


Abstract
Recurrent falls in older people are commonly associated with abnormalities that involve several parts of the central nervous system, especially with basal ganglion pathology. The aim of the present study was to evaluate the integrity of striatal dopamine transporters (DaTs) by use of 123I-N-3-fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl)tropane (123I-FP-CIT) SPECT of striatal DaTs in patients with recurrent sudden falls. Methods: Twenty-one patients without a definite neurologic diagnosis for recurrent sudden falls were enrolled in a cross-sectional study. SPECT with a DaT ligand was performed 180 min after injection of 185 MBq of 123I-FP-CIT with a dual-head γ-camera. Results: DaT SPECT findings were normal in 15 of 21 patients (71%). Of those, 73% had abnormal MRI findings suggestive of atherosclerotic lesions. Eleven patients with normal DaT SPECT findings had mild parkinsonian symptoms. There was no correlation of the SPECT results with patient age, duration of occurrence of falls, or frequency of falls, and there was no significant difference in the relative distributions of SPECT findings between patients with and patients without parkinsonian symptoms or vascular risk factors. Conclusion: Recurrent sudden falls are, in most cases, not attributable to the degeneration of the nigrostriatal system.
Recurrent falls are a distressing and common problem in the older population, and they impose a great economic burden on health care systems (1,2). Patients with cardiovascular, vestibular, metabolic, and neurologic disorders may be at risk. One important direct cause of recurrent falls is postural instability associated with extrapyramidal disorders (3–5), especially multisystem atrophy (MSA), progressive supranuclear palsy (PSP), and late-stage Parkinson's disease (PD). However, recurrent falls may also occur in patients with high-level gait disorders (6) and in patients with postural instability but with no or only minor parkinsonian symptoms (7). Pathology studies have shown that a clinical neurologic examination is not sensitive enough to identify the cause of recurrent sudden falls (8) and that more valid tools are needed.
123I-N-3-Fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl)tropane (123I-FP-CIT) is a sensitive marker of the degeneration of the dopaminergic nigrostriatal pathway. In patients with PD and degenerative parkinsonian syndromes, SPECT imaging with 123I-FP-CIT reveals decreased uptake of a dopamine transporter (DaT) ligand, indicating an impairment of the nigrostriatal system. The aim of the present study was to evaluate the integrity of the nigrostriatal system in patients with primary idiopathic recurrent falls by use of 123I-FP-CIT SPECT. We also investigated the correlation of the SPECT results with the presence of parkinsonian symptoms in patients with abnormal findings on neurologic examination.
MATERIALS AND METHODS
Subjects
The study group included 21 patients who were 70 y old or older and who were referred to the Movement Disorders Clinic of Rabin Medical Center for the evaluation of recurrent falls that could not be attributed to a specific disease or medical condition. Prior evaluations had ruled out an orthopedic, visual, or metabolic cause. The clinical work-up included a detailed focused history and a complete structured neurologic examination, including the motor part (part III) of the Unified Parkinson's Disease Rating Scale (UPDRS). All patients also underwent a brain scan with MRI (n = 17) or CT (n = 20) or both. Patients were excluded if the cause of their falls was readily identified on neurologic evaluation as idiopathic PD, MSA, or PSP or if brain imaging revealed hydrocephalus by use of accepted diagnostic criteria (9–11). Patients with cognitive decline (Mini Mental State Examination score of <25), muscle weakness, peripheral neuropathy, signs of cerebellar involvement, history of psychiatric disease, or past use of dopamine receptor–blocking agents were excluded as well. The study was approved by the Ethics Committee of the Edith Wolfson Medical Center.
Brain SPECT Study
All patients and controls received oral potassium iodide (Lugol's solution) to block thyroid uptake of free radioactive iodide. A dose of 185 MBq of 123I-FP-CIT (DaTSCAN; GE Healthcare) was injected intravenously, and imaging was performed 3 h later. The SPECT study was performed with a dual-head γ-camera (Helix; Elscint) equipped with a low-energy, high-resolution collimator. A 20% window was centered on the 159-keV photopeak of 123I. The circular rotation mode was applied to acquire 120 frames of 15 s each into a 128 × 128 image matrix. Acquired images were transferred to a dedicated Xeleris workstation (GE Healthcare) for processing. Raw SPECT data were reconstructed with a commercially available ordered-subset expectation maximization algorithm (2 iterations, 10 subsets) and postfiltered with a Butterworth filter (cutoff frequency, 0.5; order, 10.0) (12). Attenuation was corrected on the basis of an automated ellipse determination with a constant linear attenuation coefficient of 0.11 cm−1.
