


Abstract
PET has emerged as a powerful diagnostic tool for the evaluation of cancer patients. Currently, most of these studies are performed with the glucose analog 18F-FDG, which has been shown to accumulate avidly in most tumors. 18F-FDG PET is now routinely used in the diagnosis, staging, and posttherapy evaluation of oncologic patients. After reading this paper, the reader should understand the physiologic basis of using 18F-FDG in patients with different tumors, describe the role of this radiopharmaceutical in the management of oncologic patients, and identify those malignancies for which 18F-FDG has proved to be effective in diagnosis and follow-up.
Metabolic imaging has recently become a reality in clinical practice. 18F-FDG is by far the most widely used positron-emitting radiopharmaceutical used for PET imaging. The estimated number of PET studies in the United States grew from 69,000 in 1998 to 155,000 in 2000 (1).
Several factors have contributed to the proliferation of this technology. First, 18F-FDG PET has shown clinical usefulness in a variety of scenarios (mostly oncology and, to a lesser extent, cardiology and neurology). Second, recent advances such as the development of sodium iodide–based PET cameras have made the technology more affordable, which has caused 18F-FDG to become more widely available from commercial pharmacies. A third factor was the 1998 decision of the Center for Medicare and Medicaid Services to expand coverage to 5 major indications (lung cancer, head and neck cancer, colorectal cancer, melanoma, and lymphoma).
This article reviews the oncologic clinical applications of 18F-FDG imaging, discusses the rationale behind its use, and describes its usefulness for different malignancies.
18F-FDG as a Positron Emitter
18F, a cyclotron-produced radionuclide with a half-life of 110 min, is usually obtained by bombarding 18O-water with a proton to obtain 18F from an [18O (p,n) 18F] reaction. After production of this radioisotope, the next step is integration of the 18F into the glucose molecule in position 2, yielding 18F-fluoro-2-deoxyglucose. The details of this complex process have been described elsewhere (2).
18F-FDG competes with “normal” glucose to be incorporated into the cell by a membrane carrier–facilitated transport mechanism (usually by glucose transporter 1 protein, which is located in the cell membrane). Once inside the cell, 18F-FDG is phosphorylated into 18F-FDG-6-phosphate, which remains trapped because it is a polar compound that cannot be further metabolized. The 18F-FDG-6-phosphate molecule can be dephosphorylated to 18F-FDG by the enzyme glucose-6-phosphatase. This process will be slower in cancer cells than in nonmalignant cells because the former have relatively low levels of this enzyme (3).
18F-FDG in Clinical Oncology
The transport and phosphorylation of 18F-FDG to 18F-FDG-6-phosphate occurs at a higher rate in cancer cells than in normal cells. This is thought to be mostly caused by relatively higher levels of glucose transporters and possibly the action of the enzyme hexokinase (4). Because of this relatively increased avidity of neoplastic cells for glucose, 18F-FDG will accumulate at higher rates in tumor cells than in nonneoplastic cells (5) and is the basis for using 18F-FDG as a tumor marker in current clinical practice. By collecting tomographic data using either a dedicated PET scanner or a modified SPECT gamma camera with coincidence capability, one can obtain functional information to differentiate benign from malignant conditions (6).
Although 18F-FDG PET or SPECT imaging has been investigated for a wide variety of tumors, PET is currently recommended by the Society of Nuclear Medicine only for detecting and localizing unknown primary tumors, differentiating malignant from benign tissues, staging and evaluating recurrence, differentiating recurrence from postsurgical changes, and monitoring the response to therapy (7).
Patient Preparation
For diagnostic-quality images, patients should have fasted for at least 4 h before the study, and blood sugar levels should be within the reference range. These requirements are especially important in diabetic patients, in whom high glucose levels can alter the distribution of 18F-FDG. When plasma glucose levels are greater than reference values, 18F-FDG uptake increases in muscles, with subsequent blurring of tumor margins; in contrast, glucose use by most types of cancer does not seem to depend on plasma glucose levels. Therefore, more 18F-FDG is taken up by cancer cells when the extracellular concentration of glucose is low, enhancing tumor detectability (8). Usually 185–555 MBq (5–15 mCi) are injected intravenously 45–60 min before scanning. Emission and transmission scans are acquired following different protocols, each one designed for the type of tumor to be studied and the clinical question to be addressed. For assessment of regional disease, detailed imaging of a region of the body is recommended, and attenuation correction is usually needed (e.g., detection of mediastinal lymph node involvement in lung cancer). However, for screening for metastatic disease, whole-body imaging may be more appropriate (e.g., presurgical evaluation of patients with recurrent colorectal cancer).
Clinical Applications
Lung Cancer.
Lung cancer is the leading cause of death from cancer and one of the most diagnosed malignancies worldwide, with an estimated 178,100 cases and 160,400 deaths per year in the United States alone (9). Prognosis depends mainly on histologic type and stage at initial diagnosis.
