


Abstract
In all reported clinical studies with 18F-FDG–labeled leukocytes, heparin was used as an anticoagulant during labeling. Theoretically, the substitution of heparin with citrate should be advantageous. Methods: Blood from healthy controls was sampled in duplicate, anticoagulated with citrate or heparin, and labeled with 18F-FDG, and the labeling yield was measured. Viability was checked with the trypan blue exclusion technique. Moreover, 4 in vivo PET/CT studies were performed after the reinjection of leukocytes labeled after citrate anticoagulation. Results: The labeling yields obtained with citrate and heparin were not significantly different (P = 0.447). Viability was greater than or equal to 99%. The quality of the PET/CT studies was excellent. In the in vivo studies, the mean labeling yield was 78%—better than or equal to that reported with heparin as an anticoagulant. Conclusion: Citrate is at least as effective as heparin as an anticoagulant, does not (unlike heparin) increase granulocyte activation, and should be the preferred anticoagulant for 18F-FDG labeling of leukocytes.
- 18F-FDG–labeled leukocytes
- 18F-FDG–labeled white blood cells
- inflammation imaging
- vascular graft infection
For many years, scintigraphy after the reinjection of radiolabeled autologous leukocytes has been the cornerstone of infection imaging. Radiolabeling of leukocytes with 111In-oxine was developed in 1976, and radiolabeling with 99mTc-hexamethylpropyleneamine (99mTc-HMPAO) was developed in 1986 (1,2). In the first report, heparin was used as an anticoagulant in the labeling process, whereas citrate in the form of acid–citrate–glucose was used as the anticoagulant for 99mTc-HMPAO labeling of leukocytes. Successful 18F-FDG labeling of human leukocytes was first described in an extensive and detailed report by Osman and Danpure in 1992 (3). They used acid citrate as the anticoagulant. Dextrose (glucose) was not included in the medium because glucose—as shown by the authors—competitively inhibits 18F-FDG uptake by leukocytes. They found that white blood cells (WBCs) were not activated by the method used for their isolation or by the uptake of 18F-FDG. In vivo investigations were not performed.
In 2000, Forstrom et al. reported their work on in vitro labeling of human leukocytes with 18F-FDG (4). They were unaware of the earlier findings of Osman and Danpure (3); after having compared heparin with acid–citrate–glucose as an anticoagulant, they concluded that heparin had to be used to obtain an adequate labeling yield. In a follow-up letter (5), Forstrom regretted having overlooked the findings of Osman and Danpure (3) and admitted that acid–citrate without glucose could be advantageous because heparin might increase granulocyte activation and microaggregation (6).
Because the rationale for using radiolabeled blood cells for clinical studies relies on their biodistribution being the same as that of unlabeled cells, the process of preparing and labeling cells must not alter the behavior of the cells. This concept seems to have been proved for citrate as an anticoagulant but not for heparin. Nevertheless, in all reported studies of 18F-FDG labeling of human WBCs, heparin has been used as an anticoagulant during labeling (7–11).
The aim of our study was to establish whether it might be advantageous to use citrate instead of heparin as an anticoagulant in the process of 18F-FDG labeling of leukocytes.
MATERIALS AND METHODS
In Vitro Studies
Blood samples were drawn from the authors in a euglycemic state. Leukocyte counts per liter varied from 4.8 × 109 to 8.6 × 109 (the range of normal blood leukocyte counts per liter is 4.0 × 109–11.0 × 109). Typically, a 25-mL sample of blood was anticoagulated with isotonic acid–citrate or heparin. The citrate- and heparin-treated samples were thereafter divided into 3 vials each. Subsequent labeling was performed as a downscaled version of our routine method for 99mTc labeling of leukocytes, except that leukocytes were resuspended and incubated not in cell-free plasma (which contains glucose that inhibits 18F-FDG uptake) but in isotonic citrate (National Isotope Pharmacy; 1,000 mL contains 8.0 g of citric acid·1H2O, 22.0 g of sodium citrate·2H2O, 3.6 g of sodium chloride, and sterile water up to 1,000 mL; pH 4.5–5), Ringer acetate, physiologic saline, or phosphate-buffered saline (PBS). Moreover, 99mTc-HMPAO incubation at room temperature was substituted with 18F-FDG incubation at 37°C. Twenty-seven subsamples were labeled. The trypan blue exclusion test was used to check viability after labeling (4,10). The Student t test for paired samples was used for statistical evaluation of the labeling yield.