Visual analysis of the data was performed by a nuclear medicine specialist who was unaware of the patients' clinical status. Tracer uptake patterns were defined according to accepted criteria (13). In addition, 123I-FP-CIT binding to the entire striatum, caudate, and putamen was calculated quantitatively and compared with striatal binding in 20 healthy, historical control subjects (12–14). Striatal binding was analyzed by the nuclear imaging specialist.
Statistical Analysis
Data were managed and analyzed with the BMDP statistical package (BMDP Corp.). An analysis of variance was used to compare age, disease duration, and SPECT values between patients and controls and between patients with and patients without parkinsonian symptoms. The Kruskal–Wallis test was used to evaluate the effects of disease duration and symmetry of parkinsonian symptoms on SPECT values. The Pearson test, the χ2 test, or the Fisher exact test was used, as appropriate, to examine the distributions of abnormal SPECT values in patients with and patients without vascular risk factors, parkinsonian symptoms, and MRI abnormalities. All tests were 2-sided and considered significant at P < 0.05.
RESULTS
The mean ± SD age of the patients was 79.0 ± 5.5 y, and the mean ± SD duration of occurrence of falls was 2.6 ± 1.6 y. Sixteen patients had vascular risk factors, that is, hypertension, diabetes mellitus, or coronary artery disease. The frequency of falls varied from less than one per month to more than one per week. Of the 17 patients who underwent brain MRI, 15 showed diffuse white matter lucency or multiple lacunar cortical and subcortical infarcts; normal findings were noted in the other 2 patients.