For clinical purposes, lung cancer is divided into the small cell and non–small cell types. Small cell lung cancer is typically central, with extensive mediastinal adenopathy, and is strongly associated with smoking. Non–small cell lung cancer refers to 3 types of histologically different tumors: adenocarcinoma, usually peripheral, with early development of metastases and, commonly, malignant pleural effusion; squamous cell (epidermoid) carcinoma, usually central, with late development of distant metastases and more related to smoking; and large cell carcinoma, commonly a large, peripheral mass. Early-stage non–small cell lung cancer is usually treated surgically, with resection of the primary tumor and mediastinal lymph nodes. Late-stage cancer (when lymph node metastases are present on the opposite side of the chest or distant metastases are present in the liver, adrenals, or other organs) is usually treated with radiotherapy, chemotherapy, or a combination of both. Currently, no surgical curative approach has become widely accepted for small cell lung cancer, which is basically treated with chemotherapy and radiation therapy (10,11).
18F-FDG PET is used in the initial staging of newly diagnosed lung cancer and has been proven superior to CT or MRI in the evaluation of lymph node metastases (Table 1) and distant metastases (Fig. 1). The 18F-FDG PET study guides the final therapeutic approach because it differentiates surgical from nonsurgical candidates by accurately depicting the clinical stage (12–15). In addition, PET is especially useful when one is assessing the presence of adrenal metastases, up to 78% of which can be missed by CT or MRI (16,17).
18F-FDG PET vs. CT in Mediastinal Lymph Node Staging of Lung Cancer

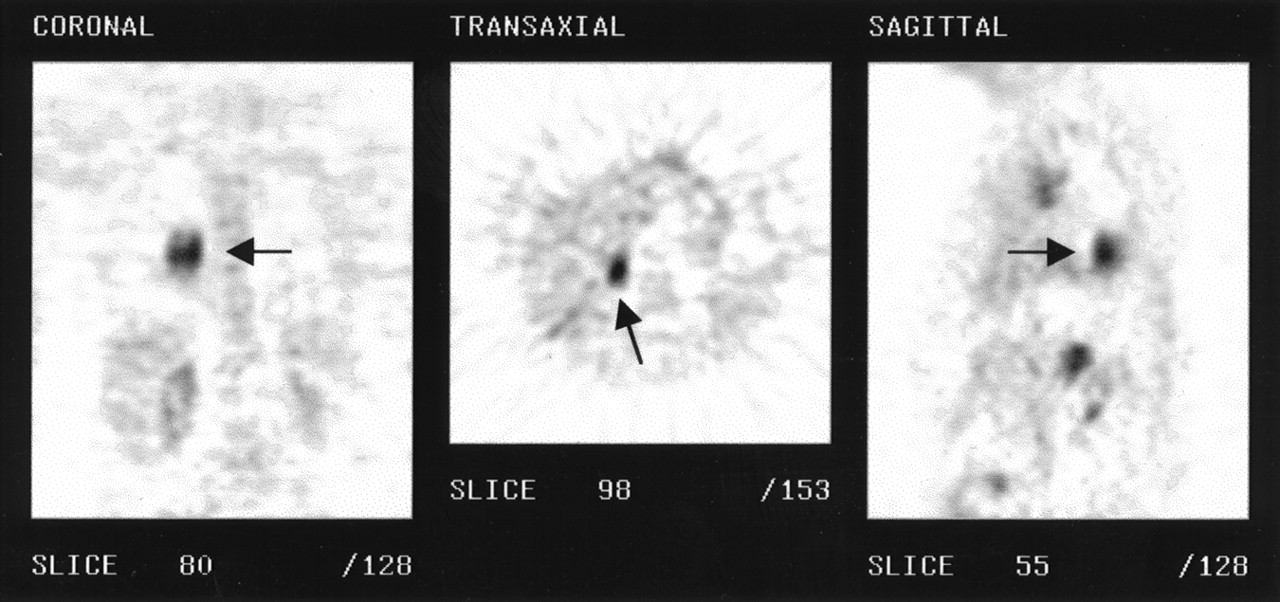
Patient with history of carcinoma of left lung with left axillary lymph node metastases. 18F-FDG PET depicted other unsuspected metastatic sites in both axilla (arrow, right panel) and paratracheal nodes (arrow, center panel).
Preliminary results also suggested a potential role for 18F-FDG in assessing the response to therapy or in following up lung cancer. Increased or persistent 18F-FDG uptake focally in lesions that had been previously treated is usually indicative of residual or recurrent neoplasia (18).
Single Pulmonary Nodule.