In Vivo Studies
For in vivo studies, a full-scale in vitro labeling procedure was performed. Autologous blood (51 mL) was aspirated into 9 mL of sterile isotonic citrate. Erythrocyte gravity sedimentation was induced by the addition of 5 mL of modified gelatin (40 mg/mL; Gelofusine; Danish National Isotope Pharmacy; 1,000 mL contains 40.0 g of succinylated gelatin and 7.0 g of sodium chloride). After adequate sedimentation (45–60 min), aspiration of the supernatant was followed by centrifugation to provide leukocyte pellets; resuspension of the pellets in PBS (produced by the Department of Microbiology, Oslo University Hospital) was followed by centrifugation and aspiration of the supernatant. Thereafter, the pellets were labeled with 370 MBq of 18F-FDG at 37°C for 20 min, with careful swirling every 5 min. The volume of 18F-FDG was 0.2–0.5 mL, depending on the decay of 18F-FDG. Next, the labeled cells were washed with 10 mL of cell-free plasma containing modified gelatin, the radioactivity in the cells and supernatants was measured, and the labeling efficiency was calculated. Finally, the cells were reinjected after resuspension in 5 mL of cell-free plasma without modified gelatin. The regional ethics committee had no objections to the clinical use of autologous leukocytes labeled with 18F-FDG as described here.
Whole-body scans were performed on 1 of the authors (control), on 2 patients with persistent fever of unknown origin, and on 1 patient with recurrent sepsis and melena. A Biograph 64 PET/CT scanner (Siemens) was used, and imaging was started 3 h after reinjection of the 18F-FDG–labeled autologous leukocytes. The acquisition time was 4 min per bed. The total acquisition time was about 40 min, depending on the height of the person being scanned and the number of beds.
RESULTS
In Vitro Studies
Resuspension and incubation in isotonic citrate or Ringer acetate yielded only 5%–13% 18F-FDG incorporation and was not evaluated further. The mean labeling yields were 30.2% for citrate anticoagulation combined with resuspension and incubation in NaCl and 31.3% for heparin anticoagulation combined with resuspension and incubation in NaCl (P = 0.279) and 36.5% for citrate anticoagulation combined with resuspension and incubation in PBS and 38.4% for heparin anticoagulation combined with resuspension and incubation in PBS (P = 0.447). The higher labeling yield obtained when PBS was used for resuspension and incubation than when NaCl was used for resuspension and incubation was the only statistically significant difference between groups (P = 0.036). The microscopic trypan blue exclusion test performed with aliquots of 18F-FDG–labeled WBCs immediately after labeling revealed, in all cases, more than 99% unstained viable cells.