Fifteen patients had mild to moderate parkinsonian symptoms of tremor (n = 9), rigidity (n = 11), and bradykinesia (n = 12). Ten patients had gait abnormalities characterized by hesitant, unstable gait and slowness, but stride size was normal and the patients did not shuffle. The mean ± SD UPDRS motor score of these patients was 16.4 ± 7.7. In 7 of them, the motor symptoms were asymmetric. None of them had predominantly axial symptoms (stooped posture, head drop, or dysarthria). In fact, they did not complain of tremor or slowness, but these signs were noted on the clinical examination. The remaining 6 patients in the study sample had no parkinsonian symptoms. All patients had abnormal pull test results.
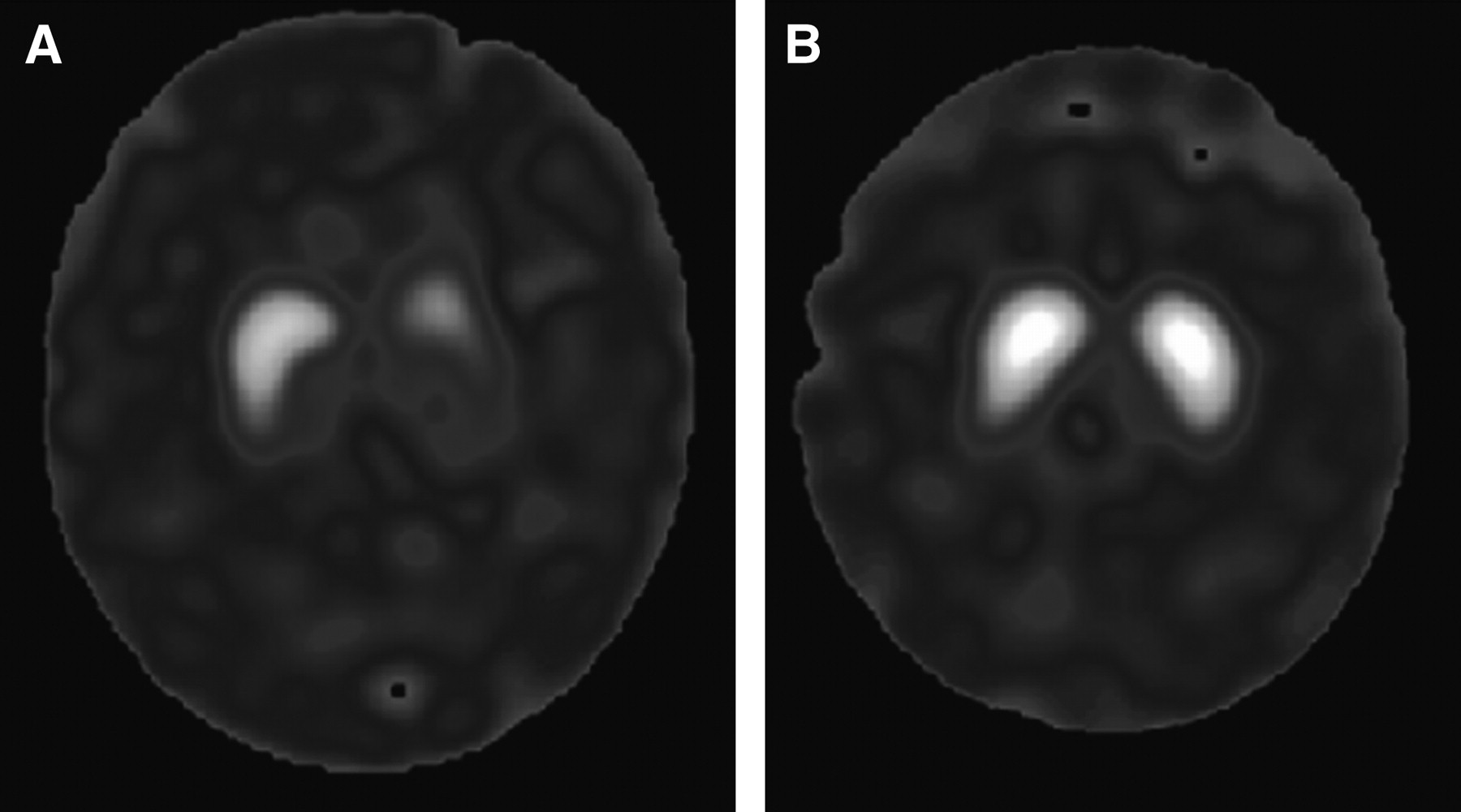
SPECT results were normal in 15 patients and abnormal in 6 patients (Fig. 1). There was no significant difference in DaT uptake in the caudate, putamen, or striatum between patients with normal scans and controls, whereas there was a significant decrease in ligand uptake in all of these areas between patients with abnormal scans and patients with normal scans or controls (Fig. 2). There was no significant difference in mean age or frequency of falls between patients with normal SPECT results and patients with abnormal SPECT results. Patients with abnormal SPECT findings showed a trend toward a longer duration of occurrence of falls than patients with normal findings, but the difference did not reach statistical significance (P = 0.09). They also had higher rigidity scores, but the difference did not reach statistical significance. There was also no correlation between SPECT findings and frequency of falls, duration of occurrence of falls, asymmetry of symptoms, tremor severity, presence of bradykinesia, or global UPDRS motor scores.