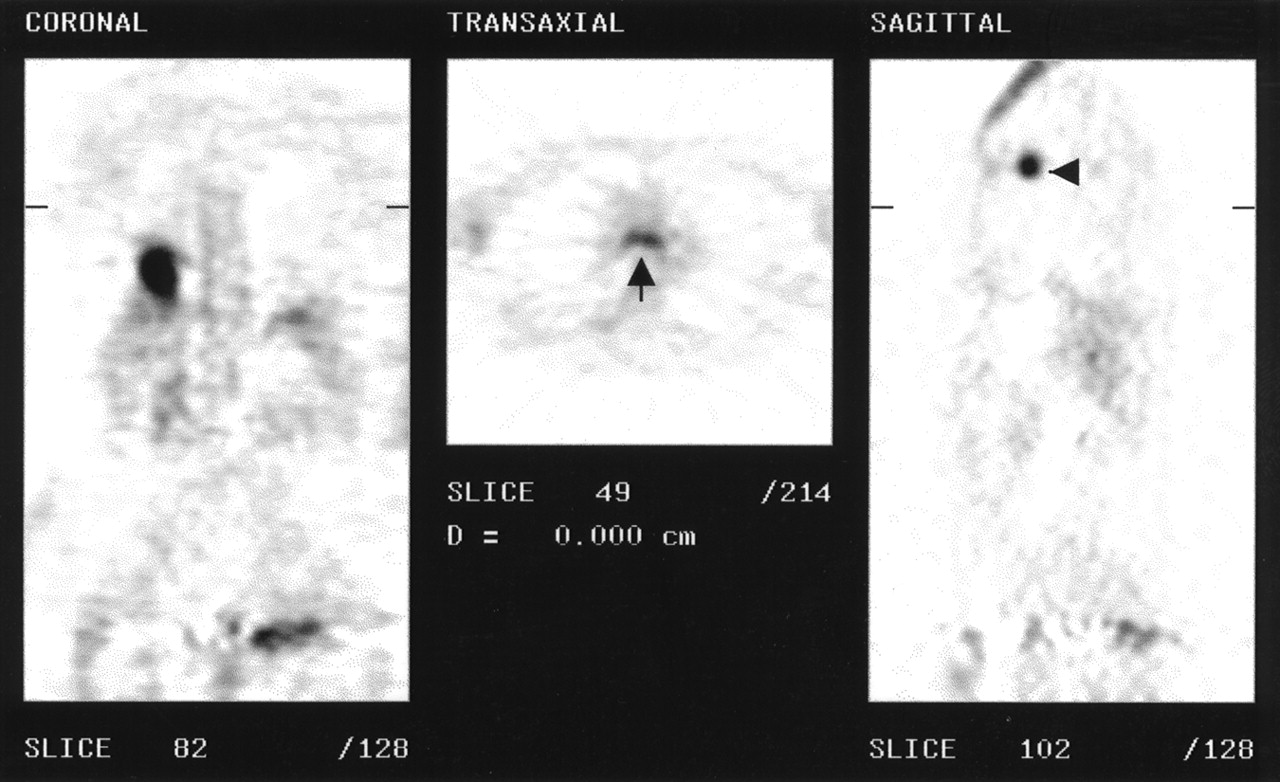
Incidental masses discovered by chest radiography or CT can be evaluated with 18F-FDG (Fig. 2). An increased metabolic rate in single pulmonary nodules has been shown to strongly indicate malignancy. In a prospective evaluation of patients with single pulmonary nodules, 18F-FDG PET yielded a sensitivity of 90% and a specificity of 83% for detecting neoplastic lesions. The main source of false-positive findings was tuberculosis, and the most frequent area was the right upper lung (19).
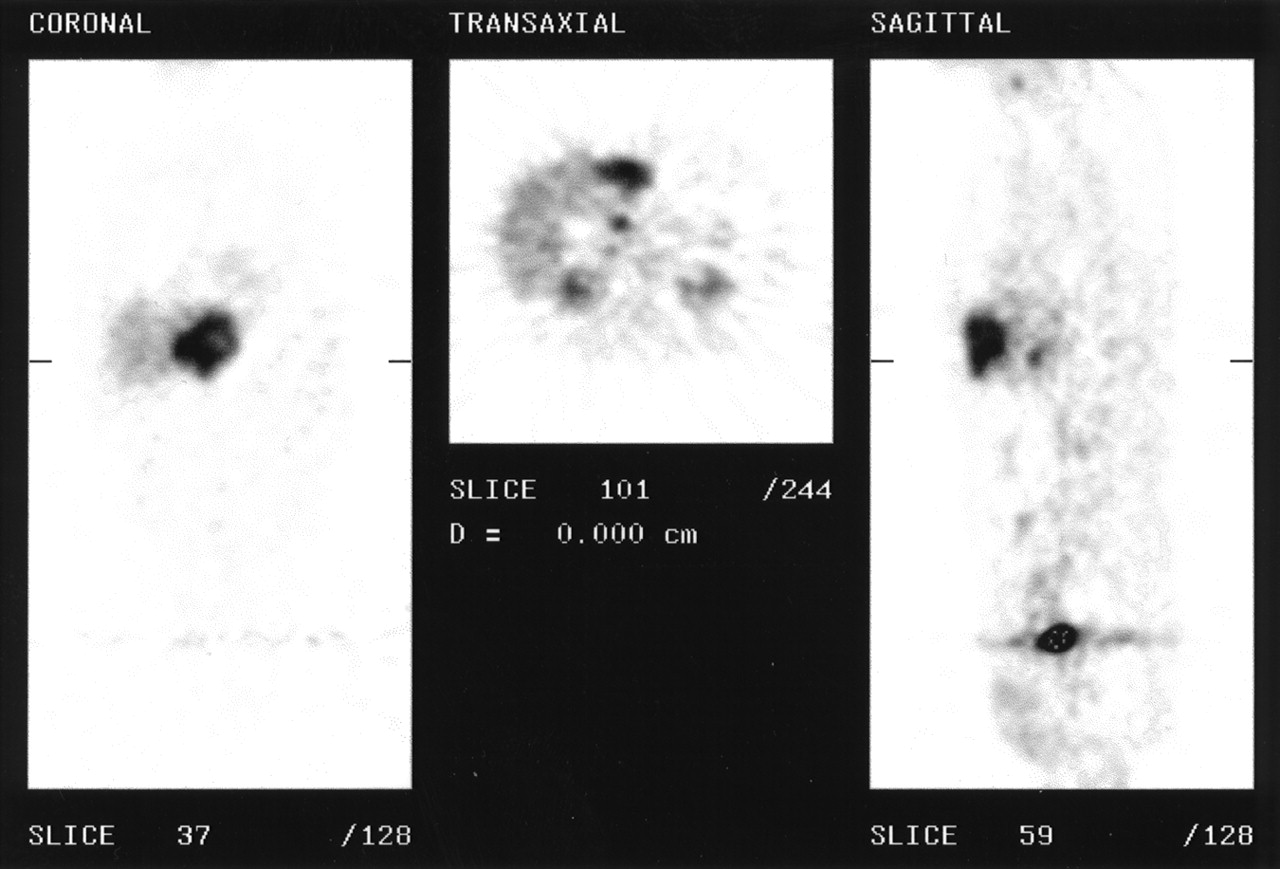
Patient with right lower lobe nodule on CT (not shown) and adrenal mass on right side. 18F-FDG PET shows primary neoplasm in right lower lobe (arrow, left and right panels) and right adrenal gland metastases (arrow, middle panel).
