


Abstract
The potential of 18F-FDG PET/CT in the diagnosis and treatment response monitoring of fever of unknown origin (resulting from hepatosplenic tuberculosis) is demonstrated in this report. The patient was a 32-y-old woman who had presented to us with a history of pyrexia of unknown origin for the past 2 mo. On investigation, she was found to have hepatic and splenic granulomas, with whole-body 18F-FDG PET demonstrating abnormal 18F-FDG–avid foci in the liver and spleen. Ultrasonography-guided liver biopsy was suggestive of granulomatous hepatitis. The patient was clinically nonresponsive to first-line antitubercular drugs, and second-line antitubercular medications were added subsequently in view of clinical nonresponse. The patient responded well to the treatment. The repeated CT scan at 11 mo demonstrated persistence of the splenic granulomas; however, follow-up 18F-FDG PET/CT at the same time showed resolution of 18F-FDG–concentrating active disease foci with suggestion of complete metabolic response, commensurate with the patient's clinical improvement.
- infectious disease
- 18F-FDG PET/CT
- pyrexia of unknown origin
- tuberculosis
- second-line antitubercular therapy
In recent years, 18F-FDG PET imaging has emerged as an important diagnostic tool in the detection and management of patients with infection and with noninfectious inflammatory disorders (1–4). One important role of this modality is in pyrexia of unknown origin, for which the sensitivity (rather than specificity) of a diagnostic modality is the major issue, because detecting the culprit lesions with high sensitivity would allow for biopsy of those sites. In this communication, we illustrate the 18F-FDG PET/CT findings and pathologic correlation in the work-up and monitoring of such a patient.
CASE REPORT
A 32-y-old woman presented with a history of fever, loss of weight (∼3–4 kg), and loss of appetite for the past 2 mo without a definitive diagnosis of the etiology. She had no past clinical or radiologic evidence of tuberculosis, and clinical examination found no major abnormalities. Her complete blood count and renal function test results were within normal limits. The levels of serum glutamate oxaloacetate transaminase and serum glutamate pyruvate transaminase were marginally elevated, but serum bilirubin was within normal limits. The erythrocyte sedimentation rate was 60 mm at the end of 1 h. She was admitted for investigations and continued to have fever during her hospital stay.
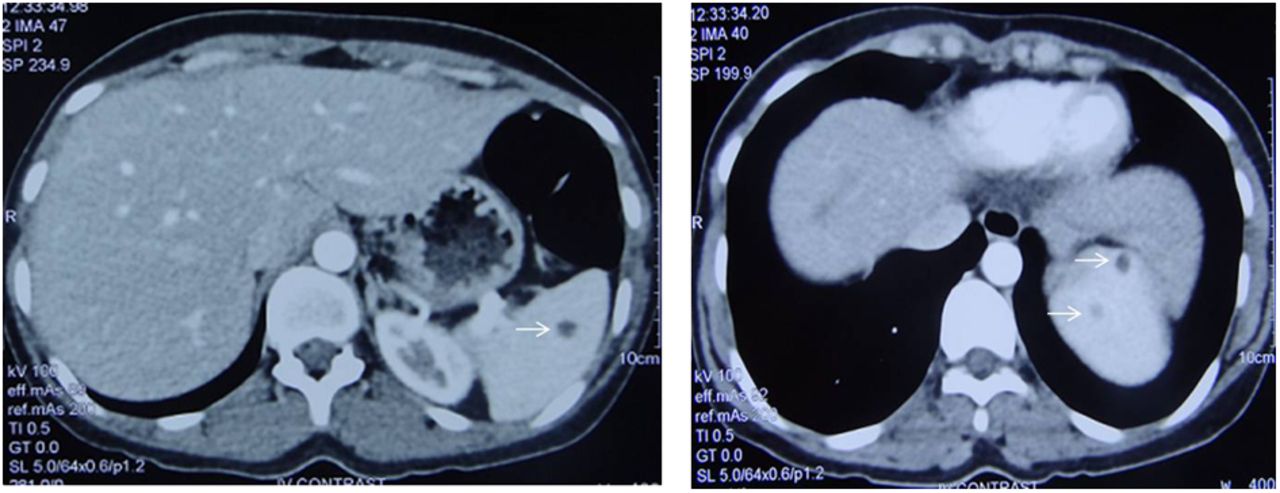
