


Abstract
In the ever-changing field of nuclear medicine, best-practice considerations cannot simply go unchallenged for months and years, with the need to minimize radiation exposure to patients highlighted in “as low as reasonably achievable” principles. The Australian Radiation Protection and Nuclear Safety Agency reports that the dose for 99mTc-macroaggregated albumin (99mTc-MAA) administered should be 180–200 MBq. An objective of imaging in pulmonary embolism, or indeed any diagnostic procedure involving radiation, is to minimize radiation exposure without sacrificing image quality and diagnostic accuracy. The amount of radiation involved must be considered together with imaging protocols. Our aim was to reduce the amount of 99mTc-MAA administered without compromising the diagnostic quality of the scan. Methods: To achieve a ventilation-to-perfusion ratio of 1:4, we ventilated the patient as per standard protocol and then placed intravenous access into the patient. For the perfusion component, 180–200 MBq were prepared in a 2-mL injection. Aliquots of 0.5 mL of 99mTc-MAA were administered every 30 s followed by a 5-mL saline flush until the required ventilation-to-perfusion ratio was achieved. Results: With this protocol, the average administered dose was 105 ± 20.7 MBq (vs. 180 ± 5.3 MBq, P < 0.0001). Conclusion: By individually tailoring the administered dose, diagnostic quality is maintained while achieving a significant dose reduction.
In the ever-changing field of nuclear medicine, best-practice considerations cannot simply go unchallenged for months and years. The need to minimize radiation exposure to patients is highlighted in “as low as reasonably achievable” principles. The Australian Radiation Protection and Nuclear Safety Agency reports that the dose for 99mTc-macroaggregated albumin (99mTc-MAA) administered is 180–200 MBq (1). The Society of Nuclear Medicine and Molecular Imaging reported the dose to be 40–150 MBq (2). When describing the use of aerosols in ventilation–perfusion (VQ) imaging, the society states that “Because both agents are labeled with 99mTc, it is extremely important that the counting rate of the second study is at least 3 to 4 times the counting rate of the first study” (2,3).
One objective of imaging in pulmonary embolus detection or indeed any diagnostic procedure involving radiation is to minimize radiation exposure without sacrificing image quality and diagnostic accuracy (4). The amount of radiation involved must be considered together with imaging protocols. We aimed to reduce the amount of 99mTc-MAA administered without compromising the diagnostic quality of the scan.
MATERIALS AND METHODS
In a VQ lung scan at St. F.X. Cabrini Hospital, the patient inhales 99mTc-Technegas for the ventilation component: 1,000−1,500 cps as detected on the γ camera, or 700 cps over the right lung using a Geiger counter measurement. The dose administered equates to approximately 40 MBq (3). For the perfusion component, we administer 180–200 MBq of Technescan LyoMAA (Mallinckrodt) intravenously. The detected 99mTc-MAA counting rate must be at least 4 times greater than the ventilation component (2).
Our routine acquisition is SPECT with low-energy high-resolution collimators, 48 views over 180° using 2 detectors. The matrix is 128 × 128, and the zoom is 1.23. The ventilation imaging is performed at 12 s/stop, and the perfusion imaging at 10 s/stop (5–8).
A control sample of 10 patients underwent lung scanning using the standard 180–200 MBq (average, 185 MBq ± 5.27 [SD]) Technescan LyoMAA dose. A VQ ratio was then calculated for each patient.
Our trial patients were ventilated per the previously discussed standard protocol, and intravenous access was placed with the patient under the camera. For the perfusion component, 180–200 MBq of Technescan LyoMAA were prepared in a 2-mL injection with normal saline. Aliquots of 0.5 mL followed by a 5-mL saline flush were administered every 30 s, and counts were performed over the right lung until a VQ ratio of at least 1:4 was achieved. The residual dose in the syringe was measured to calculate the administered dose. Intravenous cannulas were also measured. It was found that the amount left in the cannula was negligible.
All patients presenting to our department for a VQ study during the period of the trial were included in the analysis; no exclusions were required.
Statistics were analyzed using a Student t distribution test.
Approval for this study was sought and obtained from the Ethics Committee at St. F.X. Cabrini Hospital.
