 0.05). The PCC of each of the counts showed a significant and strong correlation between each interval and the mean counts (P < 0.01).
DISCUSSION
Indications for gastric-emptying scintigraphy with small-bowel and colon transit imaging include, but are not limited to, evaluation of gastrointestinal tract transit abnormalities as a cause of symptoms in patients with known or suspected gastroparesis, dyspepsia, irritable bowel syndrome, chronic constipation, chronic diarrhea, chronic idiopathic intestinal pseudoobstruction, scleroderma, celiac disease, and malabsorption syndromes. In the evaluation of patients with constipation, gastrointestinal transit measurements may demonstrate a motility disorder or slow colon transit or may provide evidence to support a diagnosis of defecation disorder or functional rectosigmoid obstruction.
The American Neurogastroenterology and Gastrointestinal Motility Society and the European Society of Neurogastroenterology and Motility have stated in a position paper that whole-gut transit scintigraphy (combined gastric emptying with small bowel and colon transit) is recommended for “detection of altered small-intestine transit in subjects with suspected diffuse gastrointestinal motility disorder” and that colon transit scintigraphy “offers reproducible and accurate performance, to measure regional colon transit in patients with suspected colonic motility disorders or more diffuse disorders involving the stomach or small intestine” (4). The recent approval of new current procedural terminology codes to perform both small bowel and colon transit studies will likely result in an increased volume of these studies being performed. The results of this study show that there can be considerable time savings in the processing of these studies using a single time point for total abdominal counts rather than measuring the mean total abdominal counts of the current recommended 7 time points. On the basis of the results of this study, use of a single-time-point measurement for total abdominal counts will result in only a small change in the values calculated for small bowel transit (percentage of activity in the terminal ileum) and geometric centers of colon transit (mean variation of 3.3%, with a range of 1.1%–6.3%).
There was consistency and lack of significant variability in measured total abdominal counts found in this study over the 8 time points measured in a diverse group of patients whose body surface areas ranged from small to large body habitus. This likely relates to the low administered oral 111In-DTPA activity, and therefore no significant dead-time losses or loss of counting efficiency, especially with modern photomultiplier tubes, resulted in low counting losses (5). The geometric mean correction using both anterior and posterior views has also been previously documented to provide good depth attenuation count correction (6,7).
CONCLUSION
There is no significant variability in the measured geometric mean of 111In-DTPA total abdominal counts during imaging of the initial 6 h of small bowel and colon transit studies. This can permit a decrease in the time required for image analysis by potentially obtaining total abdominal counts only from a single time point. Because it is diagnostically necessary to still visually analyze the small bowel and colon transit patterns, imaging at all the recommended 7 time points, however, will still need to be performed.
Footnotes
Published online Nov. 10, 2016.
REFERENCES
- Received for publication August 30, 2016.
- Accepted for publication October 28, 2016.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.