Quantitative analysis can be performed using a standard uptake value, which can be calculated by dividing the mean activity in the region of interest drawn around the lesion (MBq/mL) by the injected dose (MBq) divided by the body weight (g):
 . Tracer uptake is determined from a small region of interest placed over the tumor as seen on an attenuation-corrected image. Because 18F-FDG is not taken up by adipose tissue, the standard uptake value is more reproducible when the lean body mass (derived from measurements of both height and weight) is substituted for patient weight in the formula above.
. Tracer uptake is determined from a small region of interest placed over the tumor as seen on an attenuation-corrected image. Because 18F-FDG is not taken up by adipose tissue, the standard uptake value is more reproducible when the lean body mass (derived from measurements of both height and weight) is substituted for patient weight in the formula above.
Using this quantitative approach, Lowe et al. (20) found a cutoff point of 2.5 to be an accurate indicator of malignancy. More interestingly, characterization of single pulmonary nodules with 18F-FDG PET and CT has been reported to be the most cost-effective strategy, with yearly national potential savings of $62.7 million (21).
Cancer of Colon and Rectum.
Colorectal cancer is one of the most common cancers in the United States. Approximately 130,000 cases are diagnosed each year. After resection for cure of the primary tumor, 55% of these patients will experience recurrence, mostly to the liver, which is the major site of metastatic involvement 30% of the time (22). Before any surgery is planned, patients should be accurately screened for extensive disease to avoid unnecessary operations and exposure to possible postsurgical complications. CT has a sensitivity of approximately 85% for depicting liver involvement and 33%–94% for detecting extrahepatic sites of metastatic involvement such as lymph nodes or omentum. Because of these limitations, a significant number of patients thought to be candidates for curative resection will be found to have nonresectable disease during surgical exploration. The addition of an 18F-FDG PET whole-body scan to the presurgical evaluation of these patients improves candidate selection because of higher sensitivity for liver extension (95%–100%) and extrahepatic involvement (33%–94%) (23,24).
PET can also clarify abnormal CT findings (Fig. 3) and may depict unsuspected metastases (25). This modality can find unidentified sites of disease in patients with abnormal carcinoembryonic antigen levels (a tumor marker) and a negative work-up with conventional diagnostic modalities (26). Indeed, metabolic imaging with 18F-FDG in patients with colorectal cancer has been proven to be a cost-effective technique that often alters patient management. Valk et al. (23) found per-patient average savings of $3,003 when PET was added to the diagnostic work-up of patients with colorectal cancer before surgery; 18F-FDG scanning was able to differentiate patients with nonresectable (extensive) disease from patients with resectable disease, thus avoiding unnecessary surgical procedures (e.g., liver or lung resection). Table 2 shows the number of patients whose management was changed because of PET findings, resulting in better patient management and health care cost savings.