RESULTS
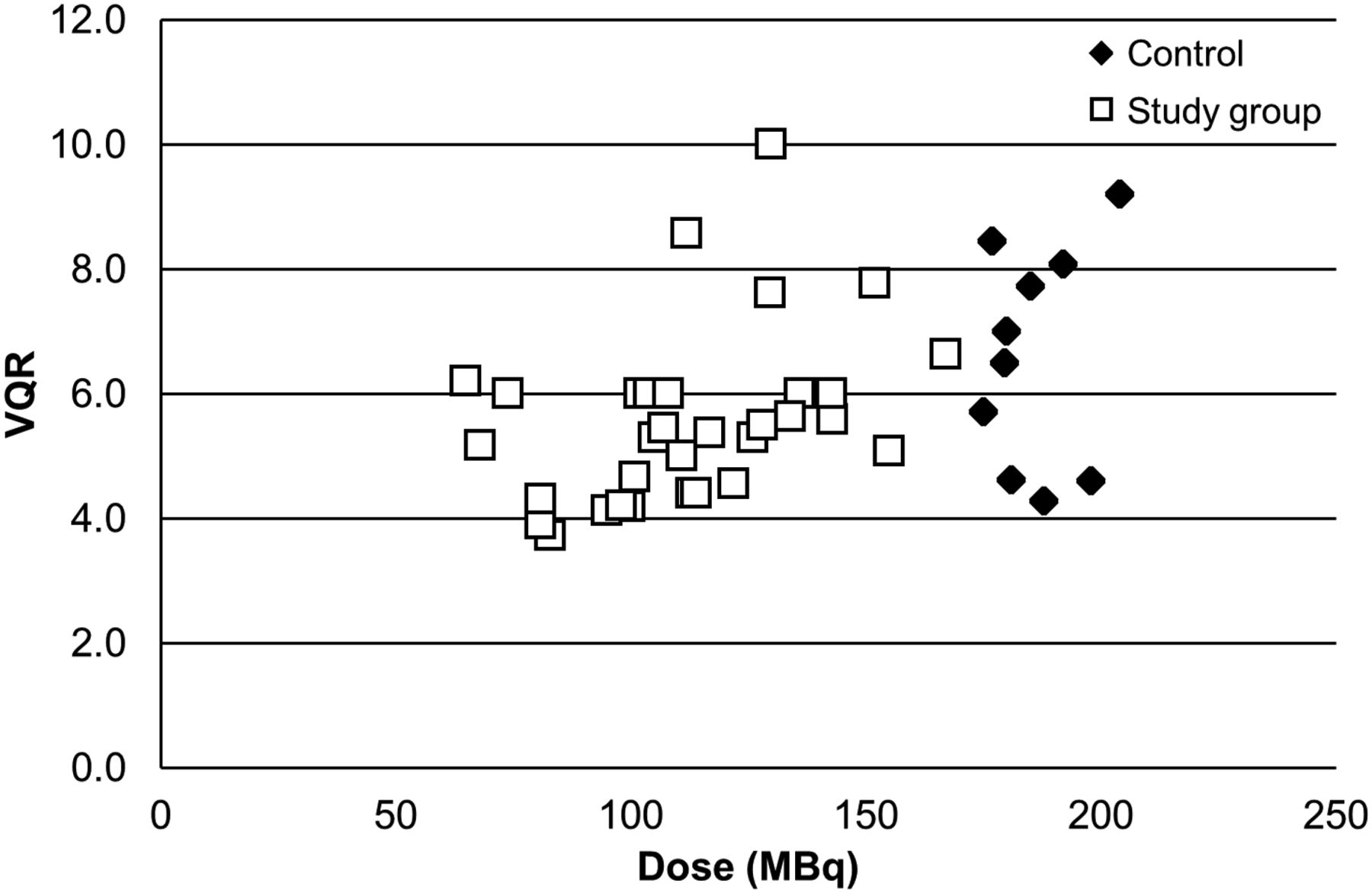
The average administered dose was 105 ± 20.7 MBq for our trial group of 18 patients and 180 ± 5.3 MBq for our controls (P < 0.0001) (Fig. 1).
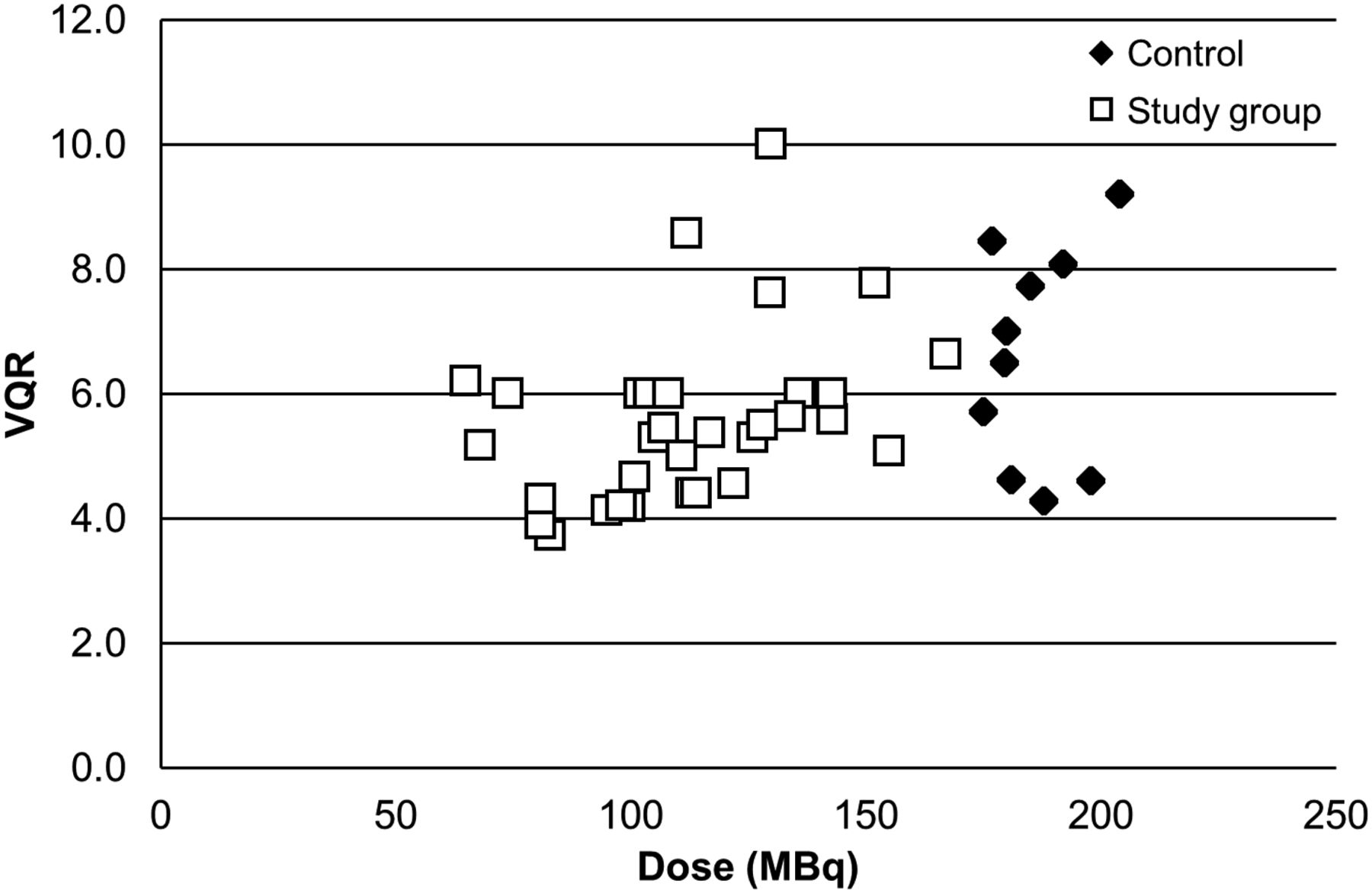
Dose vs. VQ ratio (VQR). Administered perfusion dose of 99mTc-MAA is compared between control group (n = 10) and trial group (n = 18). Although VQ ratio was greater in control patients, value still remained above 4 in trial group while allowing significant reduction in administered dose from 180 ± 5.3 to 105 ± 20.7 MBq (P < 0.0001).
As expected, the VQ ratio was significantly higher in the control group than in the trial group: 1:6.6 ± 1.7 versus 1:4.7 ± 0.7 (P < 0.001). However, the ratio in the trial patients was still over the required 1:4.
DISCUSSION
Perfusion scintigraphy is accomplished by microembolization with radiolabeled particles injected into a peripheral vein. The commercially used particles are MAA, which are labeled with 99mTc. They are 15–100 μm and lodge in the pulmonary capillaries and precapillary arterioles (9,10).
The particle distribution accurately defines regional lung perfusion. An important factor is the number of particles injected. A minimum of 60,000 particles is required to obtain a uniform distribution of activity reflecting regional perfusion. Normally, about 400,000 labeled particles are injected. Bearing in mind that there are over 280 billion pulmonary capillaries and 300 million precapillary arterioles, the administration of up to 400,000 particles will obstruct only a small fraction of pulmonary vessels (11). A reduction in the number of particles administered to between 100,000 and 200,000 is recommended in patients with known pulmonary hypertension, right-to-left heart shunt, or a single transplanted lung. In infants and children, the number of