In Vivo Studies
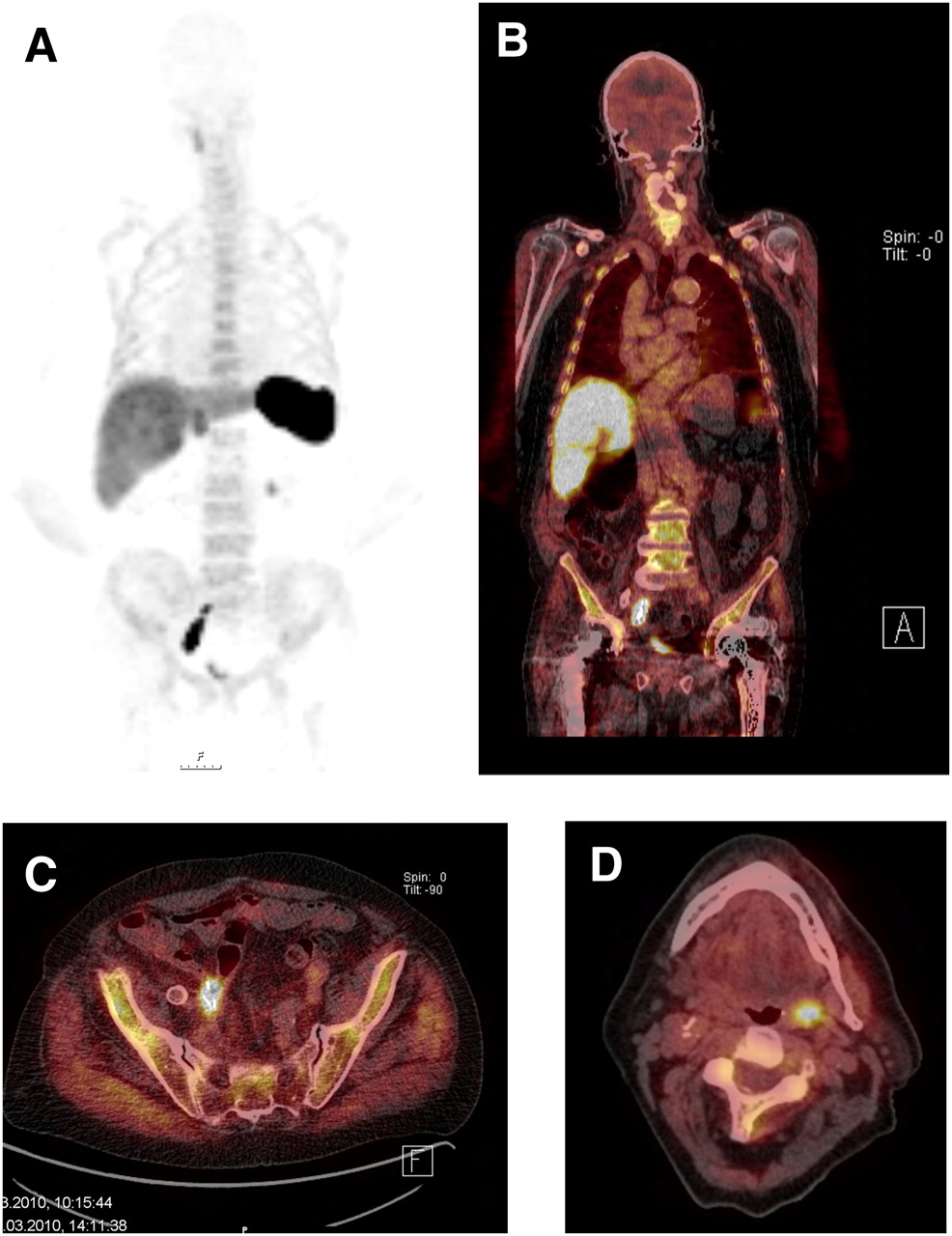
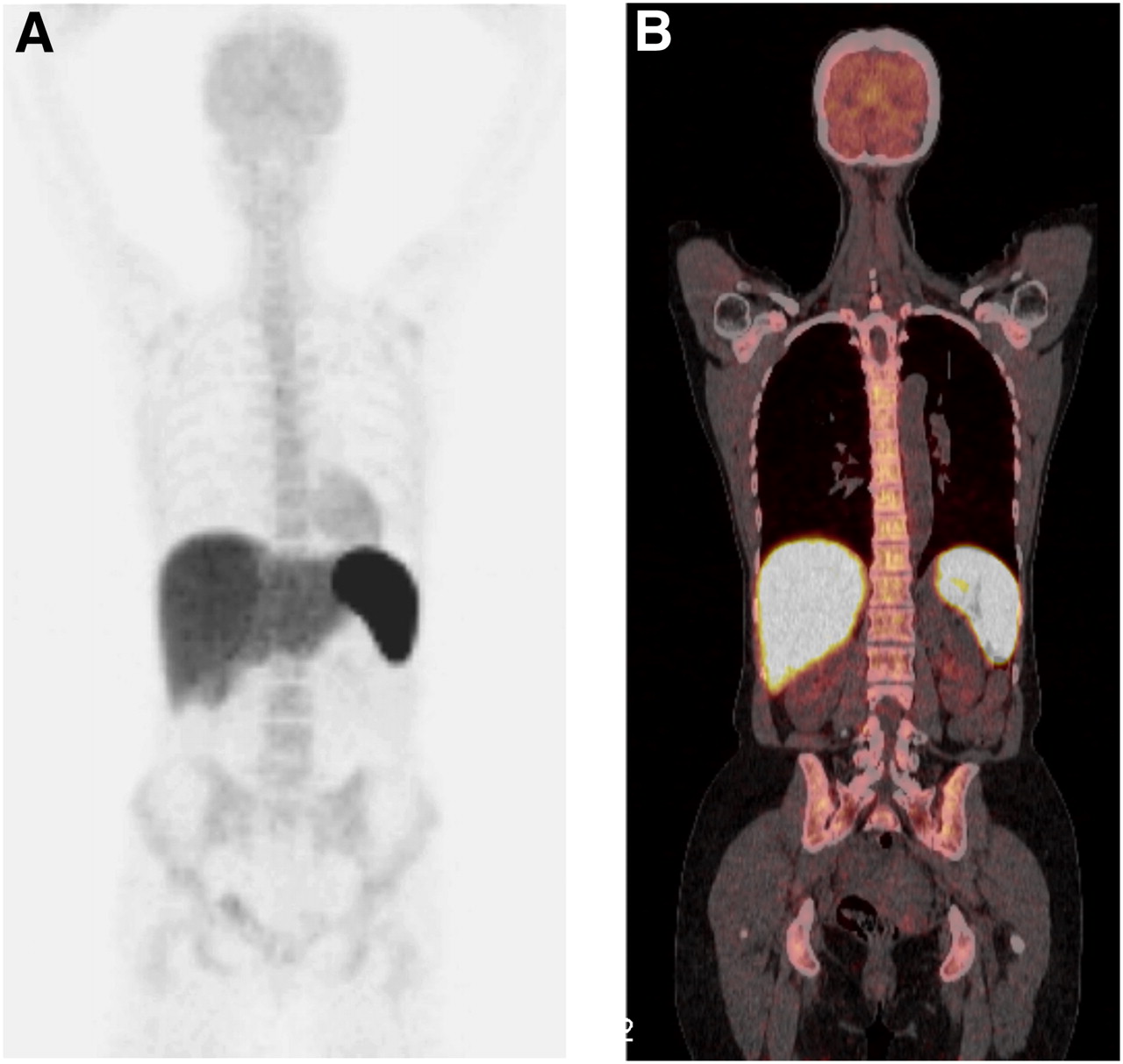
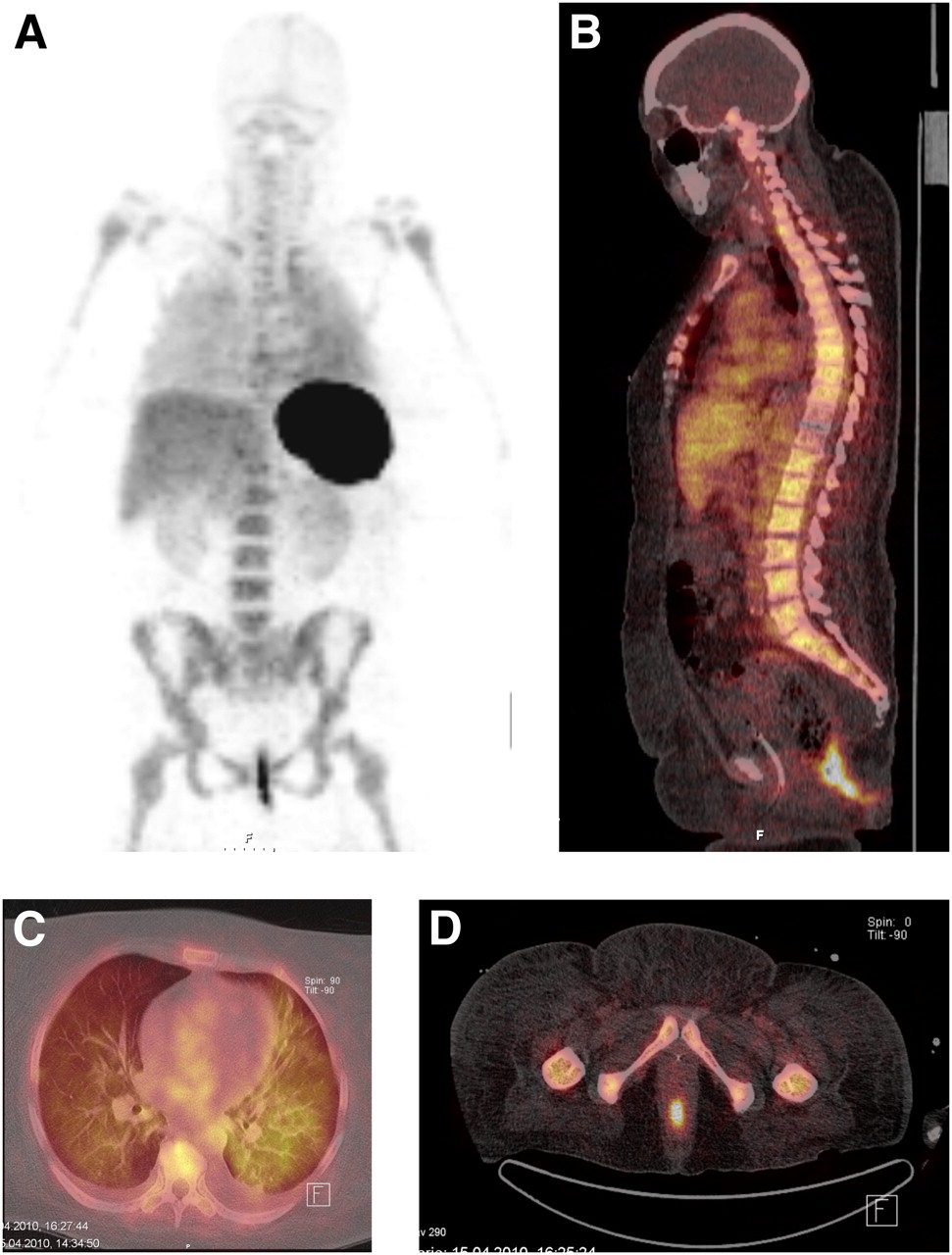
The PET/CT study of the healthy control (leukocyte count, 6.7 × 109/L; labeling yield, 76%) revealed normal leukocyte uptake in the spleen, liver, and bone marrow and only low uptake in the brain and heart caused by 18F-FDG eluted from the WBCs (Fig. 1). In the first patient with fever of unknown origin (leukocyte count, 12.5 × 109/L; C-reactive protein [CRP] level, 80 mg/L [a normal CRP level is <4 mg/L]; labeling yield, 70%), no pathologic deposition of labeled WBCs was found. In the second patient with fever of unknown origin (leukocyte count, 14.4 × 109/L; CRP level, 40 mg/L; labeling yield, 86%), pathologic WBC accumulation was found in the small pelvis and the left lung (Fig. 2). The patient with recurrent sepsis (leukocyte count, 8.8 × 109/L; CRP level, 35 mg/L; labeling yield, 79%) had had a Y-graft for an abdominal aortic aneurysm, with the later development of a right-side iliac artery aneurysm, which was treated with a coil and bypassed with a stent–graft from the common iliac artery to the external iliac artery. Postoperatively, he had had conservatively treated episodes of melena and sepsis. His 18F-FDG PET/CT study revealed gross pathology (Fig. 3).