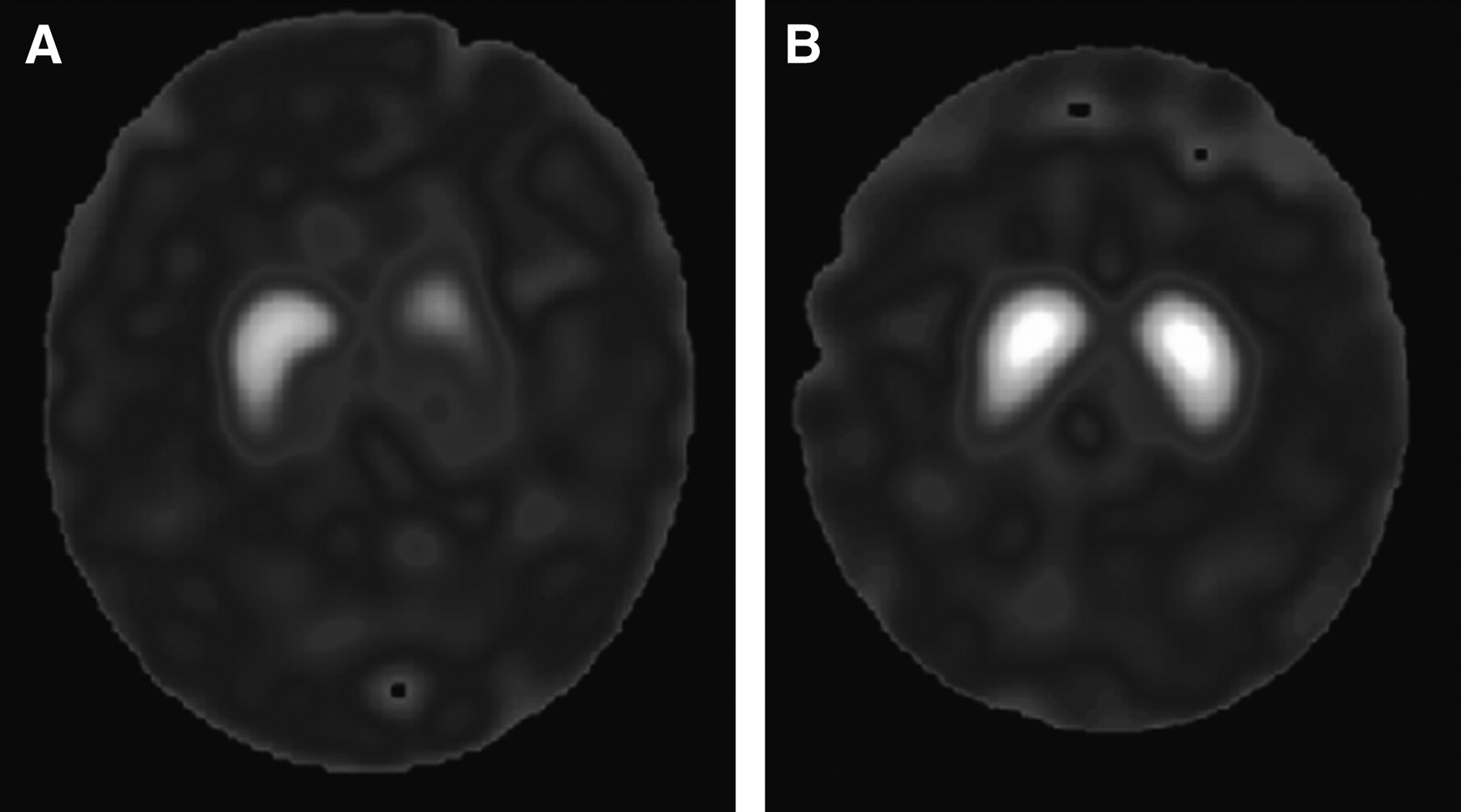
123I-FP-CIT SPECT images from 2 patients with recurrent falls. (A) 76-y-old woman with 4-y history of recurrent falls. Her neurologic examination was intact except for abnormal postural reflexes. DaT scan shows unilateral reduced striatal binding. (B) 70-y-old woman with falls during past year. On examination, she had mild symmetric tremor and bradykinesia, without rigidity. UPDRS score was 20. DaT scan shows normal striatal binding.
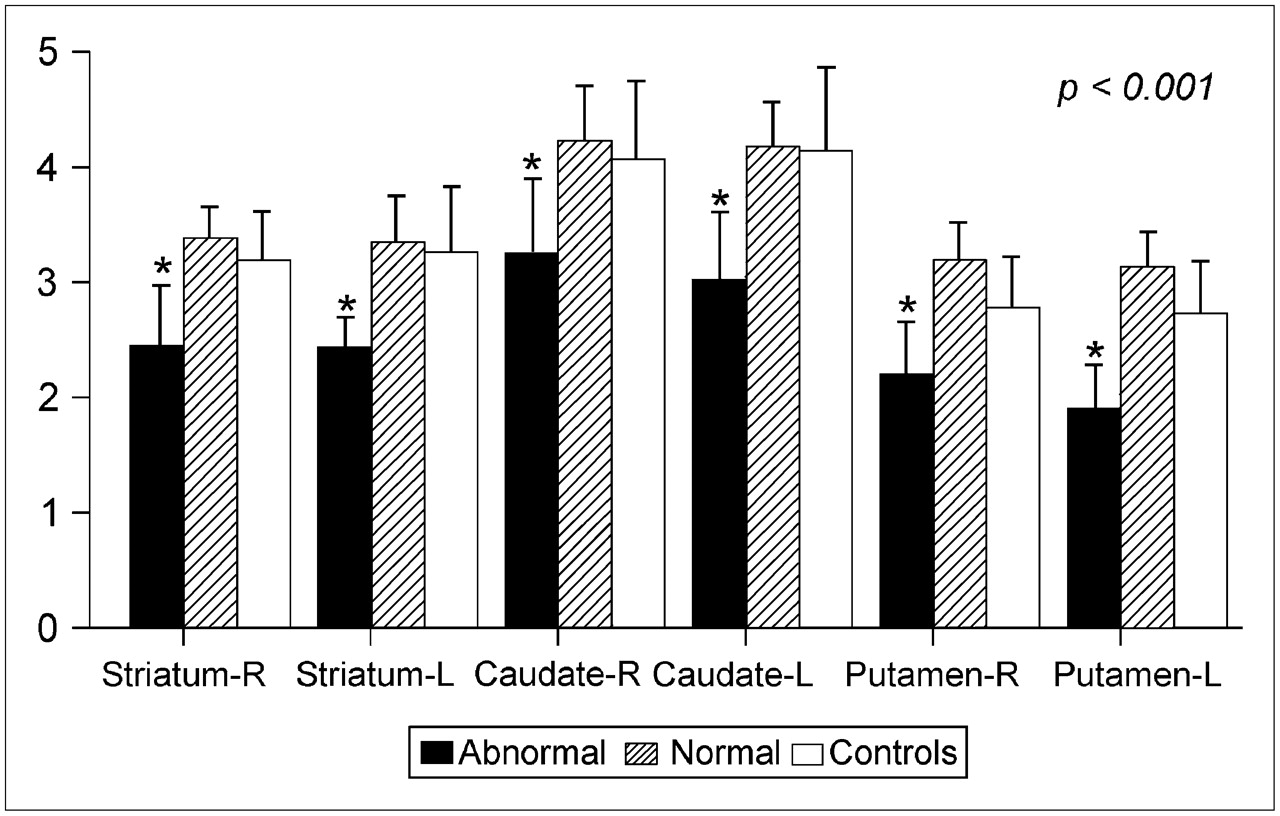
123I-FP-CIT uptake in striatum, caudate, and putamen of control subjects, patients with recurrent falls and normal SPECT findings, and patients with recurrent falls and abnormal SPECT findings. Significant decrease in ligand uptake was noted in these areas on both sides only in patients with abnormal SPECT findings. *P < 0.001.
Because recurrent falls are commonly associated with extrapyramidal neurodegenerative disorders and atherosclerotic changes, we examined the distributions of normal and abnormal SPECT results by presence or absence of parkinsonian symptoms, vascular risk factors, and MRI findings (Table 1). SPECT findings were normal in 11 of the 15 patients with parkinsonian symptoms (73%) and in 4 of the 6 patients without such symptoms (66%). Reduced DaT uptake was observed in 2 of the 6 patients without parkinsonian symptoms (33%). There was no significant