Chest radiography did not reveal any major abnormalities. Ultrasonography of the abdomen revealed multiple hypoechoic areas in the spleen suggestive of granulomas. CT scanning of the chest and abdomen was done subsequently and demonstrated mediastinal adenopathy with minimal necrosis. The liver and spleen demonstrated hypoattenuating lesions suggestive of granulomas (Fig. 1). A few subcentimeter-sized lymph nodes were also seen in the retroperitoneum. Whole-body 18F-FDG PET was undertaken as a part of the work-up for pyrexia of unknown origin and demonstrated abnormal 18F-FDG–avid foci in the liver (maximum standardized uptake value varied from 8.2 to 10) and spleen along with solitary mediastinal node hypermetabolism (Fig. 2). A differential diagnosis of tuberculosis or sarcoidosis was considered. The serum level of angiotensin-converting enzyme was normal. Serum calcium and 24-h urinary calcium were normal. The results of bronchoscopy were normal. Bronchoalveolar lavage did not reveal any acid-fast bacillus, and lung biopsy did not reveal any significant abnormality. We therefore decided to proceed with ultrasonography-guided biopsy of the region of the 18F-FDG–avid liver foci. Histopathologic examination of biopsy specimens (Fig. 3) showed that the liver parenchyma was studded with multiple well-formed, variably sized, discrete, and coalescent granulomas composed of epithelioid cells, Langhans and foreign body giant cells, and lymphocytes. Spotty foci of necrosis were also evident. The histopathologic diagnosis was determined to be granulomatous hepatitis of probable mycobacterial etiology. Tuberculosis polymerase chain reaction on the liver biopsy sample showed the presence of Mycobacterium tuberculosis complex. The QuantiFERON-TB Gold test (Qiagen NV) on whole blood showed the presence of γ interferon. The results of bone marrow examination were within normal limits, the work-up for rheumatologic disorders was unremarkable, serum anti–cyclic citrullinated peptide antibody was normal, SCL-70 IgG antibodies were not detected, anti–nuclear antibody was negative, and anti–histone antibody was negative.

Pretreatment CT scan of abdomen showing hypoattenuating lesions (arrows) in liver and spleen suggestive of granulomas.

Whole-body 18F-FDG PET images demonstrating abnormal 18F-FDG–avid foci (arrows) in liver and spleen along with solitary mediastinal node hypermetabolism.
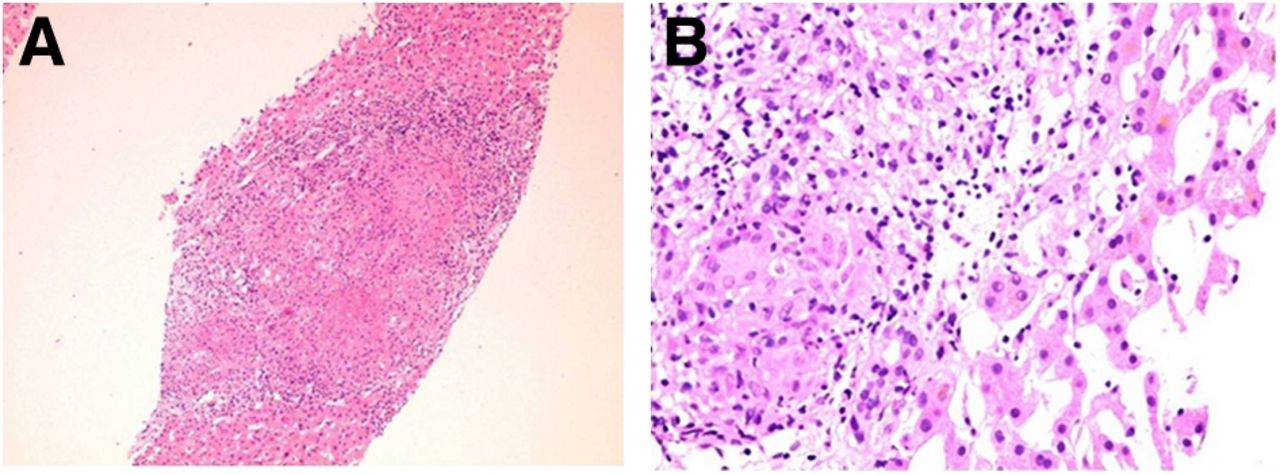
(A) Hematoxylin- and eosin-stained section of liver biopsy sample showing liver parenchyma with epithelioid cell granuloma (×5). (B) Higher magnification of same section showing granuloma composed of epithelioid cells, Langhans giant cells, and lymphocytes (×40).