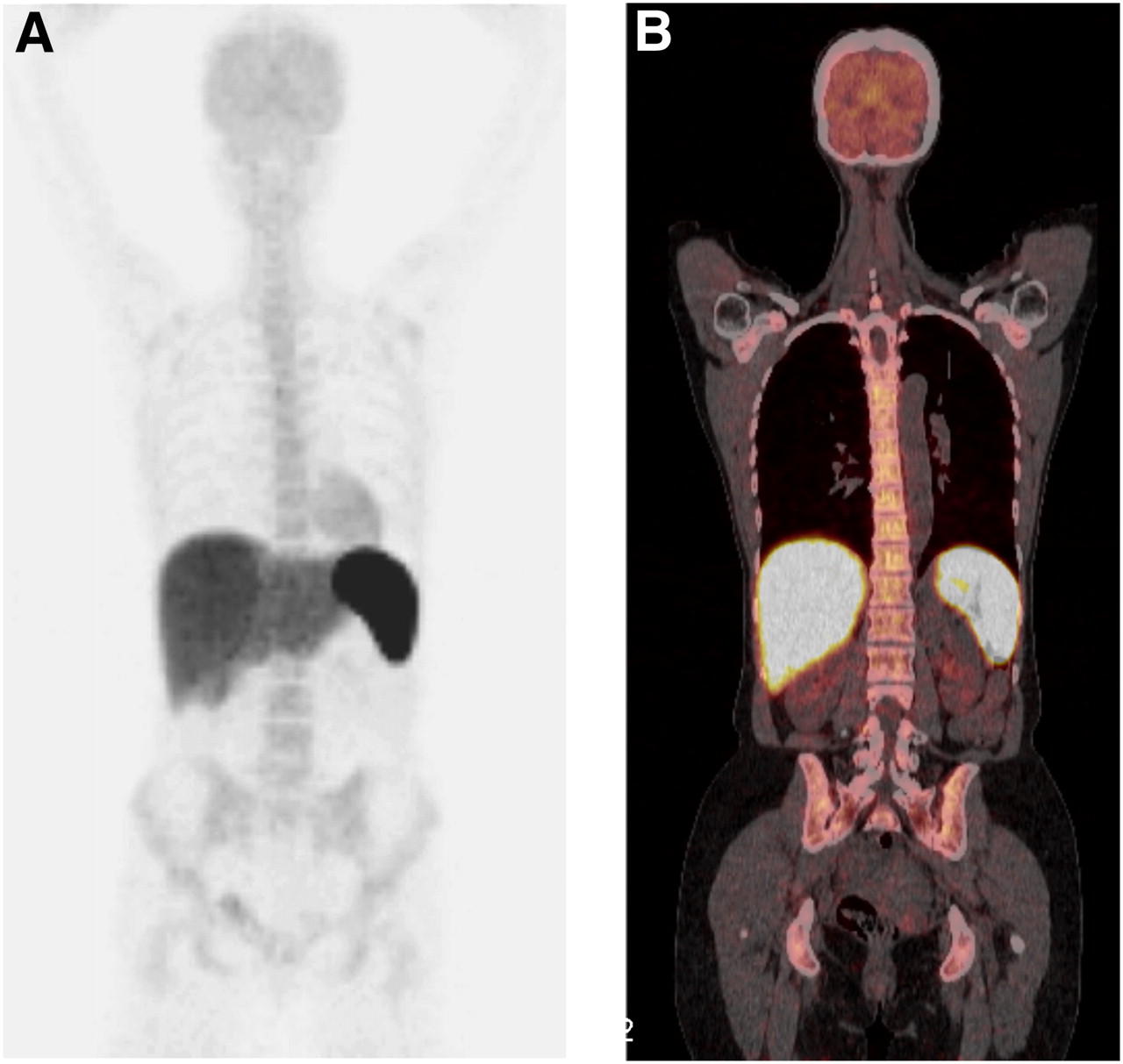
Normal deposition of 18F-FDG–labeled leukocytes in spleen, liver, and bone marrow of healthy control. Faint uptake in brain and heart was caused by 18F-FDG eluted from WBCs. (A) Anterior view from volume-reconstructed image (maximum-intensity-projection image). (B) Coronal section through spine from coregistered PET/CT images.