18F-FDG PET in Surgical Management of Patients with Colorectal Cancer
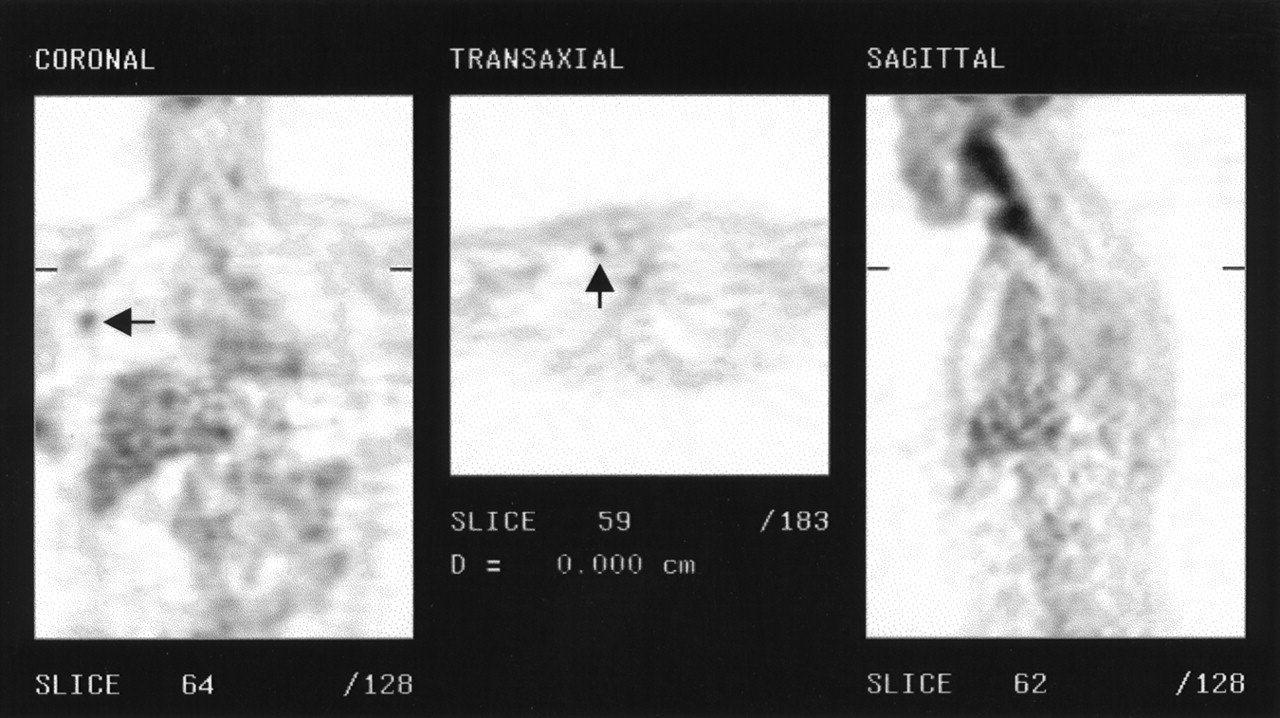
18F-FDG PET in presurgical staging of patients with colorectal cancer and hepatic metastases. This patient presented with history of adenocarcinoma of sigmoid colon and large liver lesion found on CT. PET showed liver metastases but no disease elsewhere. Patient was then considered for liver resection.
Lymphoma.
This malignancy arises from T or B lymphocytes (immune cells) and accounts for <8% of all malignant tumors. Lymphomas are classified as Hodgkin’s disease (HD) and non-Hodgkin’s lymphoma (NHL). HD is less frequent than NHL and, at an early stage, is usually confined to lymph node territories, with progression to extralymphatic organs in more advanced stages. HD primarily involves intrathoracic structures, limited to the upper mediastinum in most cases, and usually presents as enlargement of supradiaphragmatic lymph nodes with or without associated symptoms. NHL is usually widespread at the time of presentation, extending outside the lymphatic territories and commonly involving bone marrow, which heralds a poor prognosis (27).
67Ga-citrate whole-body imaging has been the method of choice in the work-up of patients with newly diagnosed HD and NHL. However, in an increasing number of patients the disease is not gallium avid. 18F-FDG PET has proven to be a cost-effective way of staging these tumors, being equal or superior to CT for detection of nodal and extranodal involvement (28,29). Also, 18F-FDG PET has been found to detect significantly more abnormal regions than has 67Ga in staging HD, suggesting more extensive disease (30).
The results of a multicenter European trial that was presented at the 46th annual meeting of the Society of Nuclear Medicine compared 18F-FDG PET with CT for primary staging of malignant lymphoma in 93 patients. 18F-FDG PET showed significantly more negative and positive correct findings for both HD and NHL. More interestingly, in the NHL group, 18F-FDG PET was significantly more accurate for extranodal disease (31).
Another advantage of 18F-FDG PET over 67Ga is better visualization of small tumors. PET can also depict central tumor necrosis better than CT. In suspected central nervous system involvement, 18F-FDG PET can also be used to differentiate between inflammatory lesions and tumor extension—an issue that can be difficult in HIV-positive patients (32).
Finally, PET can successfully evaluate tumor viability after chemotherapy and radiation therapy, allowing the clinician to reassess patient treatment. CT cannot distinguish between viable tumor and fibrosis or scar tissue. However, increased 18F-FDG uptake in equivocal masses discovered by CT has an accuracy of >90% for tumor viability (33).
Melanoma.
The incidence of this cutaneous malignancy has steadily increased over the past decade. It is estimated that 1 of 74 newborns in the United States, will develop melanoma during his or her lifetime. A multimodality approach is the usual option for treatment and includes either immunotherapy or surgical excision of the primary lesion followed by chemotherapy, depending on the extent of the disease (34). Although several positron emitters have been studied for melanoma, 18F-FDG is the most widely used because malignant melanoma has one of the highest 18F-FDG uptakes of all tumors (35). Whole-body 18F-FDG PET has a reported sensitivity of 92% and a specificity of 77% for screening for metastases from malignant melanoma and is also indicated when lymph node involvement is suspected (36,37).
Head and Neck Cancer.