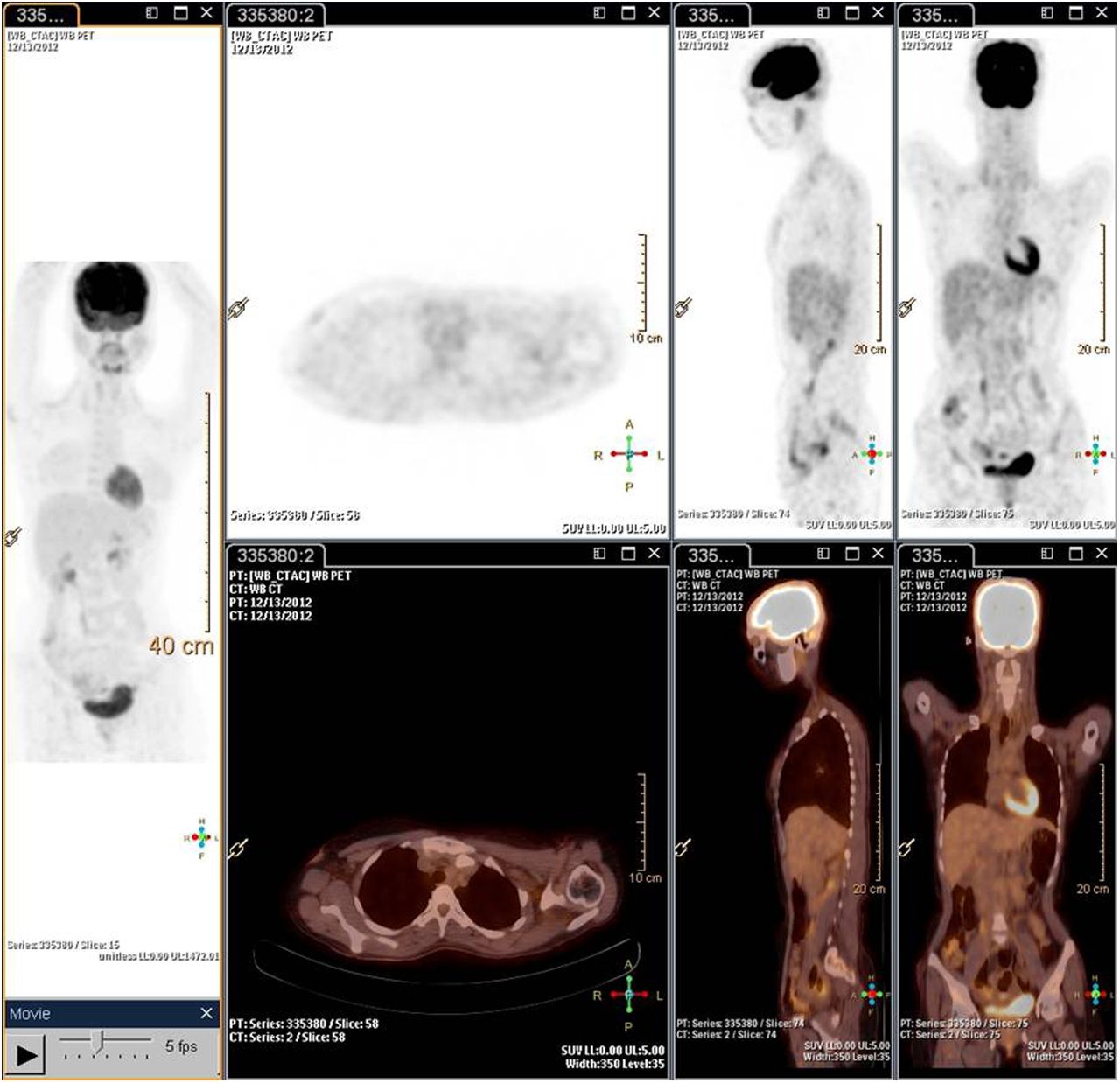
After all these investigations, we decided to start the patient on antituberculosis treatment, beginning with the first-line antituberculous drugs isoniazid, rifampicin, pyrazinamide, and ethambutol. Because the patient continued to have fever and showed no clinical improvement, second-line antituberculous drugs were added: kanamycin, cycloserine, ethionamide, and levofloxacin. The patient responded clinically, the fever responded in a few days, and she was then discharged. She was followed up periodically and showed persistent improvement in the clinical condition. A repeated CT scan at the end of 11 mo demonstrated complete resolution of the lung nodules and the lymphadenopathy but persistence of the splenic granulomas (Fig. 4). A repeated whole-body 18F-FDG PET/CT scan (Fig. 5) at that time showed no evidence of 18F-FDG–concentrating active disease foci and was suggestive of complete metabolic response, as was commensurate with the patient’s clinical improvement. In view of her remarkable clinical, radiologic, and metabolic response, the second-line antituberculous drugs were discontinued and the first-line drugs were continued for 18 mo.

Posttreatment CT scan of abdomen showing resolution of liver lesions but persistence of splenic lesions (arrows).

Follow-up 18F-FDG PET/CT images showing no evidence of 18F-FDG–concentrating abnormal focus in whole-body survey. These results were suggestive of complete metabolic response, as was commensurate with patient’s clinical improvement.
DISCUSSION