Pathologic deposition of 18F-FDG–labeled leukocytes in rectum/anal canal (arrows) and in lungs, particularly upper part of left lung, in patient with fever of unknown origin. (A) Anterior maximum-intensity-projection image. (B) Sagittal section through spine from coregistered PET/CT images. (C) Transaxial section through upper part of thorax from coregistered PET/CT images. (D) Transaxial section through lower pelvis from coregistered PET/CT images.
PET/CT with 18F-FDG–labeled WBCs for patient with recurrent sepsis and melena. Markedly increased uptake in coil-treated iliac artery aneurysm corresponded to WBC deposition extending proximal to coil, in parallel with common iliac artery, toward bifurcation. Transaxial section at this level showed air bubble in WBC deposition and apparently in sigmoid colon loop, indicating fistula between abscess and colon. No deposition corresponded to stent–graft to external iliac artery, but increased uptake indicated incidental infection in right tonsillar region. (A) Anterior maximum-intensity-projection image showing pelvic and tonsillar pathologies (arrows). (B) Coronal section through coil-treated iliac aneurysm (arrow) from coregistered PET/CT images. (C) Transaxial section through coil-treated iliac aneurysm (arrow) from coregistered PET/CT images. (D) Transaxial section through tonsillar region (arrow) from coregistered PET/CT images.
DISCUSSION
The low labeling yield in our downscaled in vitro experiments (range, 16%–56%) is explained by the low leukocyte counts in the healthy controls and the fact that our in vitro studies were performed in the afternoon with leftover and decayed 18F-FDG with a low specific activity. For our in vivo studies, fresh 18F-FDG was used, and the labeling yield was 70%–86% (mean, 78%). This labeling yield is better than or equal to that reported by other researchers, who all used heparin as an anticoagulant. Forstrom et al. (7) reported a labeling efficiency of 41%–57% in 4 healthy controls, Pio et al. (8) found a labeling yield of greater than 40% in 3 patients, Pellegrino et al. (9) found a labeling yield of 64%–75% in repetitive labeling of WBCs from the same healthy control, Rini et al. (10) reported average labeling yields of 72% in 37 patients and less than 35% in 6 patients, and Dumarey et al. (11) reported an average labeling yield of 75% in 21 patients.
The present study brings the total reported number of subjects who have had PET with 18F-FDG–labeled autologous WBCs to 76, including 70 patients and 6 healthy controls over a time span of 8 y (2002−2010). The number reported is surprisingly low given that in our institution, we have performed approximately 60 patient studies yearly with the alternative procedure for WBC labeling (using 99mTc-HMPAO), and the experience acquired so far indicates that PET/CT after injection of 18F-FDG–labeled WBCs is a superior method (12).