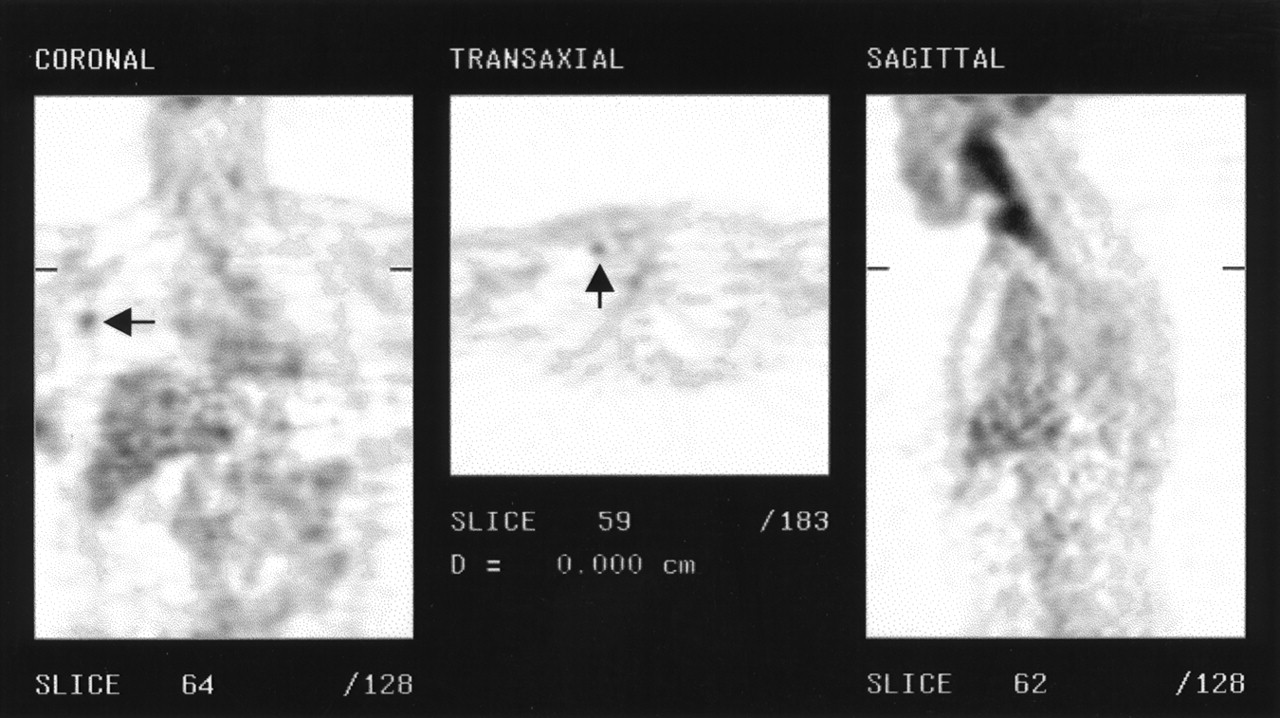
Head and neck cancer comprises approximately 4% of all newly diagnosed cases of cancer. Most of these tumors are squamous cell carcinoma originating from mucosal structures (38). These tumors usually have a poor prognosis, and accurate initial staging is mandatory before any surgical intervention is planned. Particular attention to whether the disease has spread to lymph nodes on the same or opposite side of the neck is of major importance. The location of spread dictates whether the lymph nodes will be excised from one or both sides of the neck. PET has been found to have a sensitivity of 86% and a specificity of 87% for locating the primary tumor. Moreover, 18F-FDG imaging is more accurate for detecting local lymph node involvement and distant metastatic disease (Fig. 4) (39). Recently, whole-body 18F-FDG PET has also been found to produce significant net cost savings by allowing avoidance of unnecessary surgery or radiotherapy in unsuspected distant recurrence (23). 18F-FDG PET has also been found useful for the detection of occult primary carcinoma in patients presenting with neoplastic involvement of lymph nodes in the head and neck (40).