18F-FDG concentrates in infection, noninfectious inflammation, and malignancies, the 3 most important causes of pyrexia of unknown origin. Thus, 18F-FDG PET is a sensitive whole-body imaging modality for determining the disease location, although the 18F-FDG–avid foci require further clarification by histopathology. Compared with certain other tumor-specific PET tracers, 18F-FDG is a nonspecific radiotracer, and in the area of cancer imaging, inflammatory diseases are the most common cause of false-positive uptake. This characteristic makes 18F-FDG a catch-all tracer in the scenario of pyrexia of unknown origin. Furthermore, because the metabolic response occurs before the radiologic response, the imaging findings can serve as an important marker in early assessment of treatment response, as was observed in the present case. The emerging role of 18F-FDG PET in early assessment of therapeutic response has also been emphasized in other granulomatous diseases, such as sarcoidosis (3,4). With these potential practical advantages, 18F-FDG PET/CT could completely replace CT in the evaluation of pyrexia of unknown origin as the diagnostic imaging modality of choice in this setting.
CONCLUSION
We have described the usefulness of 18F-FDG PET and PET/CT in the initial workup and for assessment of response to second-line antitubercular therapy in a young patient who had tuberculosis with prominent hepatosplenic involvement. The case classically demonstrates the early appearance of the metabolic response on 18F-FDG PET as compared with radiologic response.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 19, 2014.
REFERENCES
- Received for publication September 21, 2013.
- Accepted for publication December 27, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}