Generally speaking, the introduction of PET/CT services tends to replace SPECT/CT when competitive positron-emitting imaging agents are available. PET/CT has better diagnostic efficiency because of a high target-to-background ratio, superior image resolution, higher sensitivity, shorter acquisition times, and more reliable quantification and exact localization of pathology. Studies with 18F-FDG–labeled leukocytes can be completed within a day, with little tracer uptake in healthy gastrointestinal and urinary tracts. Brain and heart uptake is faint (Fig. 1) or nearly nonexistent (Figs. 2 and 3). At 3 h, endovascular activity also is nearly nonexistent. In animal experiments, 18F-FDG–labeled WBCs have provided better results than 18F-FDG in all sterile and septic inflammation models (9). For patients, images obtained with 18F-FDG–labeled WBCs can be directly compared with 18F-FDG PET/CT images, and the comparison can differentiate infection or inflammation from tumor uptake.
The potential of PET/CT with 18F-FDG–labeled WBCs is convincingly illustrated by our findings for the patient with recurrent sepsis. This patient had an infection originating from an aortic–bifemoral graft, and the focal infection was clearly visualized in detail. The noninfected part of the graft was not visualized. In contrast, ordinary 18F-FDG PET/CT is more or less useless in patients with vascular grafts because synthetic grafts provoke chronic low-grade aseptic inflammation, which constitutes a site for direct 18F-FDG uptake. Thus, 18F-FDG uptake occurs in most grafts in patients without graft infections (13). On the other hand, scintigraphy with 99mTc-HMPAO–labeled leukocytes and PET with 18F-FDG–labeled leukocytes are highly specific for graft infections because leukotaxis is required for uptake to occur. However, for vascular graft infections, 99mTc-HMPAO scintigraphy may have insufficient sensitivity (14).
Given these facts, why is PET/CT with 18F-FDG–labeled leukocytes not used more extensively? The limiting factors probably are the poor availability, high cost, and labor-intensive nature of PET/CT. In addition, many studies with radiolabeled leukocytes are ordered as emergency investigations; such investigations are difficult for PET centers to conduct on short notice because their schedules are often filled by routine 18F-FDG oncology (and brain) studies for patients on waiting lists that may be long.
According to the results of the present study, the yield from 18F-FDG labeling of leukocytes seems to be equally good when citrate is used instead of heparin for initial blood sample anticoagulation. Moreover, labeling yield is not necessarily the main determinant of WBC efficiency in targeting infection. Effective targeting also requires that the process of preparing and labeling cells does not alter the behavior and biodistribution of the cells relative to those of unlabeled cells. In this respect, citrate anticoagulation has an advantage over heparin anticoagulation during in vitro 18F-FDG labeling of leukocytes because of the risk of granulocyte activation with the latter agent.
The 2004 Society of Nuclear Medicine procedure guideline for leukocyte labeling with 99mTc-HMPAO (15) prescribes citrate as the anticoagulant, whereas the corresponding guideline for the preparation of 111In-labeled leukocytes (16) states that both citrate and heparin may be used. The more recent (2010) European Association of Nuclear Medicine procedure guidelines for the labeling of leukocytes prescribe citrate as the anticoagulant for 99mTc-HMPAO labeling (17) and 111In-oxine labeling (18), and no alternatives are mentioned. Given this information, we see no reason why citrate should not be the preferred agent for 18F-FDG labeling of leukocytes. In our institution, PET/CT with 18F-FDG–labeled autologous leukocytes for which citrate has been used as the anticoagulant is now the routine method for the detection of occult infectious foci.
CONCLUSION
For the detection of focal infection, PET/CT with 18F-FDG–labeled leukocytes seems to be a highly competitive method relative to SPECT/CT with 99mTc-HMPAO–labeled or 111In-oxine–labeled leukocytes. When leukocytes are labeled with 18F-FDG, citrate is at least as effective as heparin as an anticoagulant. Unlike heparin, citrate does not increase granulocyte activation and should be the preferred anticoagulant for 18F-FDG labeling of leukocytes.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 9, 2011.
REFERENCES
- Received for publication November 23, 2010.
- Accepted for publication August 30, 2011.





{kind=link}
{kind=link}
{kind=link}