difference in the relative distributions of normal and abnormal SPECT findings among these subgroups. Thirty percent of the patients with asymmetric parkinsonian symptoms had abnormal SPECT scans. Most of our patients displayed signs suggestive of ischemic changes on MRI, but there was no difference in the distributions of MRI findings between patients with normal SPECT results and patients with abnormal SPECT results. Two of 6 patients with abnormal DaT scans had small lacunar infarcts in the basal ganglia, and 5 had diffuse periventricular ischemic changes. One patient underwent only a CT scan, which showed cortical atrophy without ischemic changes. Interestingly, the patients with reduced DaT binding but with no parkinsonism were those with no vascular lesions in the basal ganglia.
Comparison of Patient Characteristics by SPECT Findings
DISCUSSION
The present study demonstrated that unexplained, recurrent sudden falls are, in most cases, not attributable to the degeneration of the nigrostriatal system and that recurrent falls are not necessarily related to any of the neurodegenerative extrapyramidal disorders (PD, MSA, or PSP), even with the presence of parkinsonian symptoms. Conversely, 2 patients without parkinsonian symptoms had reduced DaT uptake, compatible with the diagnosis of a neurodegenerative disorder. One of them acquired mild unilateral rigidity and parkinsonian facies (masklike expression), and the other is symptom free after a follow-up of 24 mo. These findings agree with those of previous studies showing that abnormal SPECT or PET findings may precede the diagnosis of PD by 3–5 y (15–17).