particles may be further reduced in accordance with weight (10–12). To reduce radiation exposure, the dose can be reduced in pregnant women (9–11). Current guidelines have also emphasized the importance of dose minimization in all patient subgroups (9). A diagnostic scan can still be obtained with this reduction in dose. It is this process that prompted the research project to reduce the standard recommended dose.
Our results demonstrate the ability to reduce the dose and not compromise scan quality by following this administration protocol (Fig. 1).
This protocol can tailor the dose to each patient to obtain perfusion images while significantly reducing dose. All scans were clinically indicated and were interpreted by the nuclear medicine physician; each scan in both groups was of excellent diagnostic quality. The sample size was small and a larger series would be useful, but the dose reduction was statistically significant.
The pattern of lung perfusion may be heterogeneous in certain subgroups (e.g., chronic obstructive pulmonary disease), and the ratio was often lower in these subgroups than in patients without such diseases. Whether this specifically affects use of the technique for dose reduction in these subgroups warrants further research.
CONCLUSION
Our novel protocol allows the perfusion dose to be individually tailored to the patient. In this way, a diagnostic scan can be achieved at a significantly reduced dose, thereby decreasing patient and staff exposure alike.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the staff in the Nuclear Medicine Department at St. F.X. Cabrini Hospital for helping to collate the data.
Footnotes
Published online Aug. 13, 2015.
REFERENCES
- Received for publication May 12, 2015.
- Accepted for publication July 1, 2015.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.