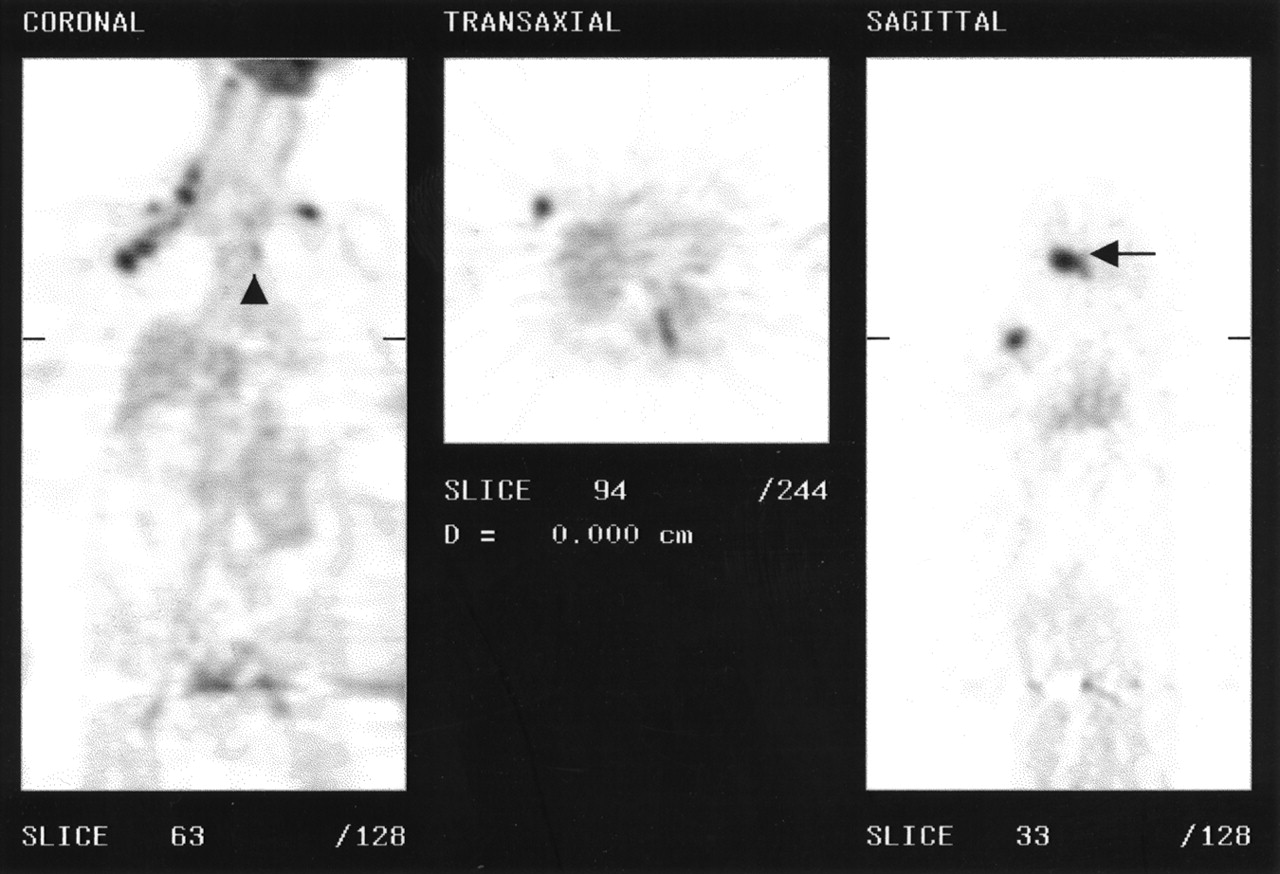
Patient with history of squamous cell carcinoma of oropharynx who was sent for PET scan to assess response to treatment. PET scan showed 2 new lesions: 1 intrapulmonary (arrow, middle panel) and 1 in right upper ribs (arrow, left panel). In addition, primary tumor appeared unchanged.
Other Applications.
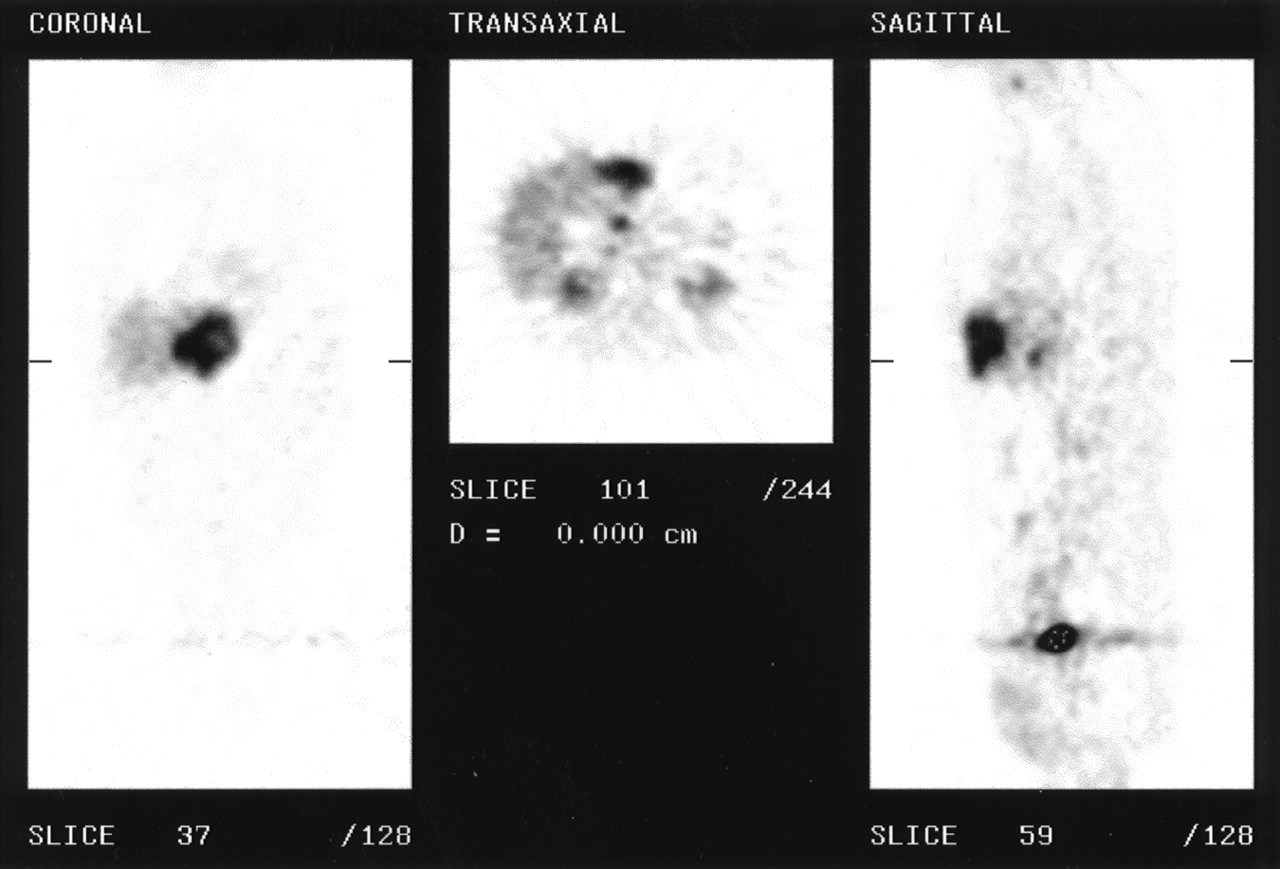
Breast cancer is the most common malignancy in women and comprises 18% of all gynecologic cancer. In recent years, its incidence has been noted to be rising, in part because of an increased number of early detection programs (41). Axillary lymph node metastasis is perhaps the single most important prognostic factor in breast cancer (42). 18F-FDG PET has been shown to have variable results for axillary lymph node staging, with an accuracy ranging from 69% to 95%, and therefore cannot be used as a substitute for lymph node dissection (43–47). However, 18F-FDG PET is superior to bone scintigraphy in detecting osteolytic bone metastases (48). This better detection may allow more accurate staging and assessment of response to therapy (49) or may aid in developing new treatment strategies (Fig. 5).