To the best of our knowledge, there are as yet no reported studies of the functional integrity of the nigrostriatal pathway in patients with recurrent falls and gait disturbance. In a study in which SPECT with hexamethylpropyleneamine oxime was used in patients with gait apraxia and lacunar infarcts, no difference was observed in regional blood flow in the cortex and basal ganglia between those patients and controls (18). Accordingly, in our study, DaT SPECT findings were normal in most patients. Because DaT SPECT is more sensitive and specific than SPECT with hexamethylpropyleneamine oxime for the detection of nigrostriatal system dysfunction, it may be useful for detecting abnormalities that can predict the emergence of a parkinsonian syndrome. We noted no correlation between SPECT results and patient age, duration of occurrence of falls, asymmetry of symptoms, presence of vascular risk factors, or pathologic MRI. However, the relatively small number of patients precludes a definitive conclusion.
Recurrent falls are a major hazard in the older population. In some patients, falls are accompanied by a typical high-level gait disorder, characterized by a wide stance, cautious and hesitant gait, short shuffling steps, and impaired or aberrant postural reflexes (6,19,20). This type of gait has also been variably termed arteriosclerotic parkinsonism, lower-body parkinsonism, gait apraxia, and frontal ataxia or disequilibrium (21–24). One proposed underlying mechanism of high-level gait disorders is vulnerability of the long corticospinal fibers that control leg and trunk movements as they descend close to the lateral ventricles (6). A particularly important connection is the basal ganglion outflow from the pallidum via the thalamus, which may contribute to the hypokinetic elements of gait and the rigidity that we found in our patients, even those with normal SPECT findings.
Several studies have suggested that one of the most common causes of high-level gait disorders is subcortical arteriosclerotic encephalopathy (Binswanger's disease) (23,25,26). Subcortical ischemic changes and lacunar infarcts were also demonstrated in our series, and they probably play a role in the pathogenesis of recurrent falls. However, there was no correlation between vascular lesions on MRI and SPECT findings. Moreover, 2 patients had normal MRI and normal SPECT findings. It could be argued that vascular lesions in the basal ganglia are the cause of reduced DaT binding in patients without parkinsonian signs. However, microinfarcts in the basal ganglia do not affect DaT uptake (27), and the 2 patients with no parkinsonism and reduced DaT binding did not have lacunar infarcts in this area. Together, these data suggest that mechanisms other than arteriosclerosis of subcortical arteries are involved in the pathogenesis of recurrent falls.
Functional imaging techniques exploring the density of DaTs may help to differentiate PD, a presynaptic disorder, from arteriosclerotic parkinsonism (unless there is a focal basal ganglion infarction). Indeed, parkinsonian features in patients with recurrent falls can yield an incorrect diagnosis of PD, MSA, or PSP and lead to unnecessary treatment with dopaminergic medications. According to the literature, nearly 10% of patients diagnosed with PD by neurology specialists are found on postmortem examination to have evidence of a lacunar state without characteristic PD pathology (8). On the other hand, the abnormal SPECT findings in 2 of our patients who did not have parkinsonian symptoms indicate that recurrent falls are, in some cases, the presenting symptom of an extrapyramidal disease and that DaT SPECT is more sensitive than a clinical examination for the early detection of the disease. These patients did not have lacunar infarcts in the basal ganglia (in one patient, only a CT scan was performed). In 2 other patients who had abnormal SPECT findings and who underwent MRI, there were no ischemic lesions in the basal ganglia; therefore, we do not believe that lacunar infarcts are the direct cause of parkinsonian signs but rather that they have an indirect effect on the pathogenesis of a distinct neurodegenerative disease. Conversely, it should be noted that normal SPECT findings do not absolutely rule out an extrapyramidal syndrome, and longer-term follow-up of patients is warranted to reach a final diagnosis. Our findings suggest that a clinical examination is not sufficient to establish the presence of an extrapyramidal disorder and that the diagnosis should be based on clinical, anatomic, and functional neuroimaging examinations.
CONCLUSION
DaT SPECT does not reveal a decrease in ligand uptake in most patients with recurrent falls. This finding implies that the cause of recurrent falls in these patients is not a neurodegenerative extrapyramidal disease and that idiopathic falls may represent a distinct neurodegenerative entity. Vascular leukoencephalopathy plays a major role in their occurrence. DaT SPECT can improve diagnostic skills for patients with recurrent falls and allow for better management.
Acknowledgments
This study was supported by a research grant from GE Healthcare; by the National Parkinson Foundation, USA; and by the Alan and Norma Aufzien Chair for Research in Parkinson's Disease, Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 9, 2007.
- Accepted for publication June 13, 2007.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.