PET in staging of breast cancer. This patient presented with newly diagnosed breast carcinoma with suspected liver metastases. In addition, PET showed extensive lymph node involvement in right axilla (arrow), neck (bilaterally), and mediastinum (arrowhead).
The second most common gynecologic cancer is ovarian cancer, with an incidence of approximately 10 cases per 10,000 women in western countries. Because of the high proportion of women in whom disease has spread beyond the ovaries at the time of diagnosis, the survival rate is still disappointingly low (50). Therefore, early diagnosis and accurate assessment of tumor extension at initial presentation is extremely important. Hubner et al. (51) found a 93% sensitivity and an 82% specificity when evaluating patients with primary ovarian cancer using 18F-FDG PET. More recently, PET has been shown to improve the diagnostic accuracy of sonography for evaluating asymptomatic ovarian masses (52) and performed better than CT for detecting suspected recurrence, although the detection of microscopic peritoneal disease remains a challenge (53).
18F-FDG PET has also been used for other types of cancer. In general, PET has been reported to affect patient management and aid in the characterization of abnormal findings by other imaging modalities. These results are summarized in Table 3. Although 18F-FDG does not have a well-established role in bladder, prostate, kidney, and endocrine gland tumors, research is ongoing and the role is expected to clarify.
18F-FDG PET in Other Malignancies
CONCLUSION
Since the time that PET evolved from the research setting to the clinical setting, most studies have been performed with 18F-FDG. This radioactive glucose analog has been able to provide important information in different clinical settings, especially in oncology. Although initially regarded as an expensive test, 18F-FDG PET supplies the clinician with functional and metabolic information not available from any other tool used clinically. Increased 18F-FDG production at a lower cost, in conjunction with technical developments in camera design and manufacturing, is expected to make this test more widely available and probably to lower its cost. Active research with other positron-emitting compounds, such as 11C-choline, 18F-acetate, and 11C-methionine, is already taking place at several institutions. Thus, technologists who are currently involved in conventional nuclear medicine imaging will likely sooner, rather than later, be working with 18F-FDG imaging.
Acknowledgments
The authors thank Elpida S. Crawford, director of the nuclear medicine technology program; Fred Covelli, senior staff assistant; and Dr. Mohei Abou Zied for their help with preparing the manuscript.
Footnotes
For correspondence or reprints contact: Hani A. Nabi, MD, PhD, Department of Nuclear Medicine, State University of New York at Buffalo, 105 Parker Hall, 3435 Main St., Buffalo, NY 14214.
E-mail: hani{at}nucmed.buffalo.edu
REFERENCES





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Fifty Years of Radiopharmaceuticals
- Paraneoplastic thrombus or relapse of a pulmonary artery sarcoma?
- Reduction of the Ring Size of Radiolabeled Lactam Bridge-Cyclized {alpha}-MSH Peptide, Resulting in Enhanced Melanoma Uptake
- High-Contrast PET of Melanoma Using 18F-MEL050, a Selective Probe for Melanin with Predominantly Renal Clearance
- 99mTc- and 111In-Labeled {alpha}-Melanocyte-Stimulating Hormone Peptides as Imaging Probes for Primary and Pulmonary Metastatic Melanoma Detection
- Utility of 18F-FDG PET in Evaluating Cancers of Lung
- 3'-18F-Fluoro-3'-Deoxy-L-Thymidine: A New Tracer for Staging Metastatic Melanoma?
- Direct Imaging of Exercise-Induced Myocardial Ischemia With Fluorine-18-Labeled Deoxyglucose and Tc-99m-Sestamibi in Coronary Artery Disease
- Glucose Metabolism in Cancer: EVIDENCE THAT DEMETHYLATION EVENTS PLAY A ROLE IN ACTIVATING TYPE II HEXOKINASE GENE EXPRESSION